


|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Immediate Implant Placed at the Site of the Lower 2nd Molar Reduces Neurovascular Complication
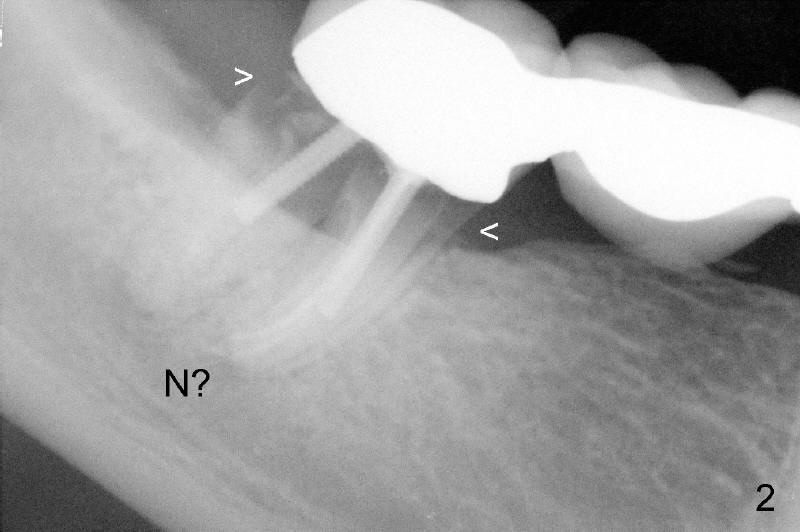
A Caucasian lady in her forties has had a bridge (Fig.1: #29-31). It looks ok 2 years ago. Recently, the bridge is loose. The posterior abutment has root fracture (Fig.2 <). The best option is extraction and implant placement at the sites of #30 and 31. Her lower jaw is small. Where is the inferior alveolar nerve under this 2nd molar (N)?
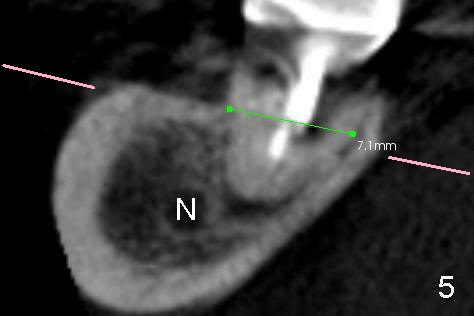
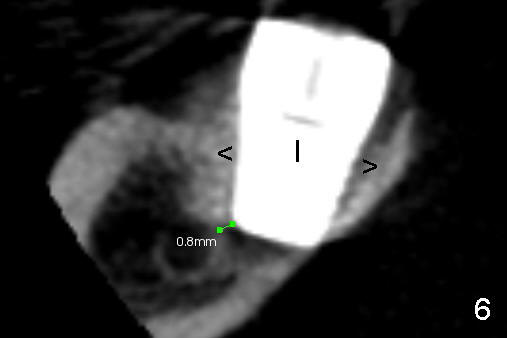
Preop coronal section of CBCT shows that the inferior alveolar nerve (Fig.5 N) is buccoapical to the apex of the 2nd molar, which is 7 mm wide buccolingually. With slow and careful bone expansion technique using osteotomes and taps, a 7x11 mm immediate implant is placed (Fig.6 I: post op CT). It is .8 mm away from the nerve. The bone buccal and lingual to the implant is condensed and displaced (>). Although the lingual plate over the submandibular fossa may have undergone green stick fracture, there is no intra and post-ostop neurovasculuar complication.
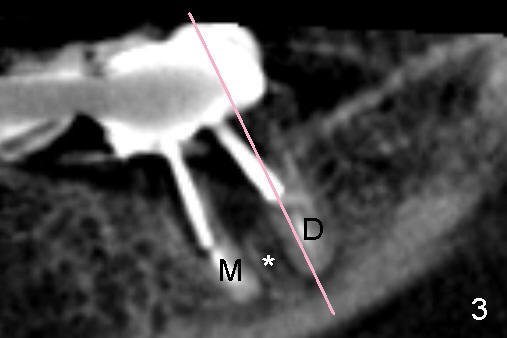
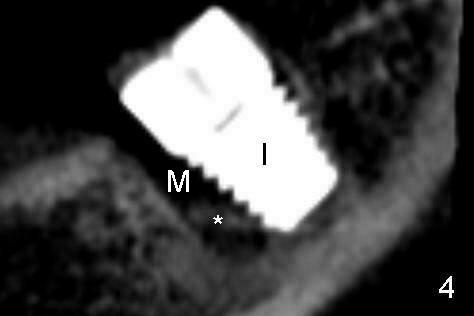
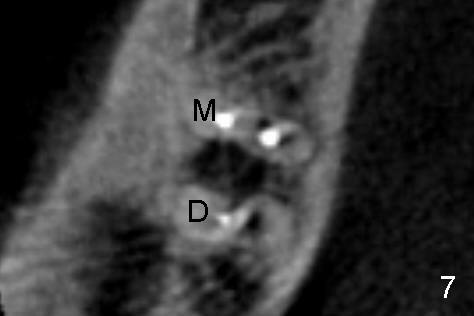
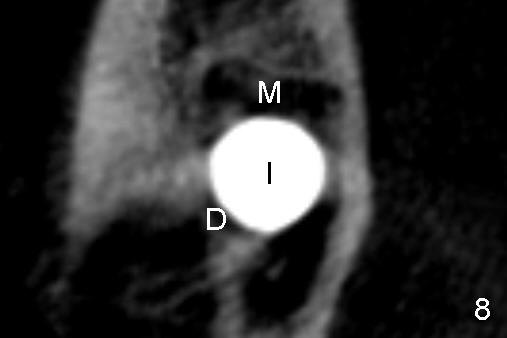
In fact the implant is placed mainly in the distal socket (Fig.4 with the septum pushed mesially (*), as compared to preop image (Fig.3)). The axial images show the same (Fig.7,8).
Although the patient is fearful, she is co-operative. In order to reduce the chance of nerve injury, infiltraton anesthesia is administered. In case the nerve is being approached, the patient may send us signal of severe pain.
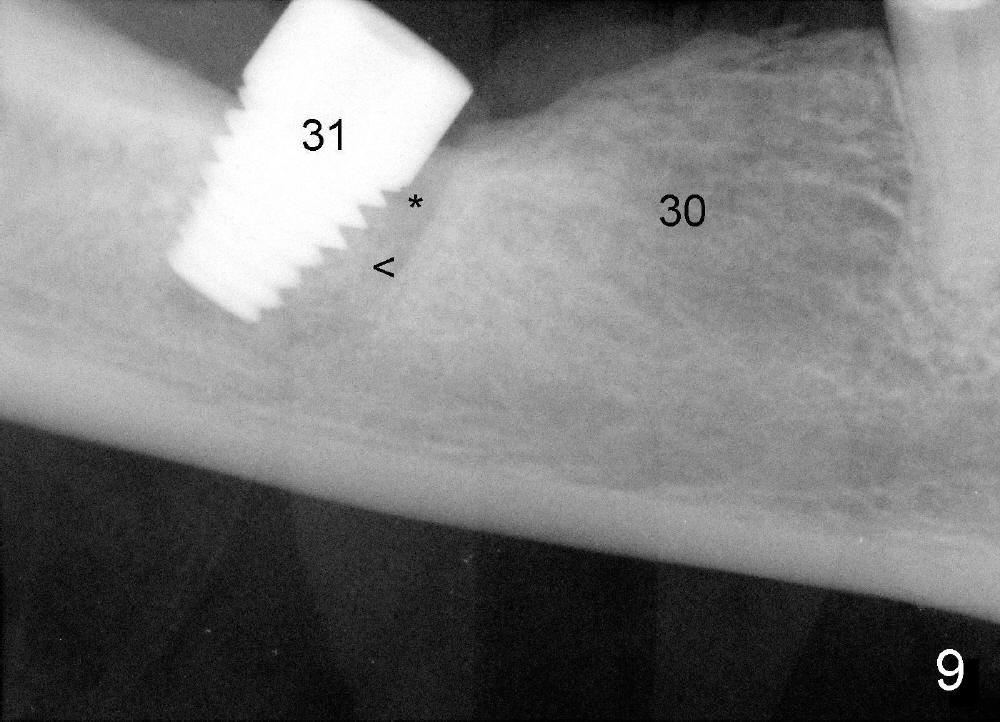
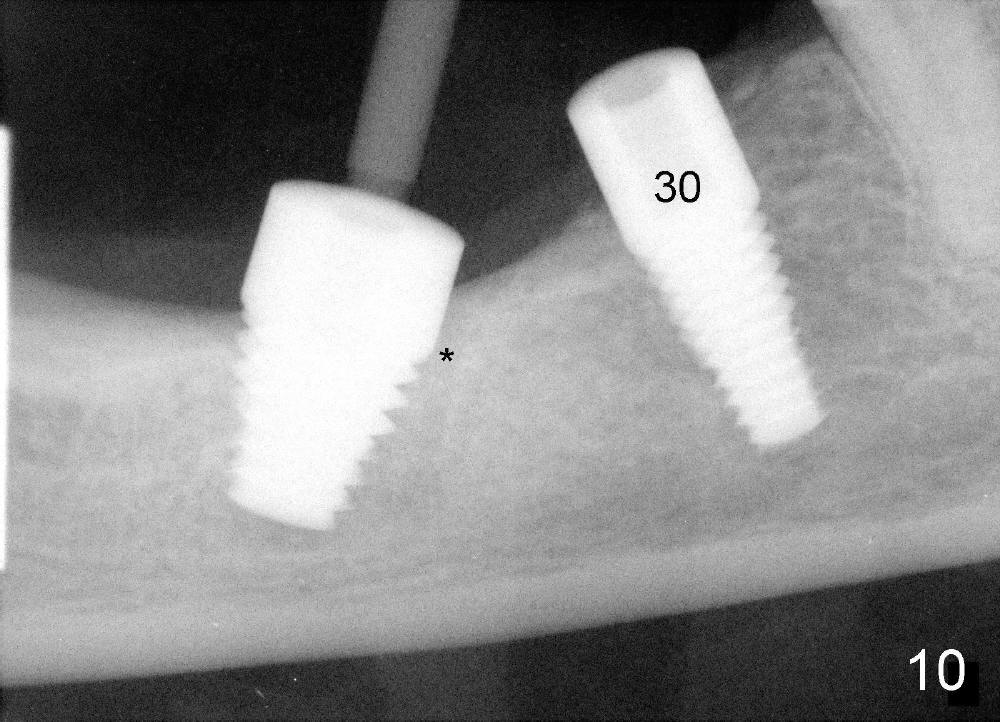
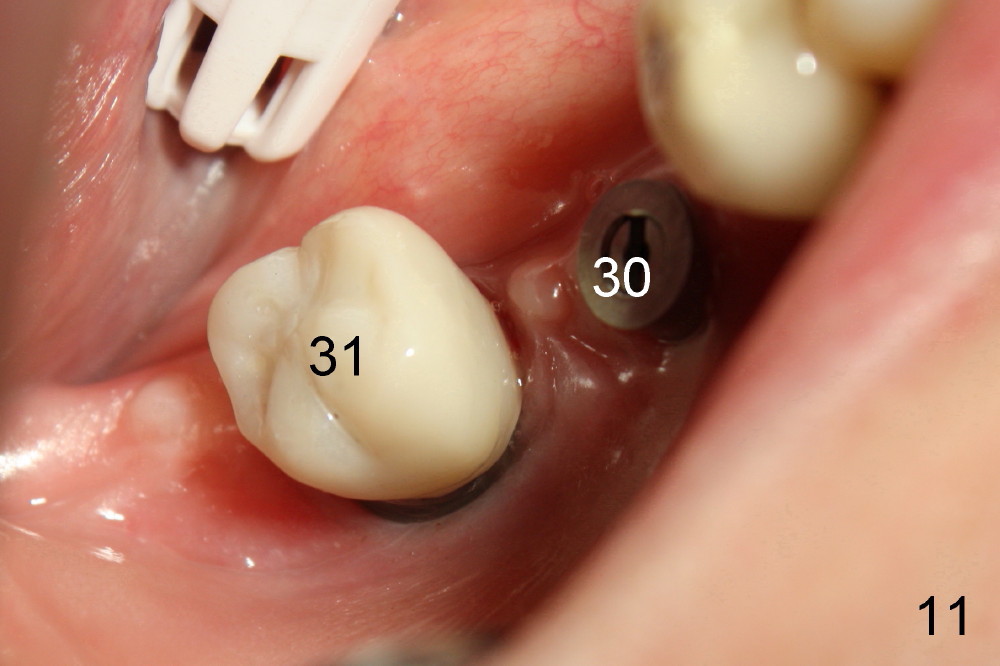
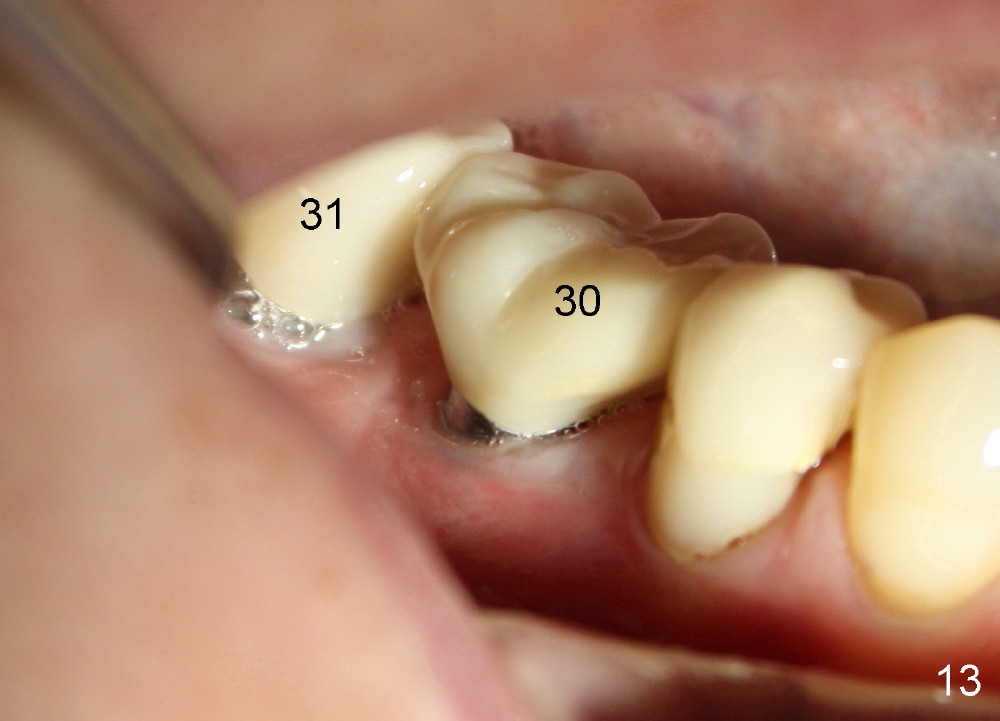
PA in Fig.9 shows that the implant is just placed at the site of #31. Bone (<) is compressed into the bottom half of the mesial socket (*). Four and a half months later when a second implant is placed at the site of #30, the top half of the mesial socket is apparently filled by new bone (Fig.10 *). The implant is very sturdy. Two months later, the implant at the site of #31 has a crown (Fig.11). The bone density increases (Fig.12 *, 3 months after Fig.10, 1 month after Fig.11). Bone keeps growing around the implant. The patient reports that she can chew better because of this implant. After the crown for the implant at the site of #30 is cemented (Fig.13), she reports that she chews even better.
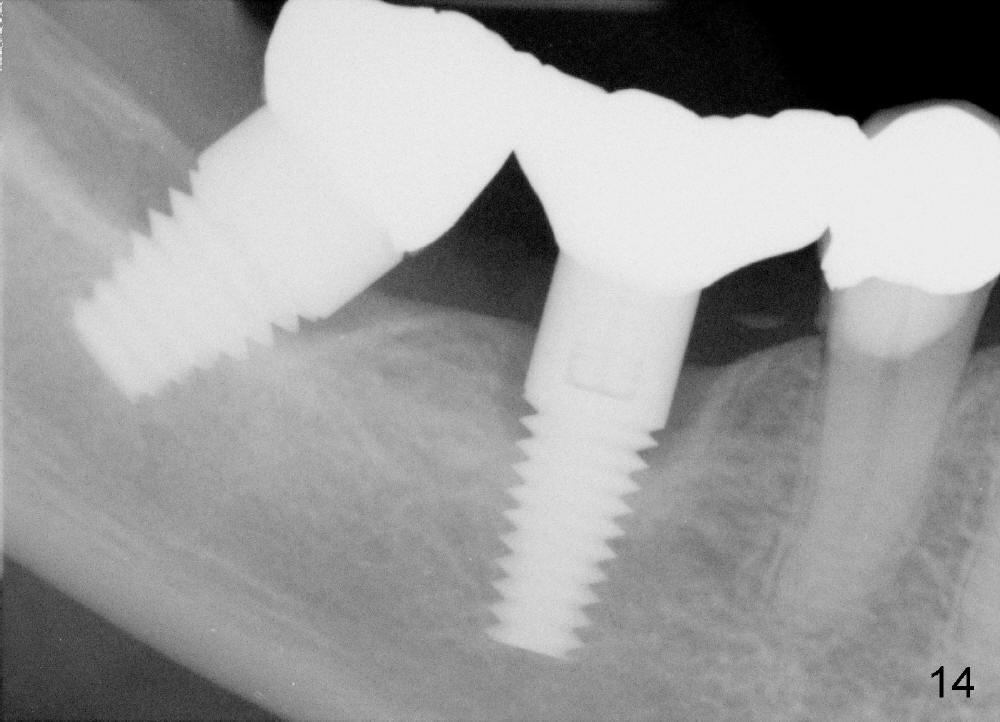
The patient returns 1 year 6 months post cementation of #30. Hard and soft tissues appear normal around the two implants (Fig.14,15). To reduce buccal implant exposure, the implant at #18 will be smaller and to be placed a little more lingually.
Immediate Implant Safety Issues, Introduction to Immediate Implant, Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 08/22/2012, last revision 10/24/2015