
|
|
|
|
|
|
||
|
|
|
|
|
|
||
Prevent Post-Implant Infection
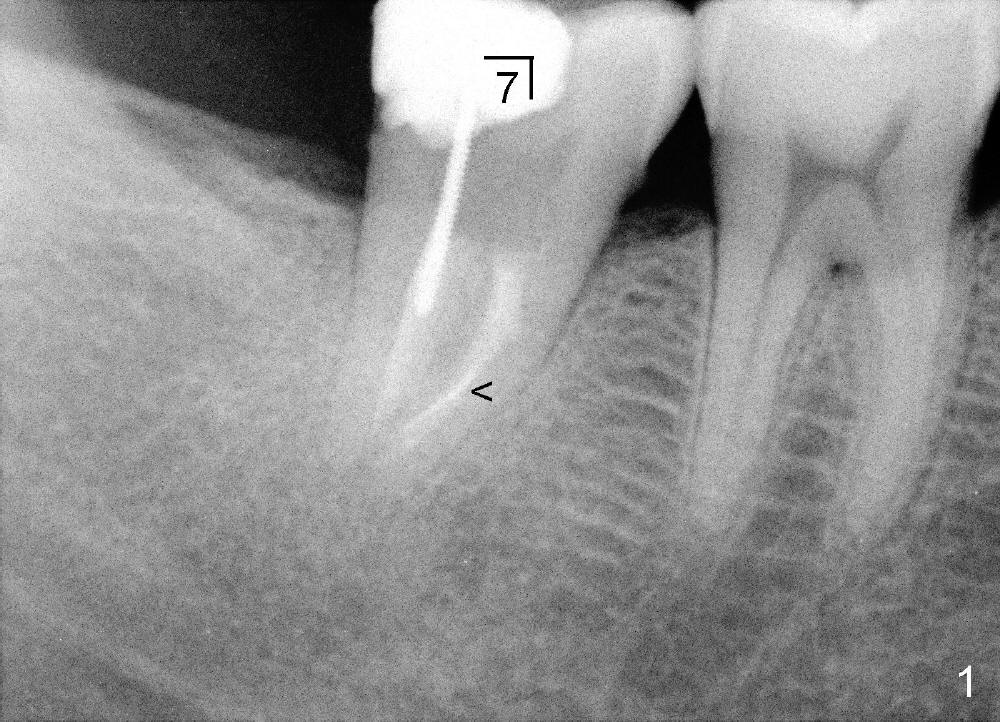
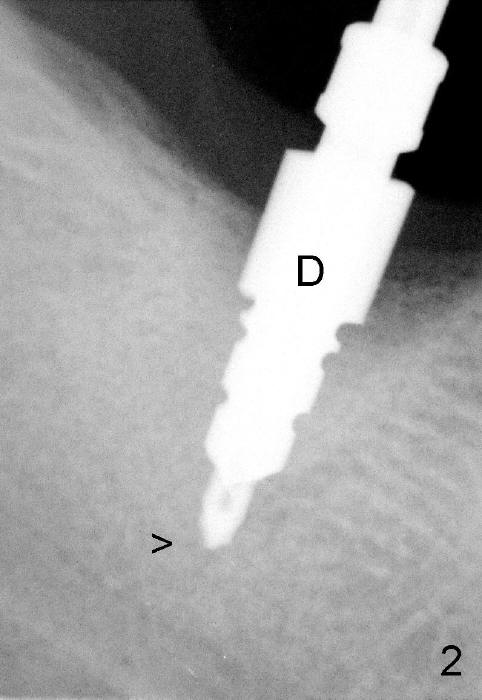
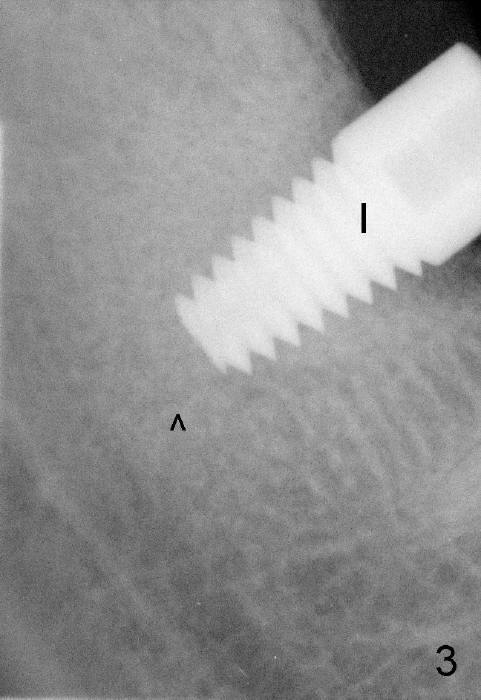
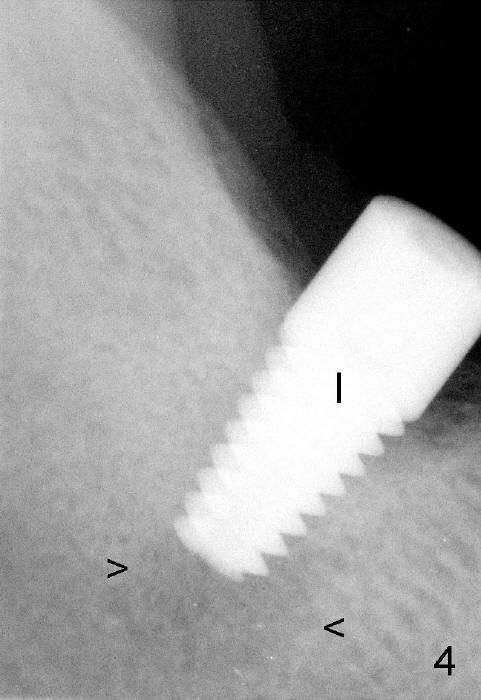
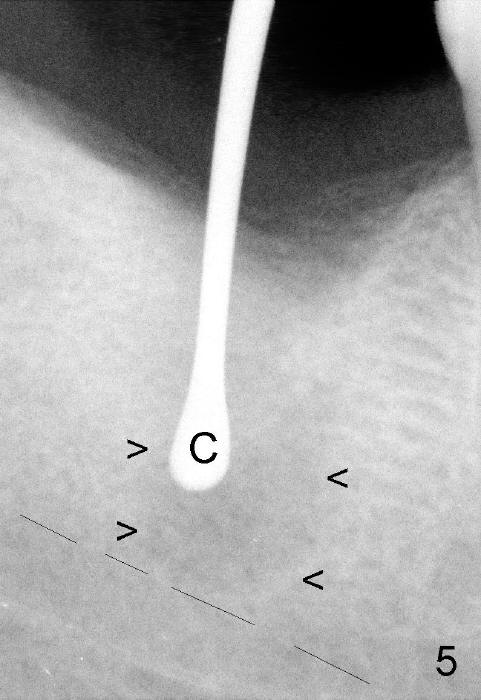
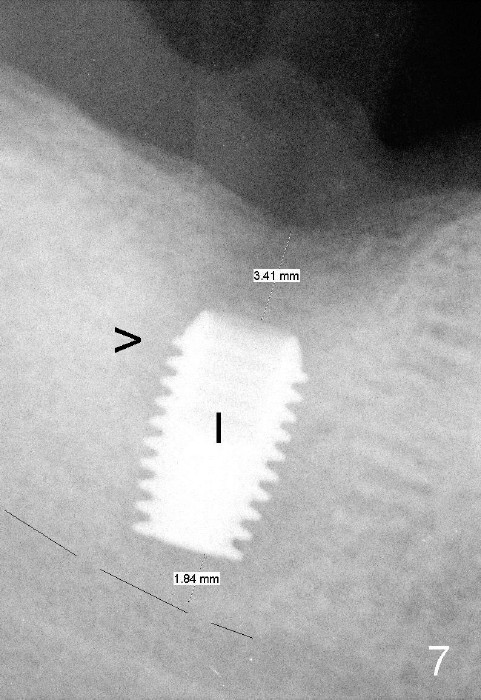
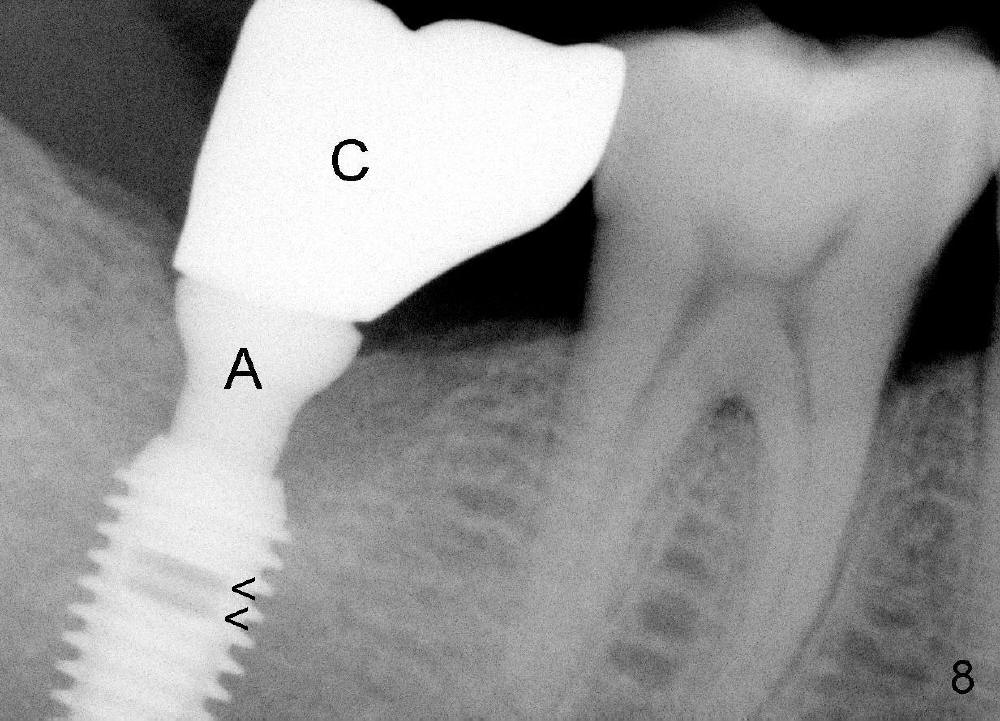
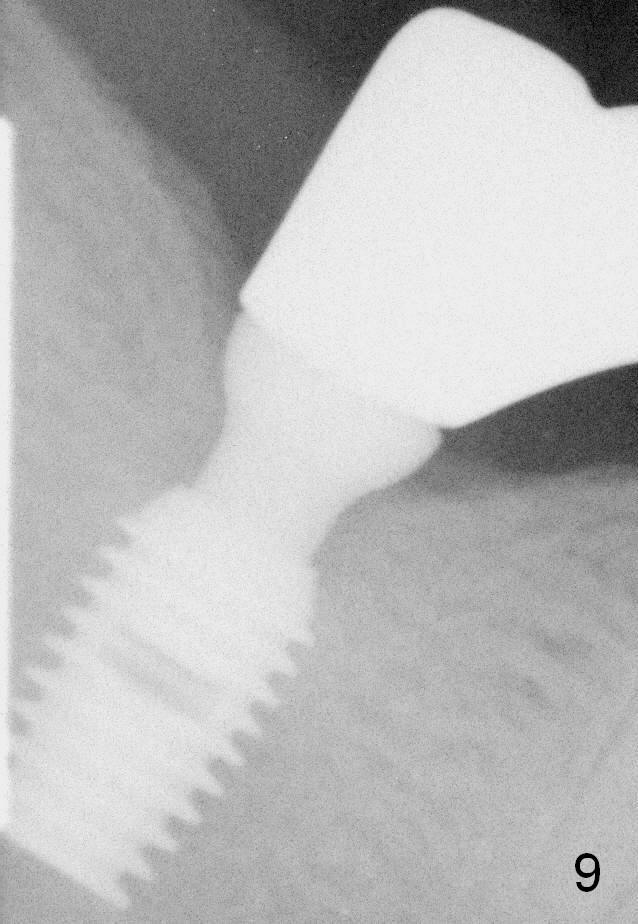
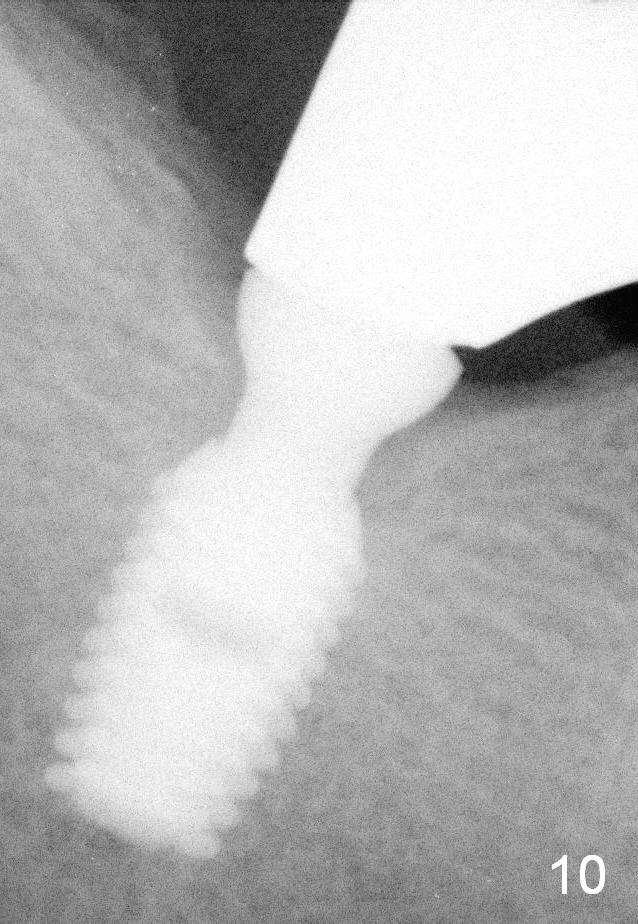
It is advantageous to place implant immediately or shortly (4-8 weeks) after extraction. But most teeth to be extracted are potentially infected, such as in the case of Ms. Pei (Fig.1). Periapical radiolucency (PARL) is not obvious prior to extraction. Six weeks post-extraction, osteotomy is finished with bone expansion and drilling (Fig.2 D, 5x14mm). Tatum tapered implant is placed (Fig.3 I: 6x14). So far PARL is minimal if any (Fig.2,3 <). Pain develops approximately 20 days post-implantation with expanding PARL (Fig.4 <). Antibiotic treatment does not resolve the infection. The implant has to be removed. Infected granulation tissue is thoroughly removed from the apical portion of the socket (Fig.5 <) with a curette (C). Scaling and root planing is done for 4 quadrants. A month later, potentially infected hard tissue is removed by reamers (Fig.6 D, 5 mm). Bicon implant is buried inside the bone and separated from the oral cavity (Fig.7 I, 5x8). At that time, there is a gap next to the implant (>). Five months later, the gap disappears, suggesting implant osteointegration (Fig.8). Extraoral cementation is done between abutment (A) and crown (C). The abutment/crown unit is tapped into the implant with 2 visible threads (<). The latter indicates that the abutment is completely seated. Dashed lines in Fig.5-7 denote the upper border of the inferior alveolar canal. PAs are taken 6 months (Fig.9) and 1 year 7 months (Fig.10) post cementation. In all, it is a hassle to do re-implantation. Efforts should be exerted to prevent post-implant infection.
Assistants, Long Term Follow-Up, Implant Fails Xin Wei, DDS, PhD, MS 1st edition 09/14/2013, last revision 05/18/2018