Treatment Plan for Anterior Immediate Implants
-
52 y/o, Smoker; when he comes back for surgery, ask him whether he has
smoked less or not. Smoking is associated with higher risk of implant
failure
-
He has advanced chronic periodontitis. Scaling & root planing has been
done. Ask him whether he has brushed more or not and whether he
flosses or not
-
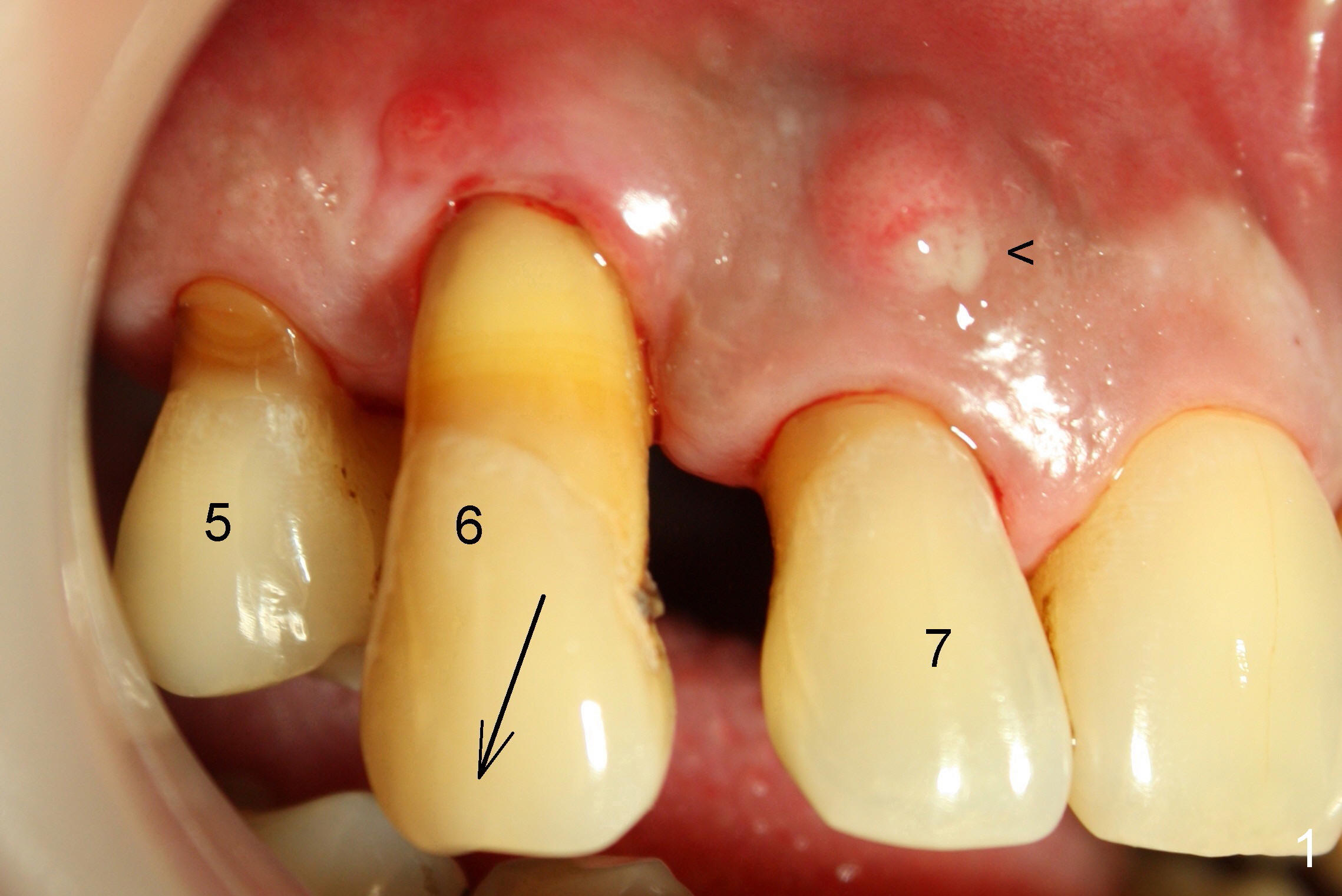
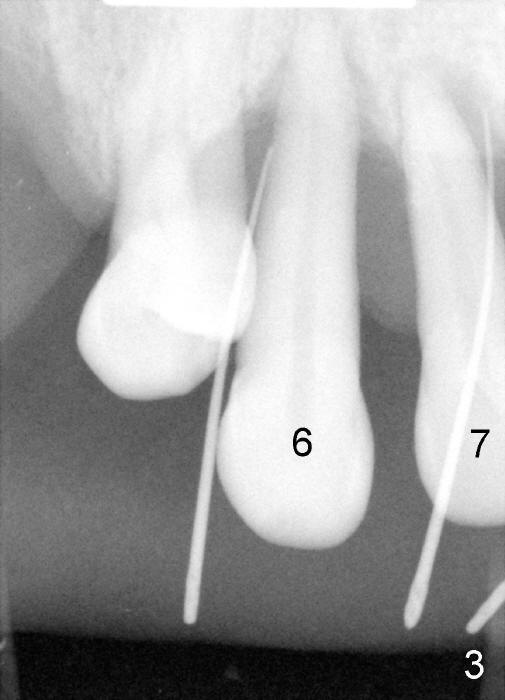
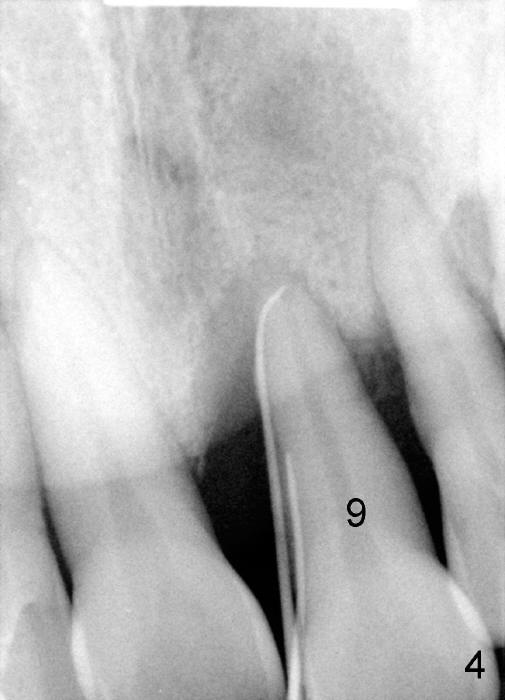
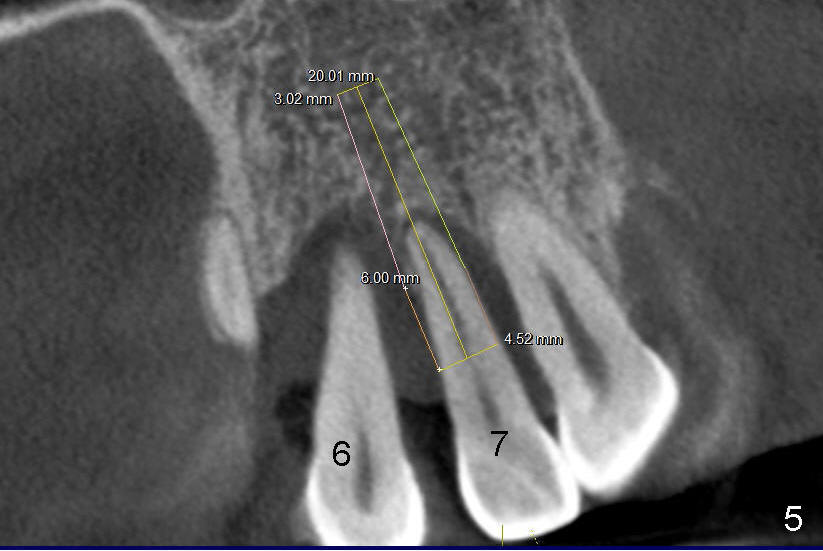
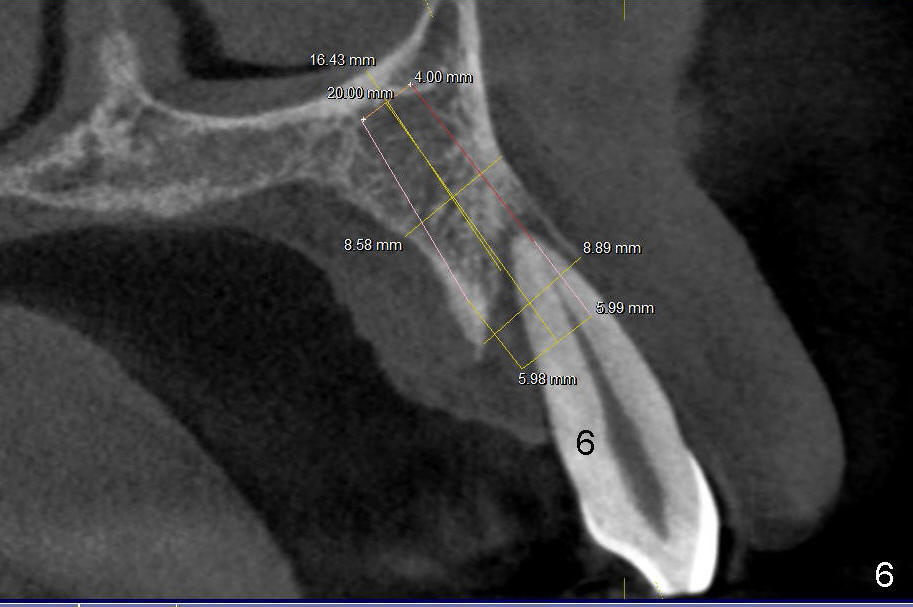
He has lost several upper teeth: #2,3,4,14 and 15. The remaining teeth
are loose, particularly #6,7, and 9 (Fig.1-4). There are several
treatment options for him. Tell him that the doctor will discuss with
him
-
Double check whether he has taken antibiotic and rinsed with Chlorhexidine
at home
-
First of all, #6,7 and 9 will be extracted with immediate implants and
provisional
-
Since the tooth # 6 shifts the most (Fig.1 arrow), it will be extracted
first (the reason will be further explained in section #9), followed by
thorough curettage, copious irrigation and soak with antibiotic
-
Prepare a large bowl for Normal Saline and small one for Clindamycin.
-
Cut a 2x2 into small pieces (9) and soak in Clindamycin solution, insert one
piece into the socket, then irrigation, repeat these steps 3 times.
When the socket is pretty clean, use a plastic pipet to collect blood
-
Use the teeth #5,7 as guides for #6 pilot drill (Tatum) trajectory, with
depth ~14 from gingival margin until the drill is relatively stable
-
Then ext #7, curettage, rinse, antibiotic soak, rinse, pilot drill (Bicon,
possible with drill extension)
-
Take PA with 2 pilot drills in place.
-
Bicon reamers, save bone, later mix with synthetic bone (Osteogen), reamers
until 3.0 mm for #7, 3.5 for #6, tap 4.5x20 for 6, then 5x20, possibly 6x20
-
Take PA again with 3.0 mm reamer in #7 socket, a tap in #6
-
Place implants as palatally as possible. Use Tatum tapered drills if
orientation changes unfavorably
-
Try in abutments. If straight, no cementation; prep
-
Use crown forms for temporary crowns. Check occlusion
-
Bone graft deep portion of buccal sockets
-
Cementation, remove cement thoroughly
-
Then more bone grafting in the more coronal portion of the sockets
Return to
Assistants,
Upper Incisor Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 10/26/2013, last revision
04/27/2014