
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||||
Bone Graft When Sinus Membrane is Perforated?
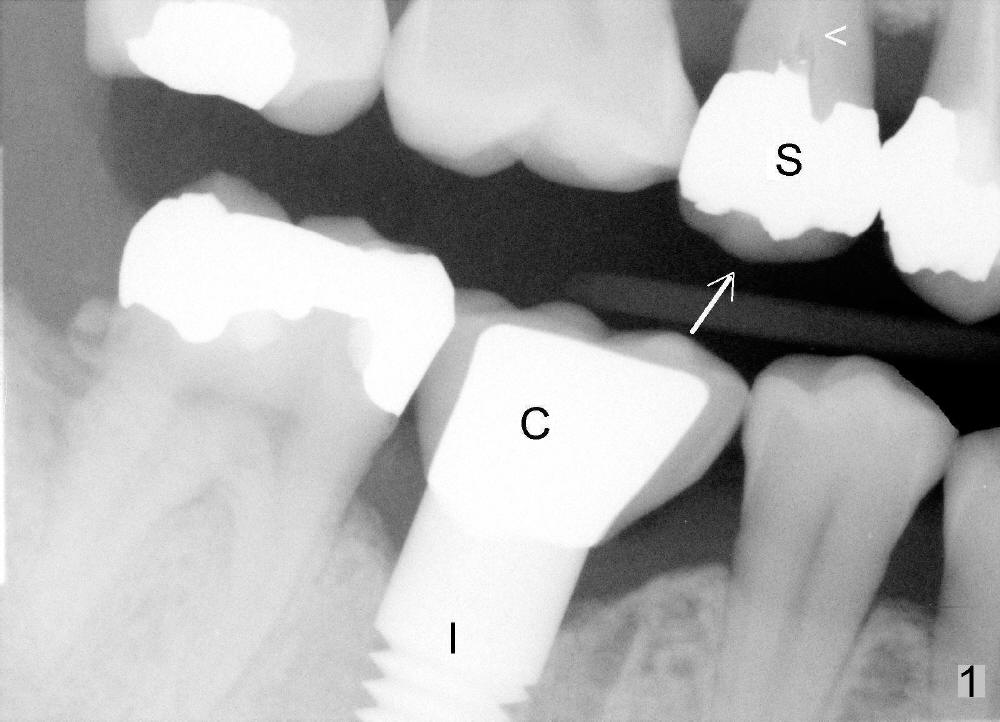
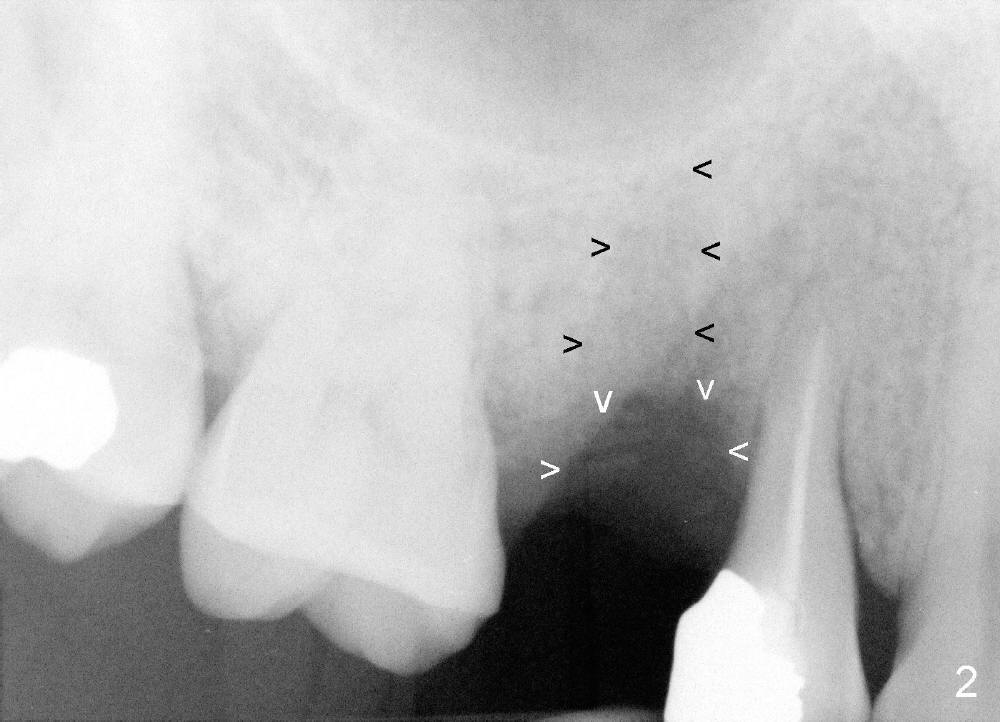
A few months after cementation of implant (Fig.1 I) crown (C) at #30, a 44-year-old man fractured the tooth #4 with MOD amalgam (S) and root canal thereapy (<) while he was visiting his home country. Fig.2 shows the socket (black arrowheads) and bony defect (white arrowheads).
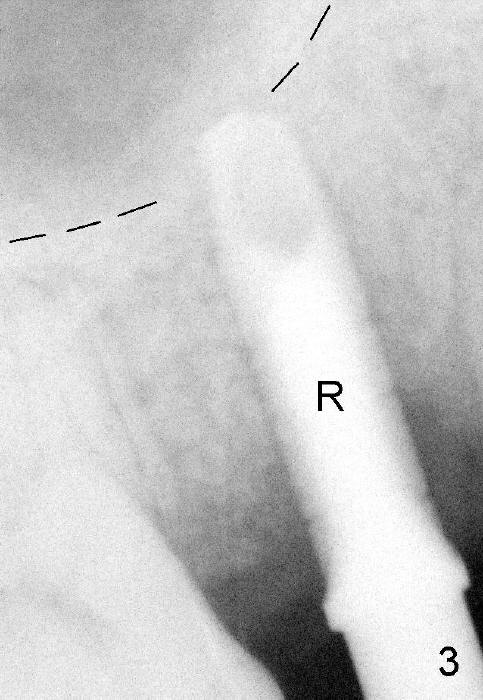
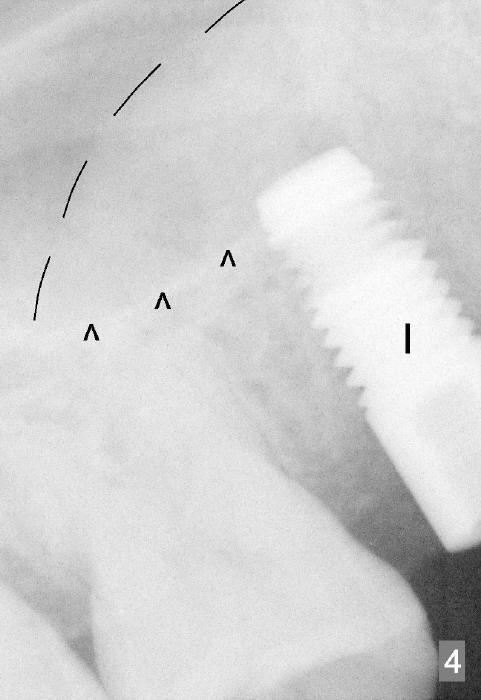
Osteotomes are used to form initial osteotomy, approximately 11 mm deep, 4 mm wide. Bicon reamers (Fig.3 R) are used to increase osteotomy while collecting autogenous bone; it appears that the sinus floor is partially penetrated (dashed line). After sinus lift (Fig.4 dashed line), a 5x14 mm cylindrical tissue-level implant is placed (I; arrowheads: sinus floor). There is no intraop nasal hemorrhage. Amoxicillin is prescribed postop (500 mg tid for 7 days). There is purulent, particulate discharge from the right nostril postop. One month later, the implant is loose and removed.
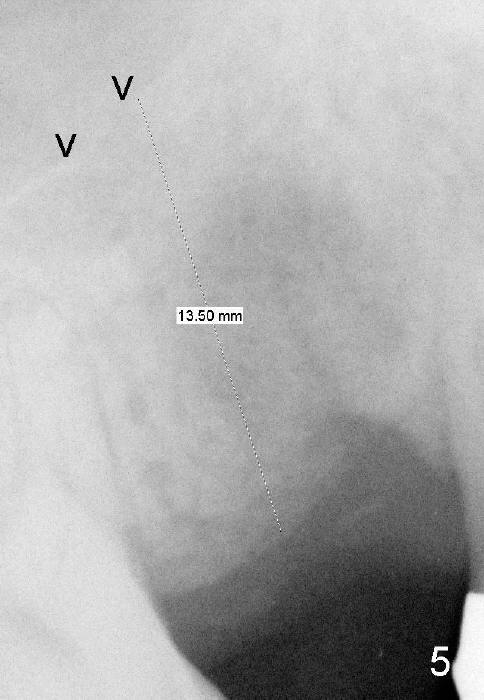
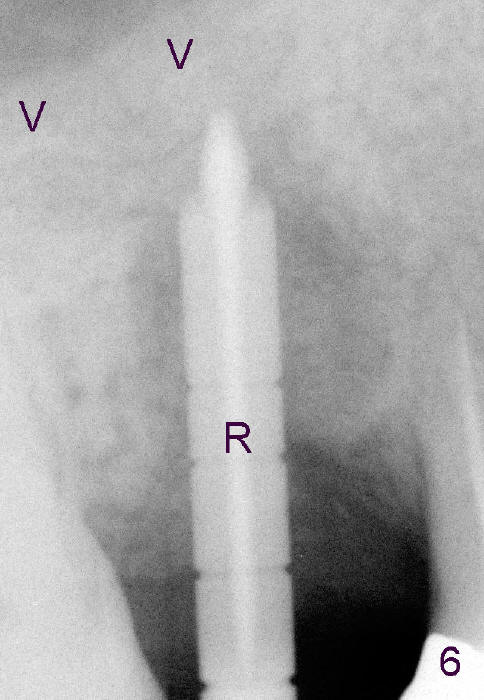
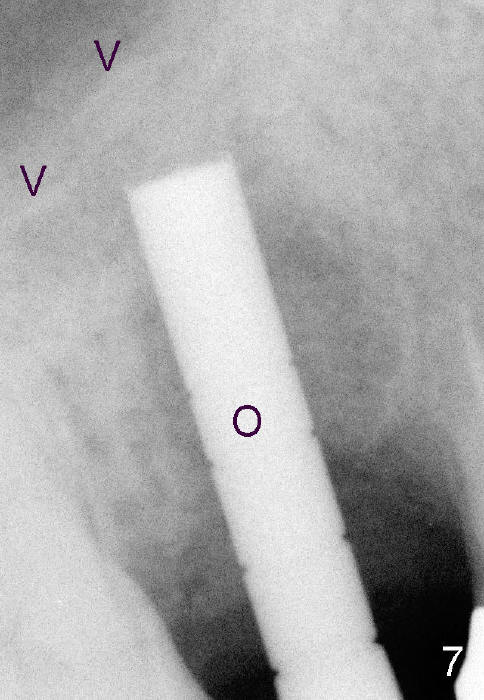
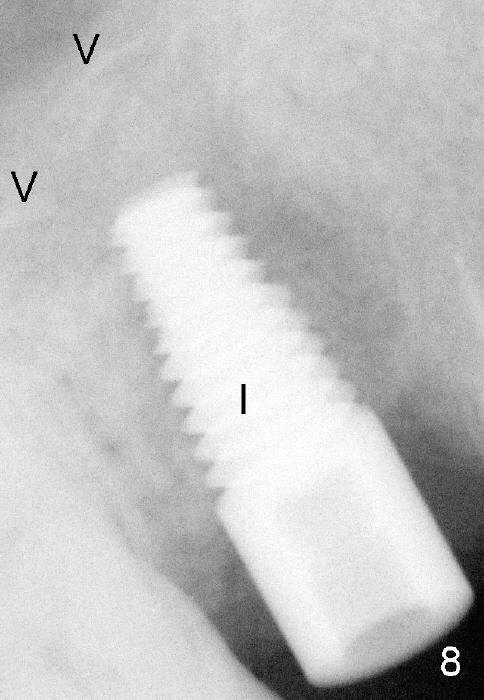
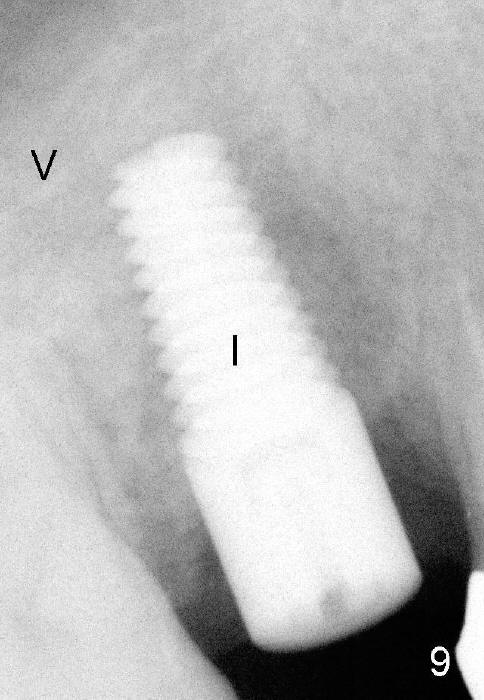
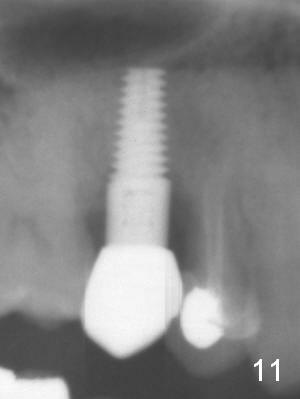
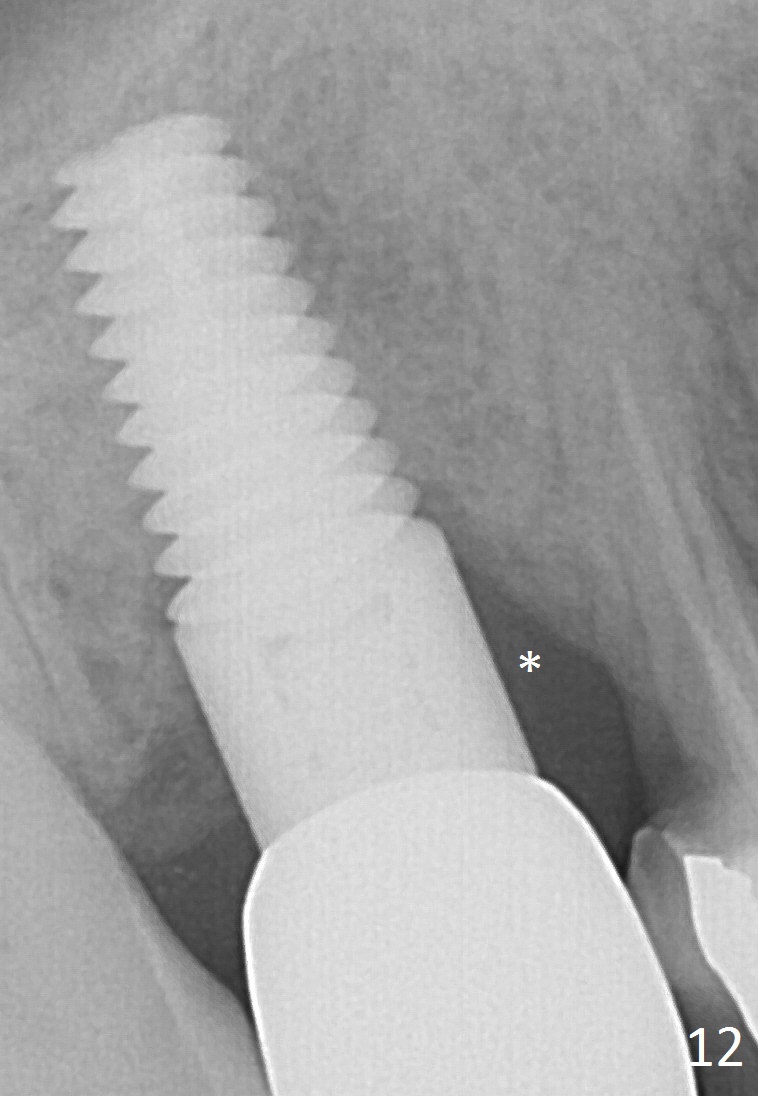
Four months after implant removal, the bony defect appears to increase (Fig.5). Reamers (Fig.6 R)and osteotome (Fig.7 O) are short of the sinus floor (arrowheads). A 5x14 mm tapered implant is placed with primary stability (Fig.8 I). The implant is placed ~ 2 mm deeper (Fig.9). No bone graft is used for sinus lift. There is no complication. The sinus floor appears to be repaired 4.5 months postop (Fig.10). Fig.11 (trimmed from panoramic X-ray) is taken 1 year 7 months post cementation. The bone remains stable 4 years 2 months post cementation (Fig.12); the mesial defect is most likely related to extraction trauma (*).
When sinus lift is being attempted, double check whether the sinus membrane is perforated. If perforation is extensive, repair with insertion of collagen membrane, but not bone graft.
Return to Follow Up
Xin Wei, DDS, PhD, MS 1st edition 03/31/2013, last revision 05/18/2018