



|
|
|
|
|
|
|
|
|
|
|
|
Immediate Implant is the best way to prevent dry socket
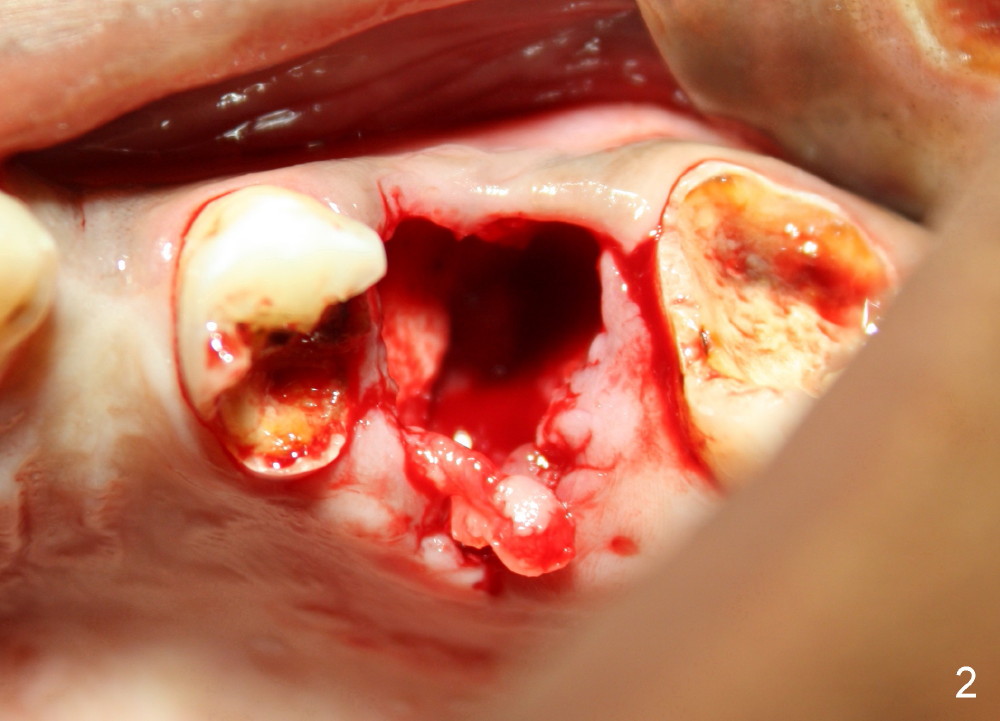
Rishawn, 23 years old, has had severe caries. The tooth #14 is unsalvageable (Fig.1). Due to finance, immediate implant is not considered. Upon extraction, there is no septum, probably resulting from infection (Fig.2). Six days later, dry socket develops with excruciating pain (Fig.3 *: yellowish and grayish exudates in the socket). The chance of dry socket would have dropped if the immediate implant were placed.
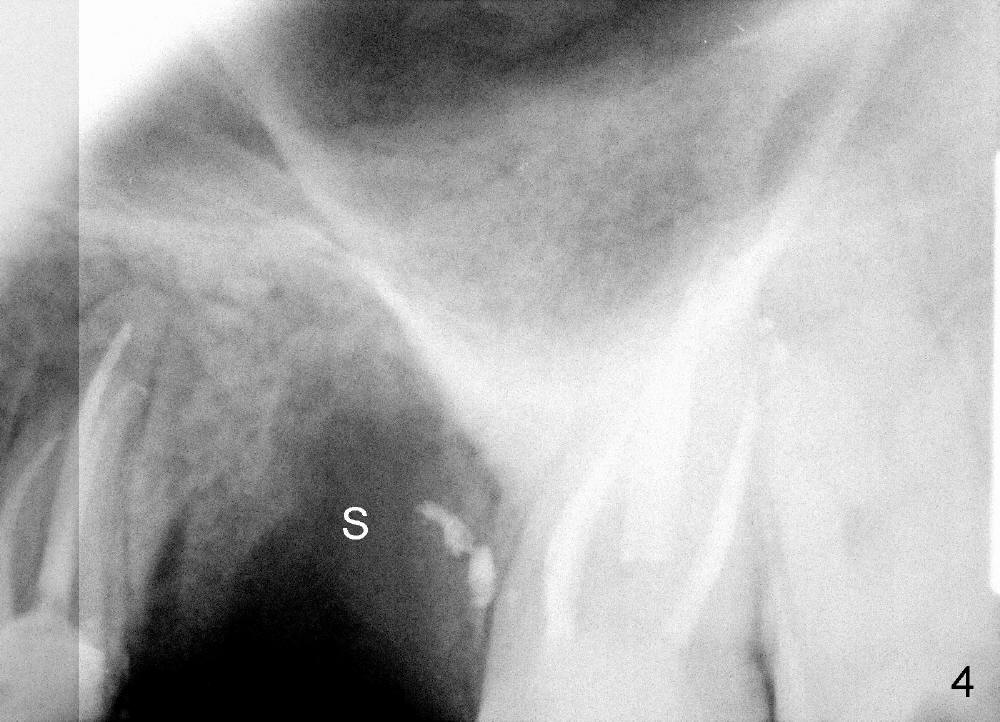
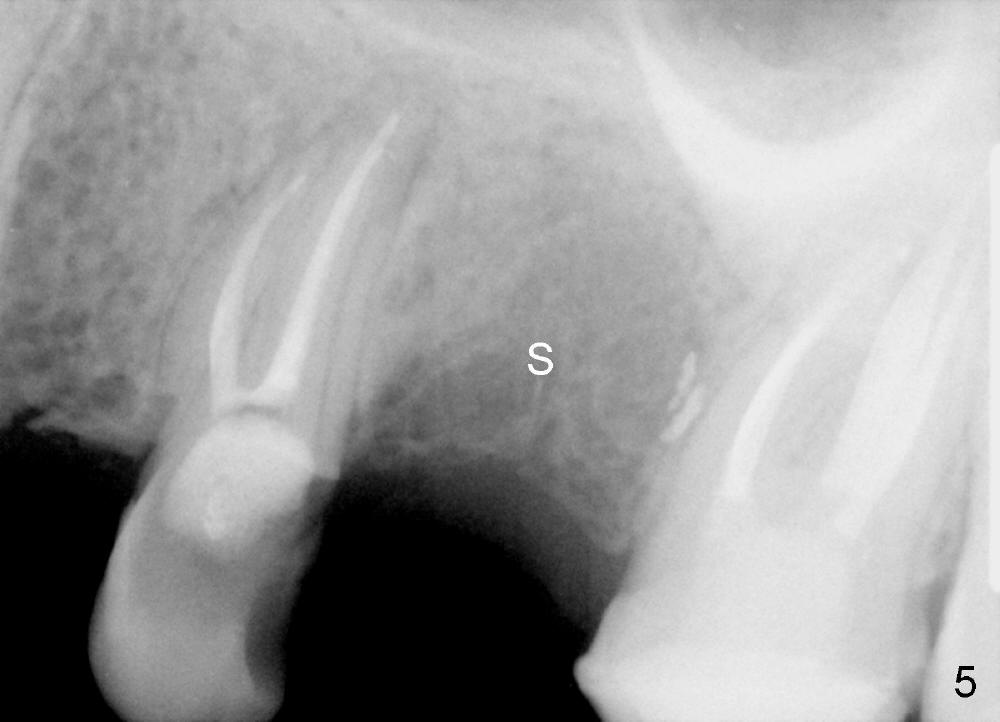
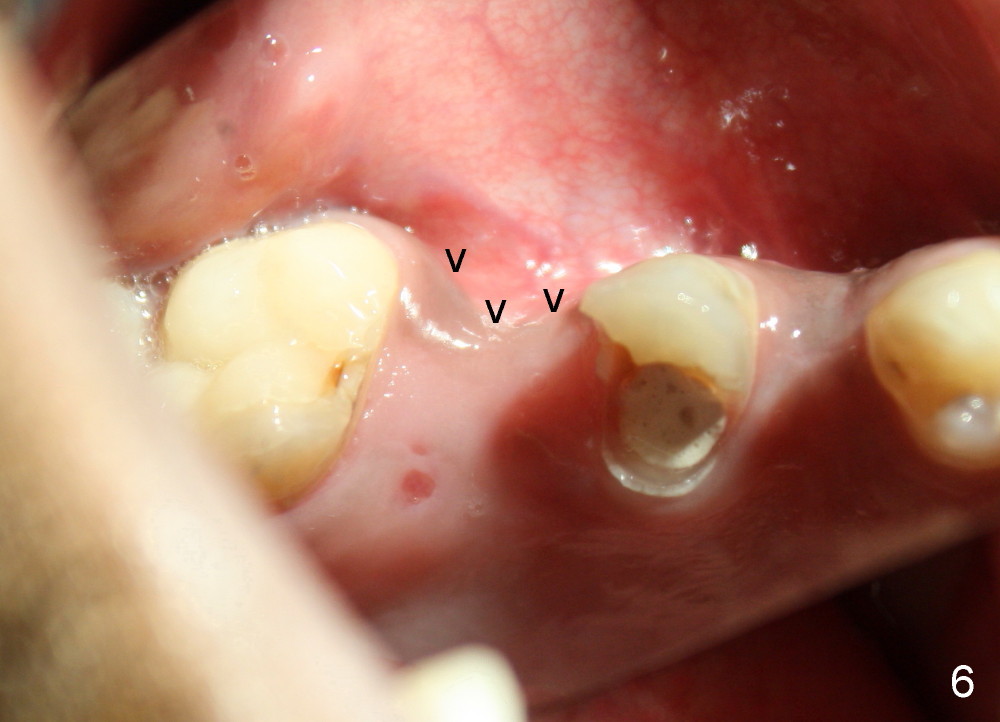
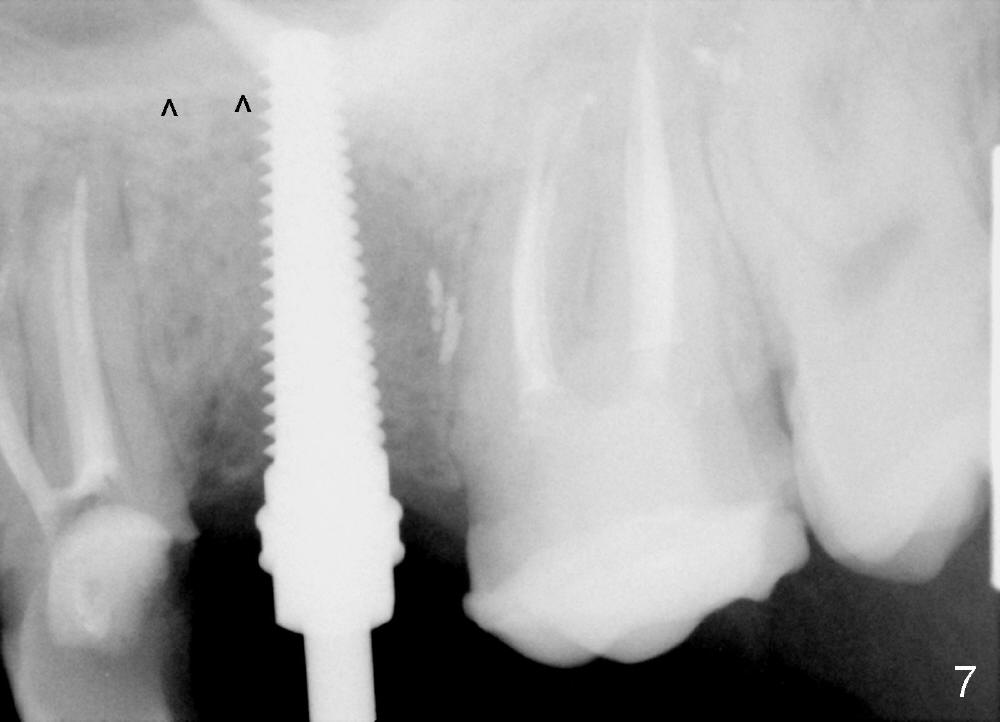
The socket looks empty two months post-extraction (Fig.4 S). Bone appears to re-grow in the socket 9 months after extraction (Fig.5 S), but the buccal plate is severely atrophic and concave (Fig.6 arrowheads). When an incision is made, the socket feels soft. Osteotomy is created by bone expansion (round tapered osteotomes (RT) 2,3,4 mm). Drilling is done once, using 3.5x17 mm tapered drill when the larger RTs meet resistance near the sinus floor. Tapered taps are used to continue to expand the osteotomy (4.5 (Fig.7), 5.0 and 6.0x20 at the depth of 17 mm). Finally 6.0x17 mm implant is placed with insertion torque more than 60 Ncm (Fig.8). The buccal plate is less concave with bone expansion and implantation (Fig.9 arrowheads). Without immediate implant, bone resorbs quick, which makes delayed implantation difficult.
Xin Wei, DDS, PhD, MS 1st edition 10/03/2013, last revision 10/04/2013