




|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Immediate Implant Avoids Injury to Mental Loop
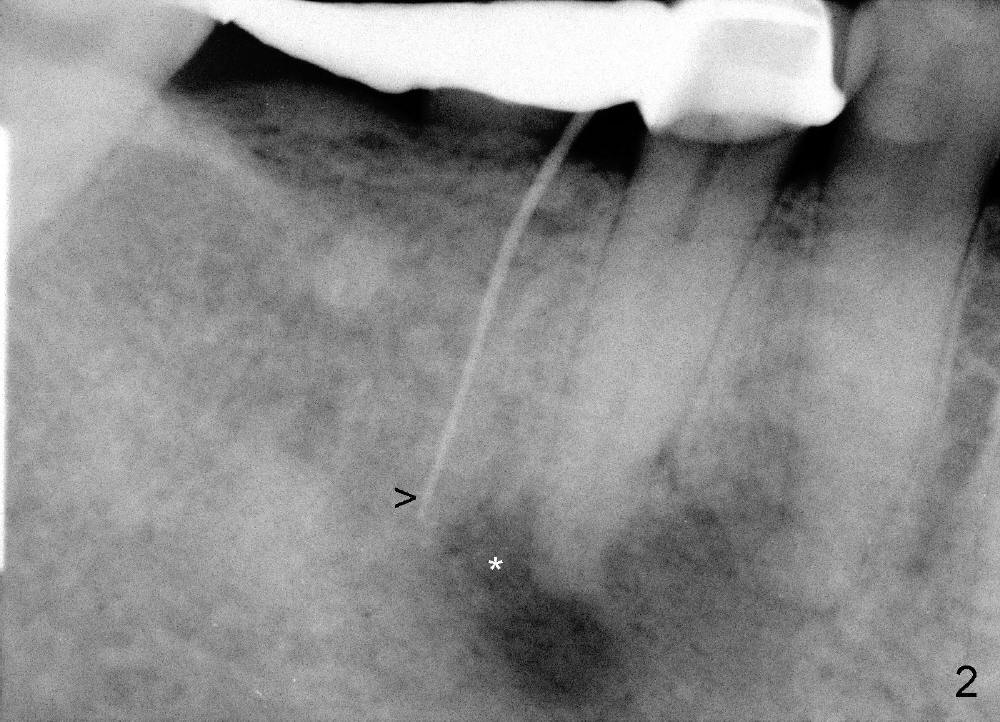
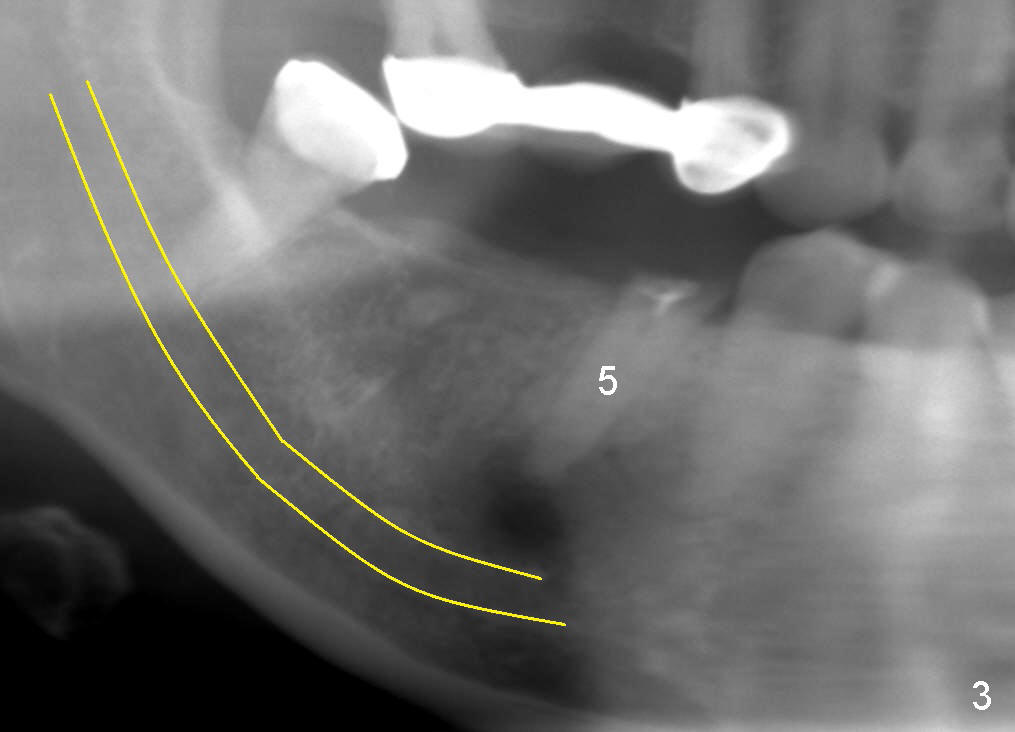
A 49-year-old lady cannot chew with the lower right bridge (Fig.1: from the 2nd premolar (5) to the third molar (8)). Insertion of gutta percha (Fig.2 >) points to the apical radiolucency of the anterior abutment (*). The bridge is sectioned between the pontic of 2nd molar and the retainer of the posterior abutment. The anterior segment of the bridge falls out. The anterior abutment is non-salvageable due to severe 2nd caries (Fig.3 (5) part of panaramic X-ray). The yellow lines denote the inferior alveolar nerve. In brief, the apex of the affected tooth is most likely closely associated with the mental loop.
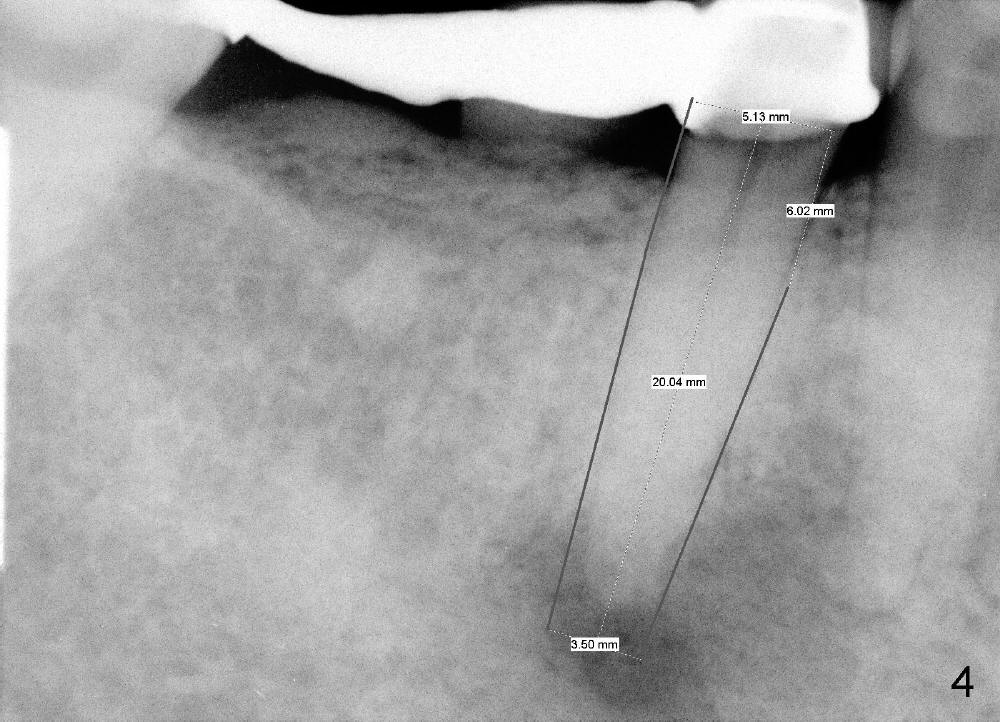
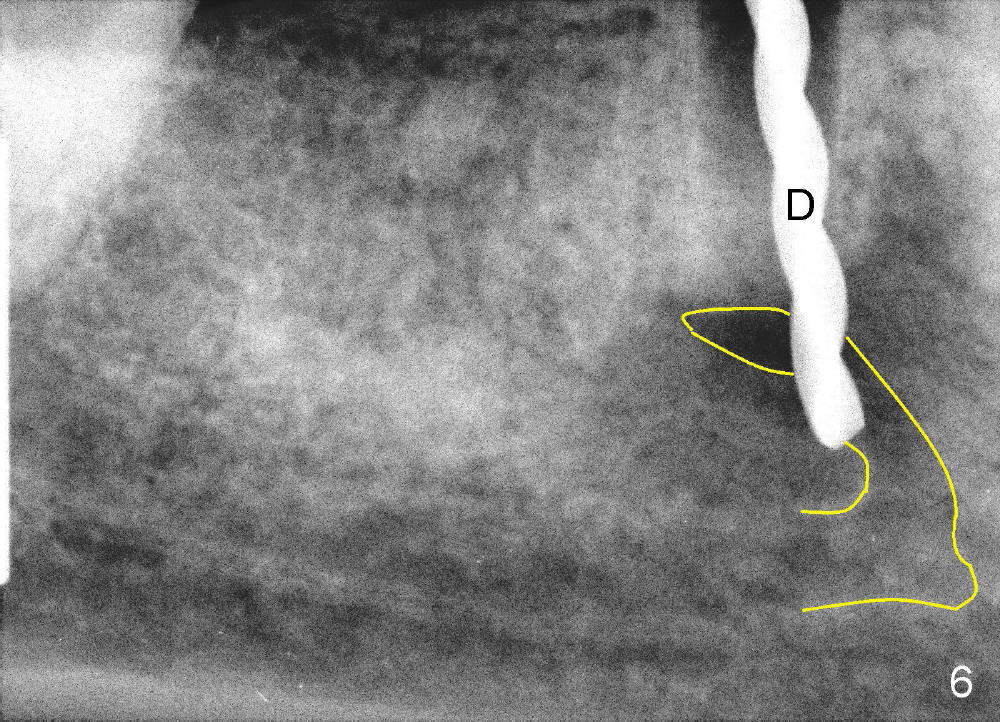
If the immediate implant (5x20 mm) is placed within the confinement of the socket, the integrity of the nerve will be not violated (Fig.4). The patient returns for the surgery 2 months after bridge removal. The root stump is cleaned so well that the buccal apical fistula disappears (Fig.5). The mesiodistal dimension of the root is 5 mm, whereas buccolingual 6.5 mm. Infiltration (not block) anesthesia is administered. The root is extracted. A 2 mm pilot drill drops by itself into the socket (Fig.6 D); the loop should overlap the apex of the socket.
The apical lesion is mainly located in the lingual aspect of the socket. Curettage of granulation tissue is accomplished lingually to avoid potential damage to the buccally located loop. Copious irrigation is applied to the socket with normal saline and hydrogen peroxide, followed by soaking with 150 mg Clindamycin suspension.
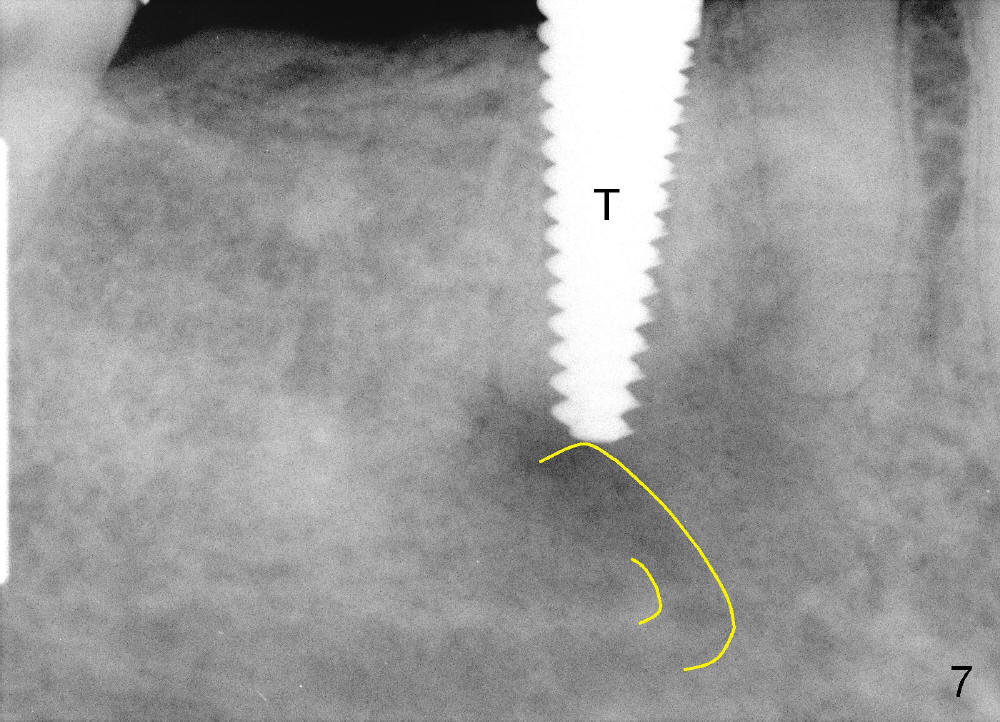
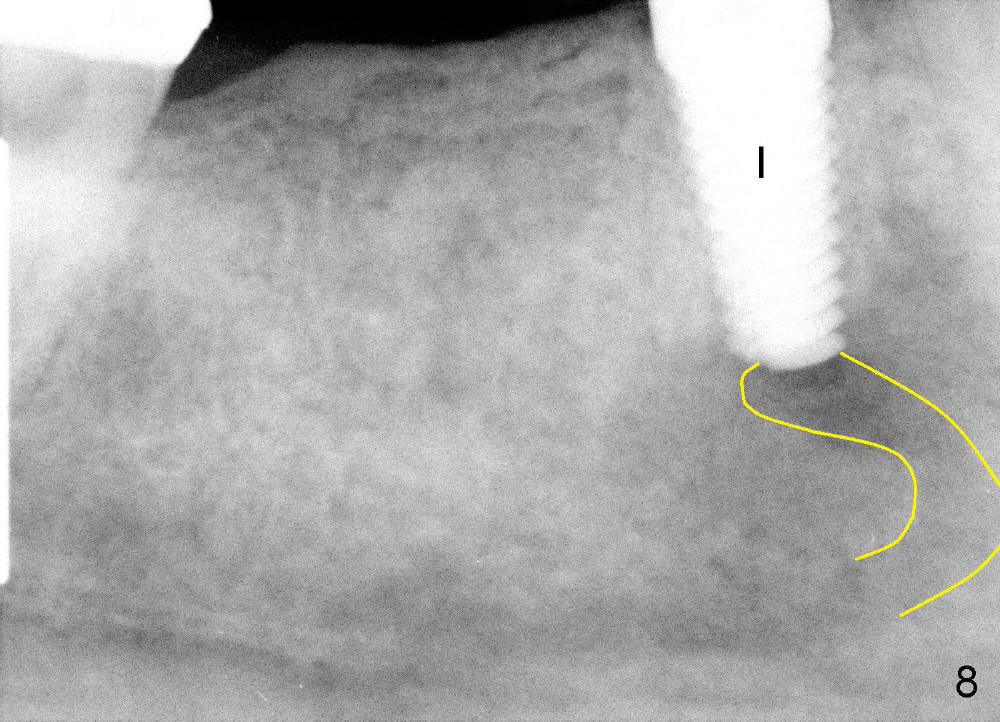
Osteotomy is created by using taps manually. There is no engagement of 5x20 mm tap (at the depth of 17 mm) with the socket. When a 6x20 tap (17 mm deep) is inserted, it is stable (Fig.7). In order to engage better, a 6x17 tapered drill is used (force applied lingually). Finally 6x17 mm implant (Fig.8 I) is inserted with torque more than 60 Ncm. The opening of the socket is obliterated by the large diameter implant, as evident by Fig.9,10 (2 weeks postop). There is no sign or symptom of paresthesia intra or post-op.
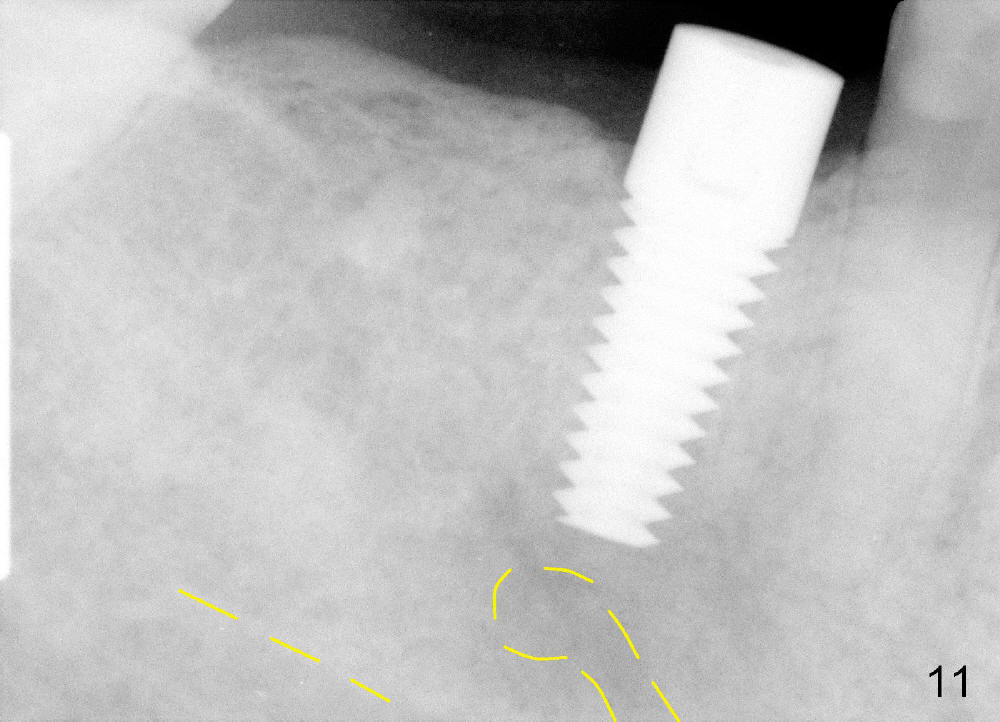
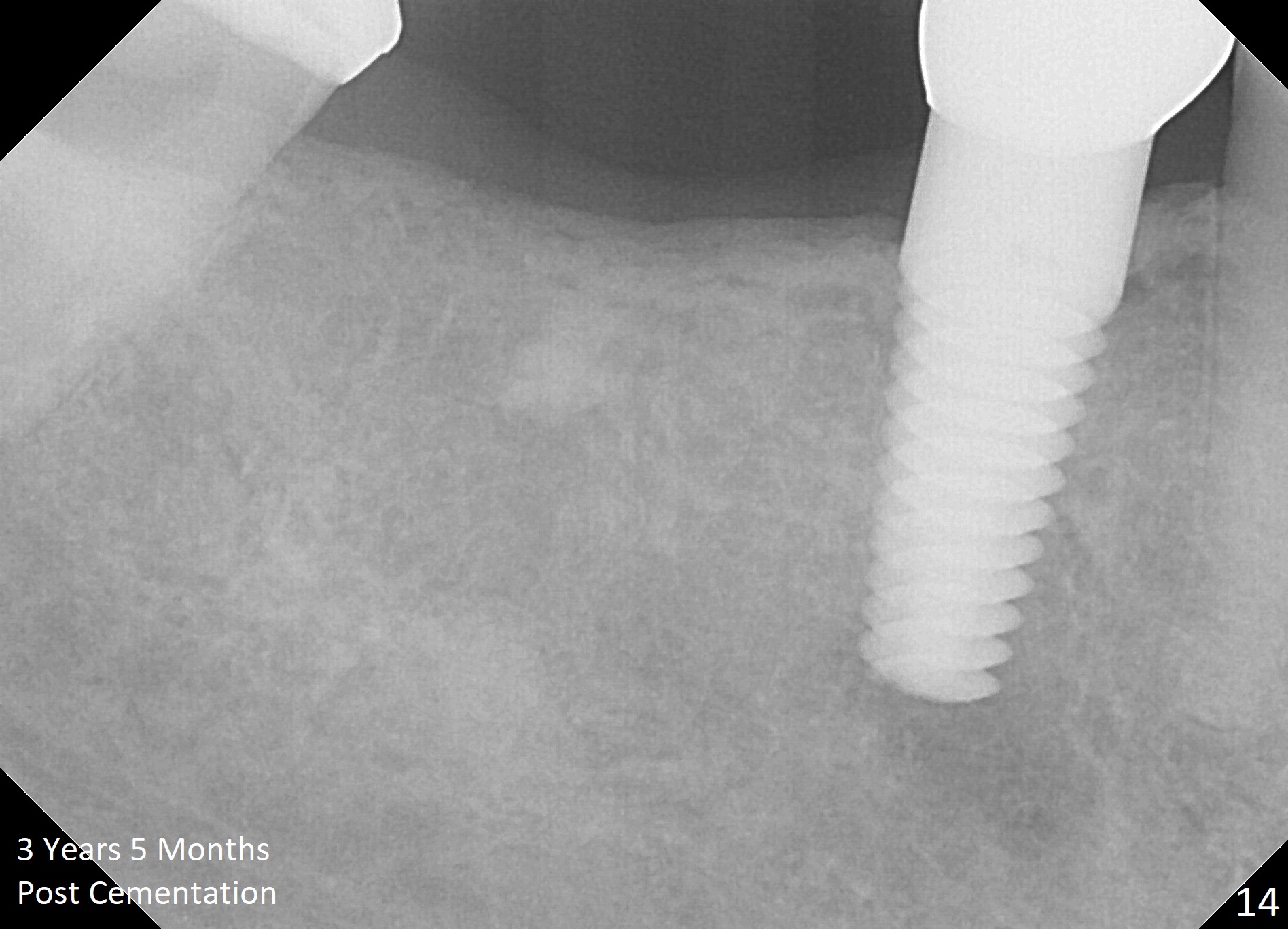
The implant appears to be osteointegrated 4 months postop (Fig.11). A healing cuff is inserted in preparation for restoration 2-4 weeks later (Fig.12). Fig.13 shows that the crown is just cemented. One month later, the patient is concerned about the metal showing through the gingiva (*). To overcome the issue, gold coated implant is used, an implant is placed more lingual (smaller), or bone graft is placed buccal to the implant. There is no bone loss 3 years 5 months post cementation (Fig.14).
Immediate Implant Safety Issues, Immediate Implants for Lower Bicuspids, Introduction to Immediate Implant, #30,31
Xin Wei, DDS, PhD, MS 1st edition 09/04/2013, last revision 12/25/2017