


|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Short Implant (3)
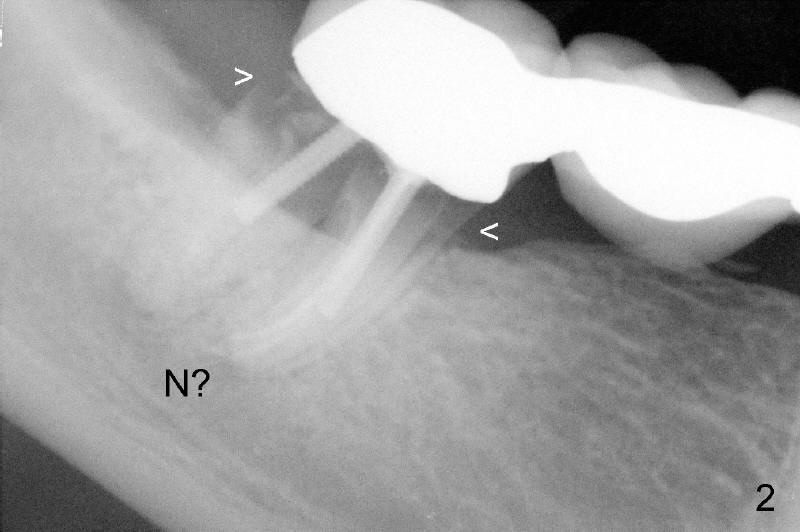
Susan has had a bridge (Fig.1: #29-31). It looks ok 2 years ago. Recently, she finds that the bridge is loose. New X-ray shows one of bridge supporting teeth (#31) has a problem (Fig.2). Two roots of this tooth are broken (<). The tooth should be extracted and replaced by an implant. But her lower jaw is small. Where is a big nerve (N) under this 2nd molar in regular 2-dimensional X-ray? Usually the root tips of 2nd molar is the closest to the nerve. Implant surgery in this area is risky.
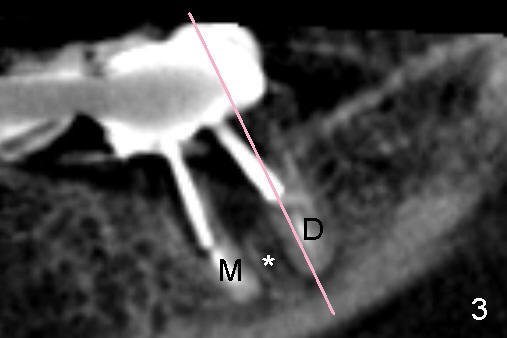
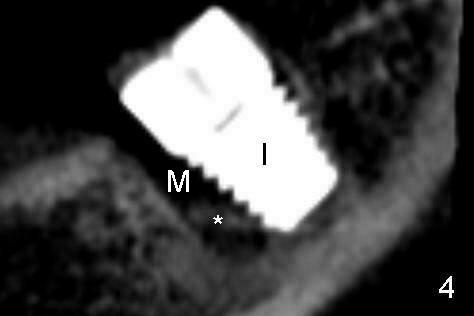
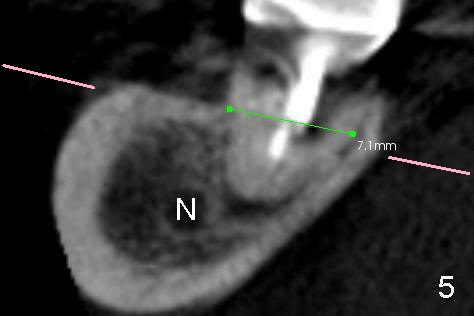
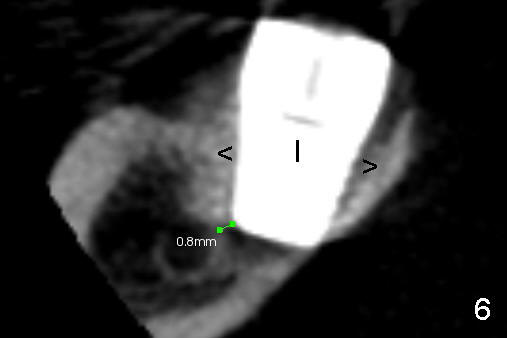
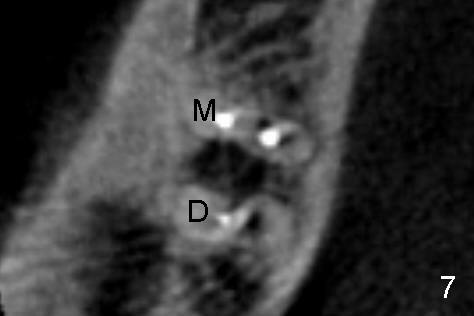
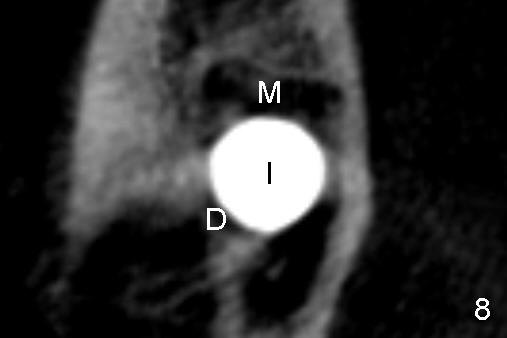
Three-dimensional (3-D) CT is taken before surgery. Fig.3 is a thin 3-D image in the same orientation as Fig.2. There is a bone structure (septum, *) between the two roots (mesial (M) and distal (D)). No nerve is found in this image. Let us make a section as the pink line across the distal root. The new 3-D section shows the nerve (Fig. 5: N) close to the root tip of the distal root. Although the root is short, it is quite wide: 7.1 mm. So a short, but wide implant is chosen (Fig.4,6,8: I). Drilling, bone expansion with chisels and placing the implant is confined to the septum and above the root tips. Injury to the nerve is minimized. In fact the edge of the implant is about 0.8 mm from the nerve (Fig.6). But there is no sign of nerve trauma after surgery.
The implant is placed mainly in the distal socket, pushing the septum (Fig. 4: *) into the mesial socket (M). The pink lines in Fig.5 indicate the section level for Fig.7 (before) and 8 (after).
Although the patient is fearful, she is co-operative. In order to reduce the chance of nerve injury, we do not anesthetize her jaw too deeply on purpose. In case the nerve is being approached, she may send us signal of severe pain. She bears certain amount of pain during the surgery. Because of her cooperation, the implant is placed a little deeper (to increase implant stability) without touching the nerve grossly. The second reason for implant stability is tight contact between the wide implant and socket (Fig.6). In fact the implant compresses the bone around it (>), making the bone look whiter (denser).
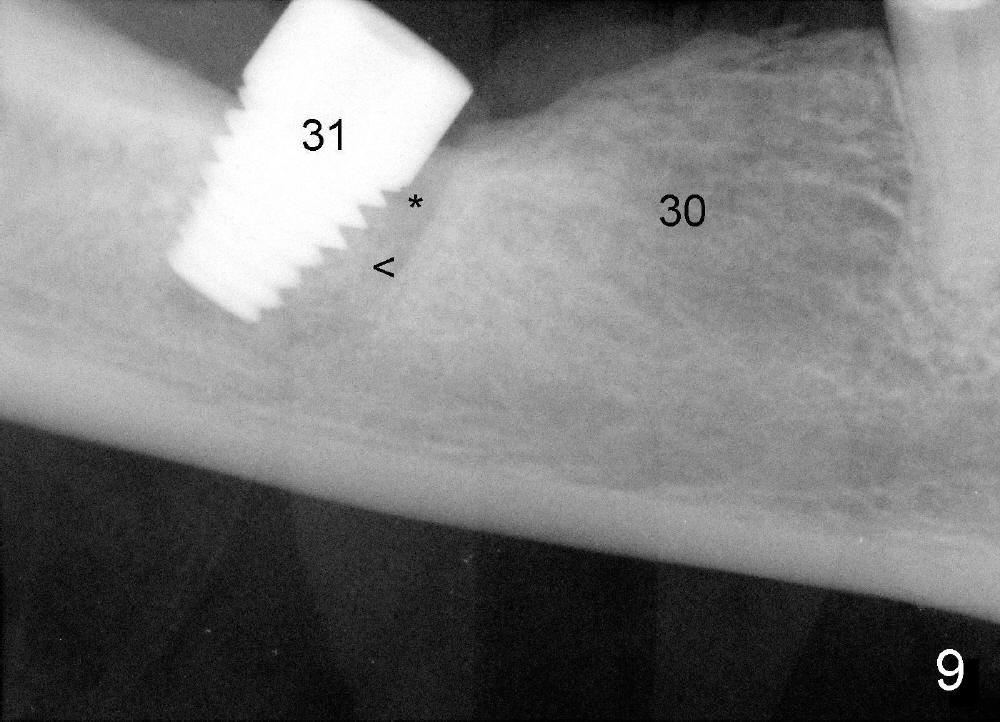
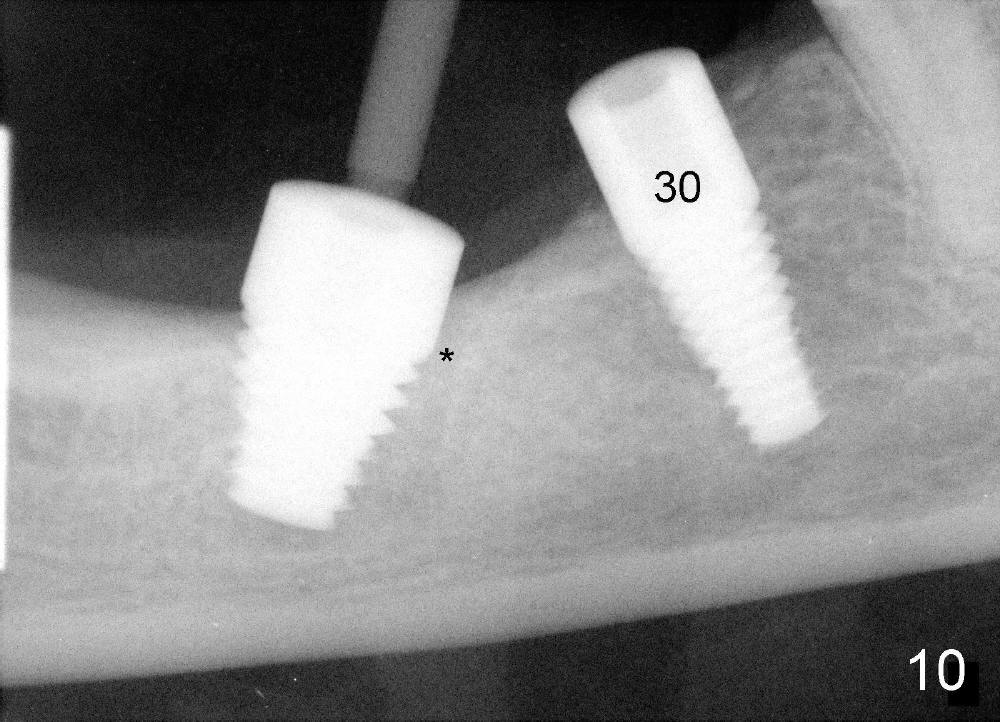
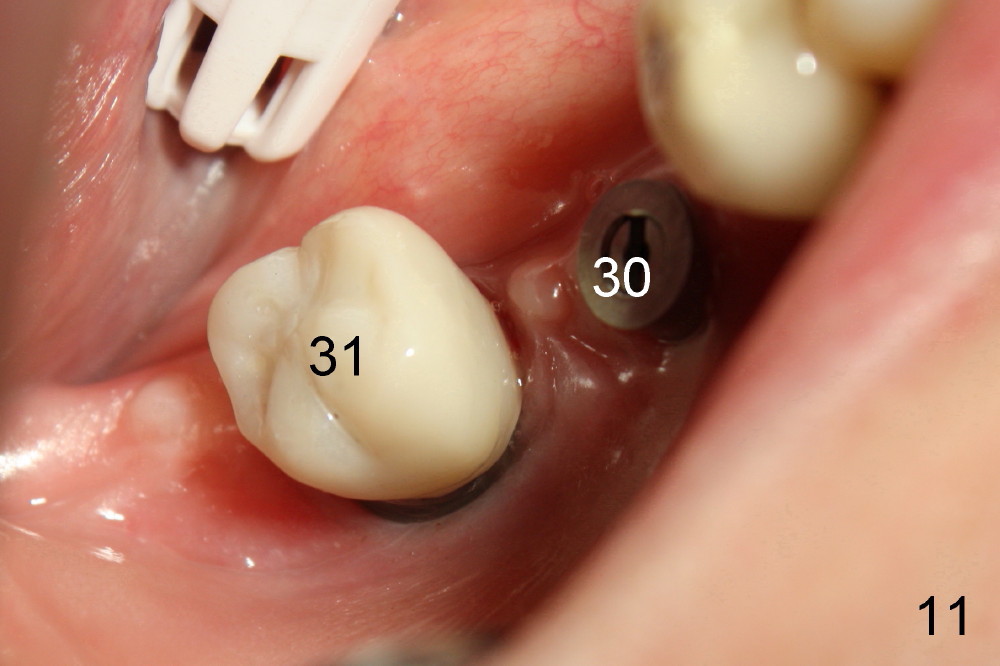
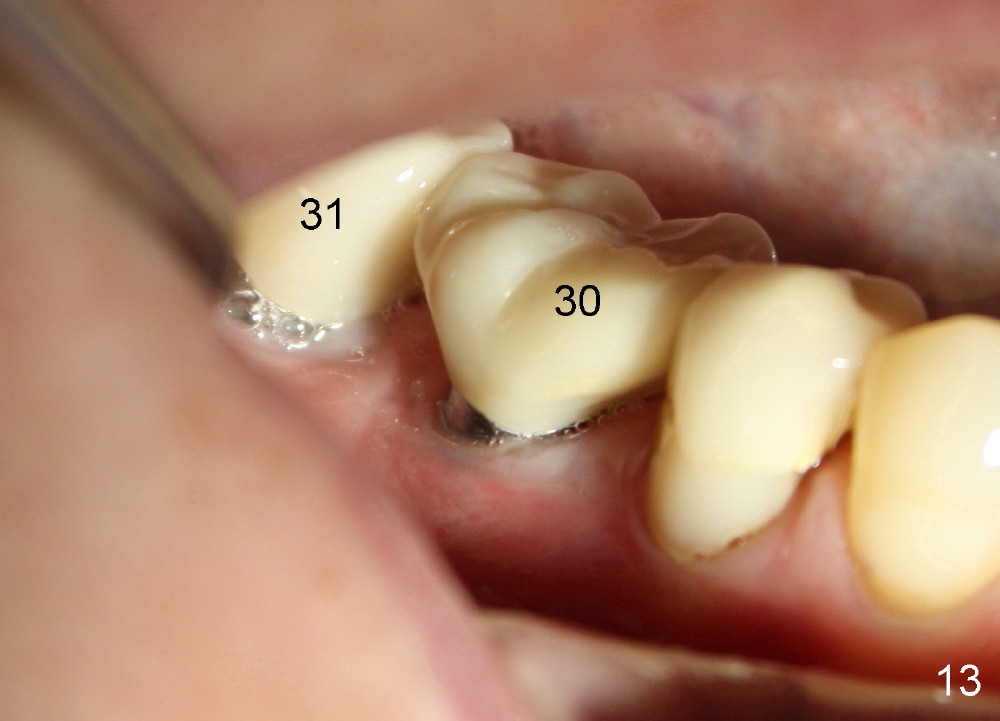
Regular X-ray in Fig.9 shows that the implant is just placed at the site of #31. Bone (<) is compressed into the bottom half of the mesial socket (*). Four and a half months later when a second implant is placed at the site of #30, the top half of the mesial socket is filled by new bone (Fig.10 *). The implant is very sturdy. Two months later, the implant at the site of #31 has a crown (Fig.11). The bone density increases (Fig.12 *, 3 months after Fig.10, 1 month after Fig.11). Bone keeps growing around the implant. The patient reports that she can chew better because of this implant. When we cement the crown for the implant at the site of #30 (Fig.13), she is going to chew even better. Her gums are pinkish and healthy due to her meticulous oral hygiene.
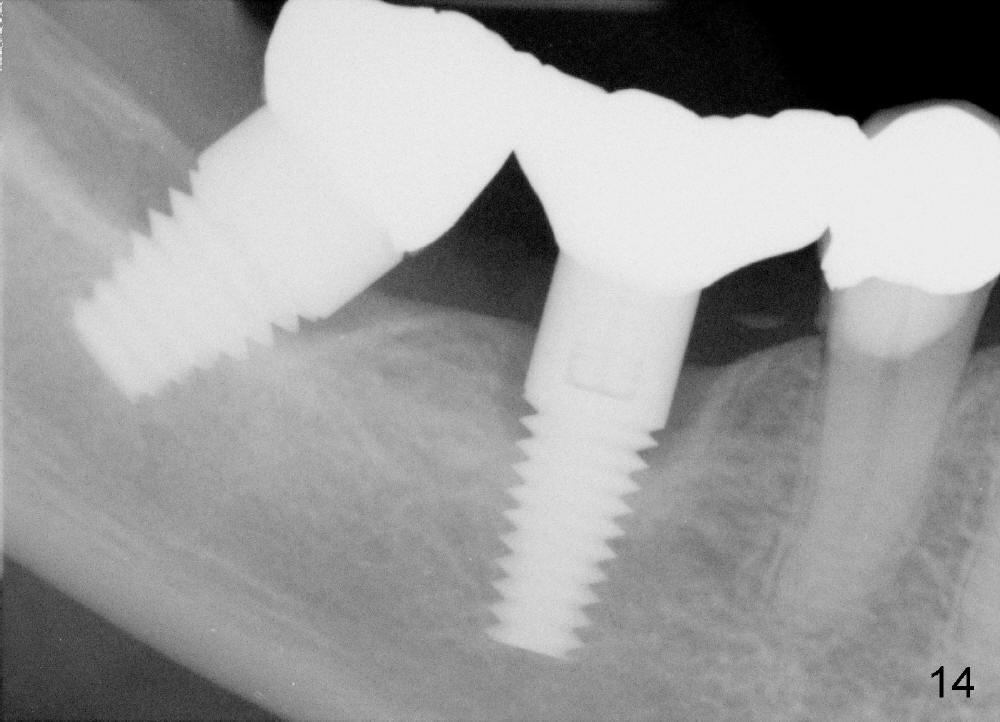
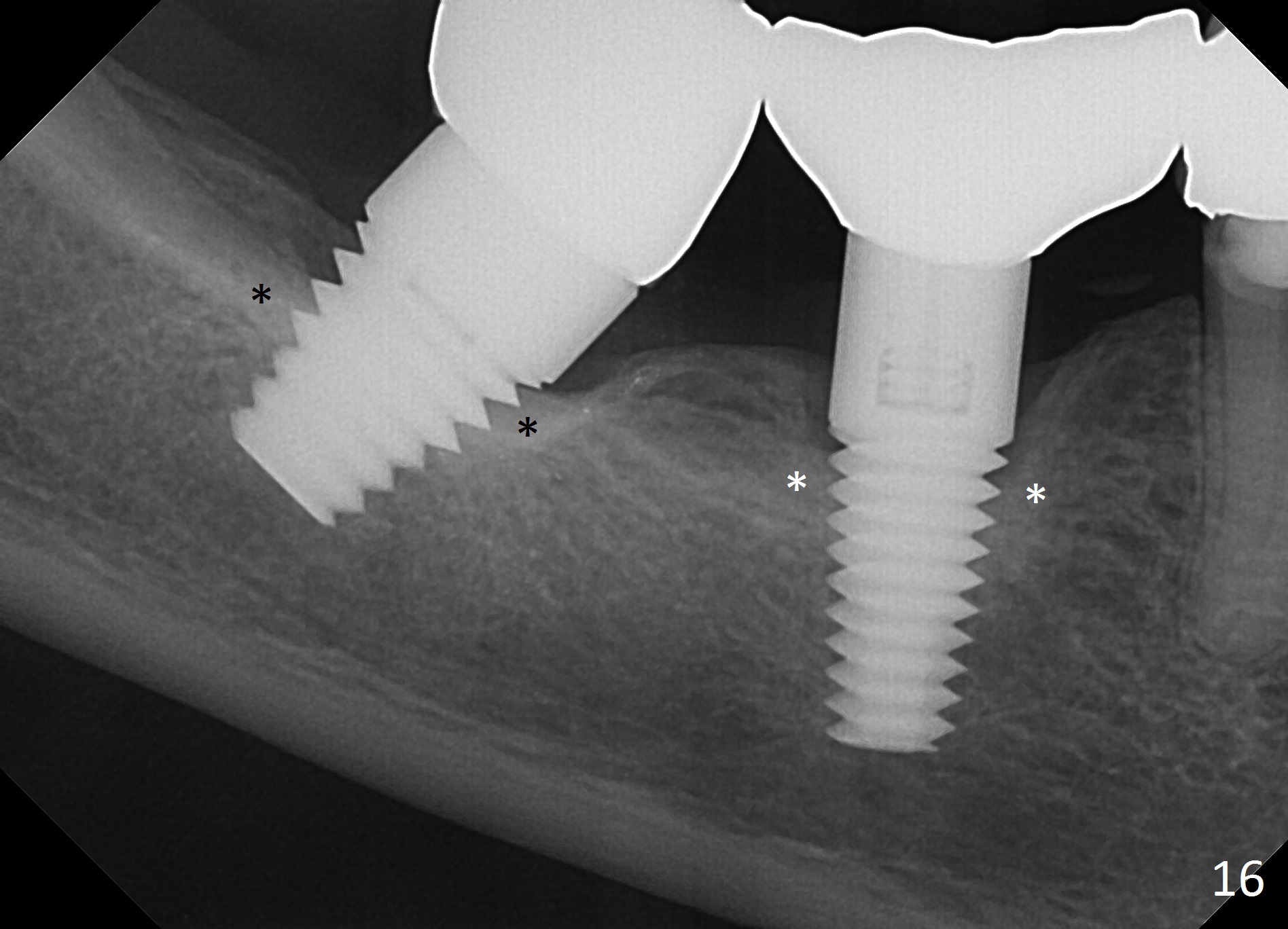
The patient returns for follow up 1.5 years after cementation of #30 crown (Fig.14,15). Hard and soft tissues around implants look normal. Bone is dense around the implants 4 years after crown cementation (Fig.16 *).
Xin Wei, DDS, PhD, MS 1st edition 08/22/2012, last revision 05/04/2017