




|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
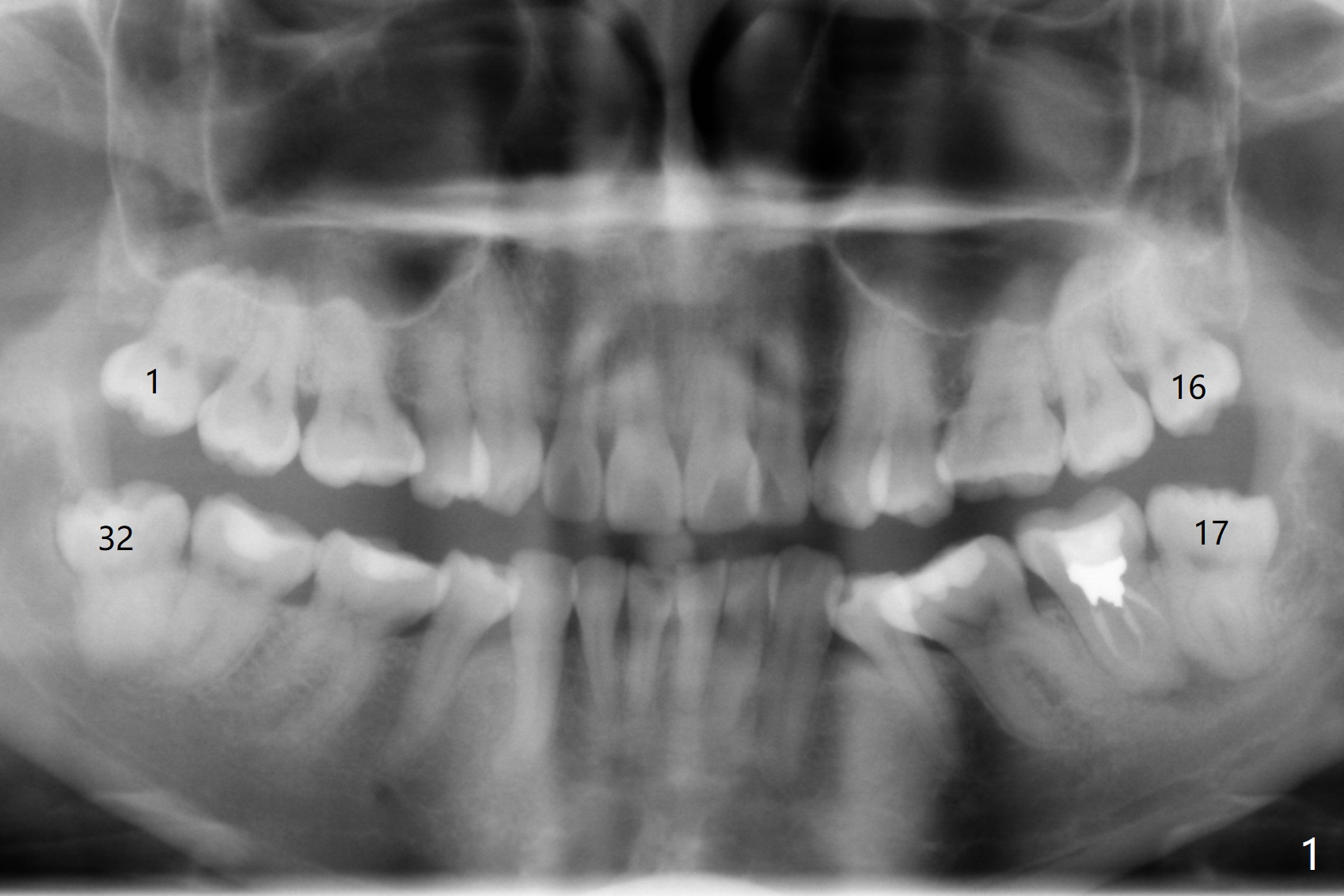
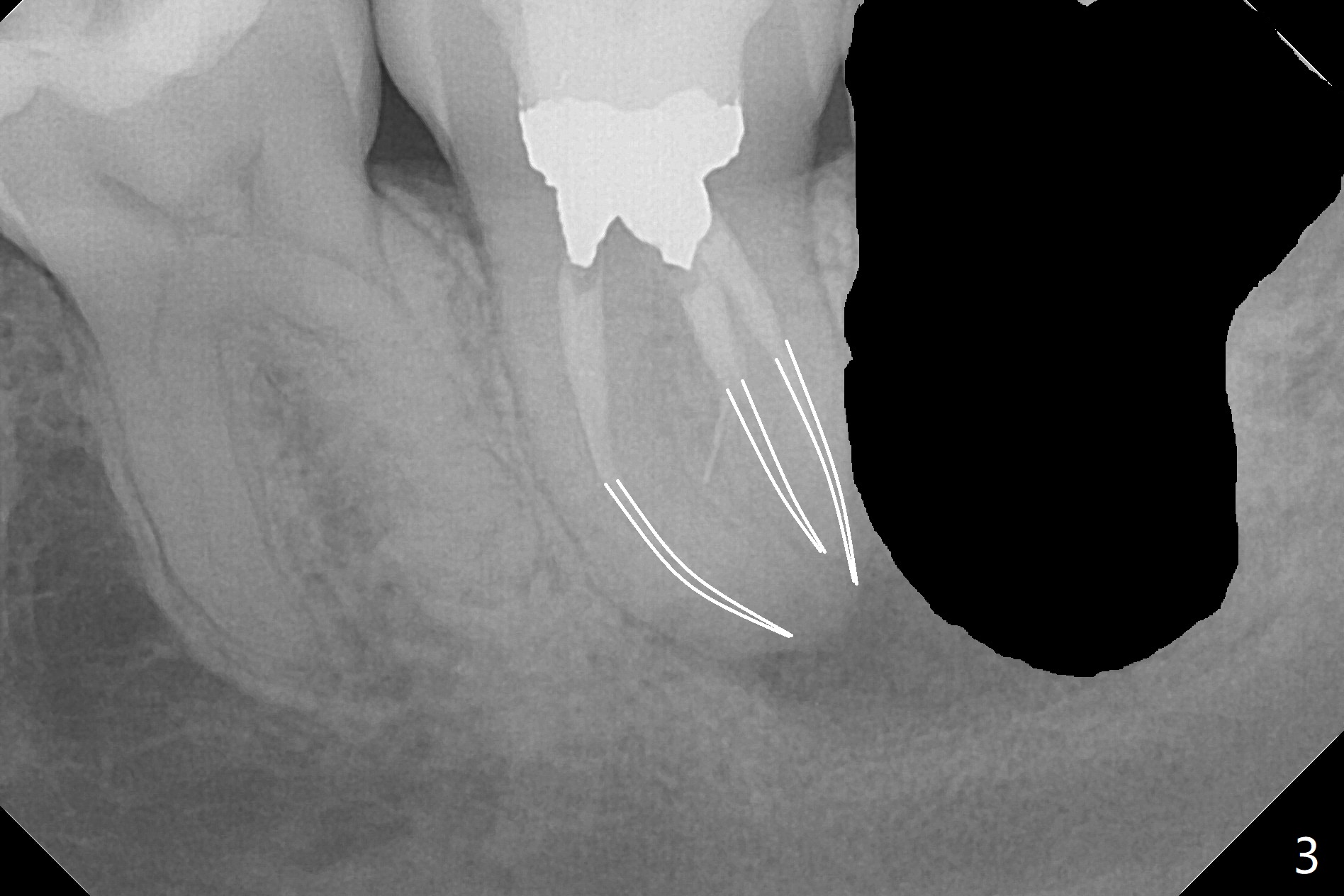
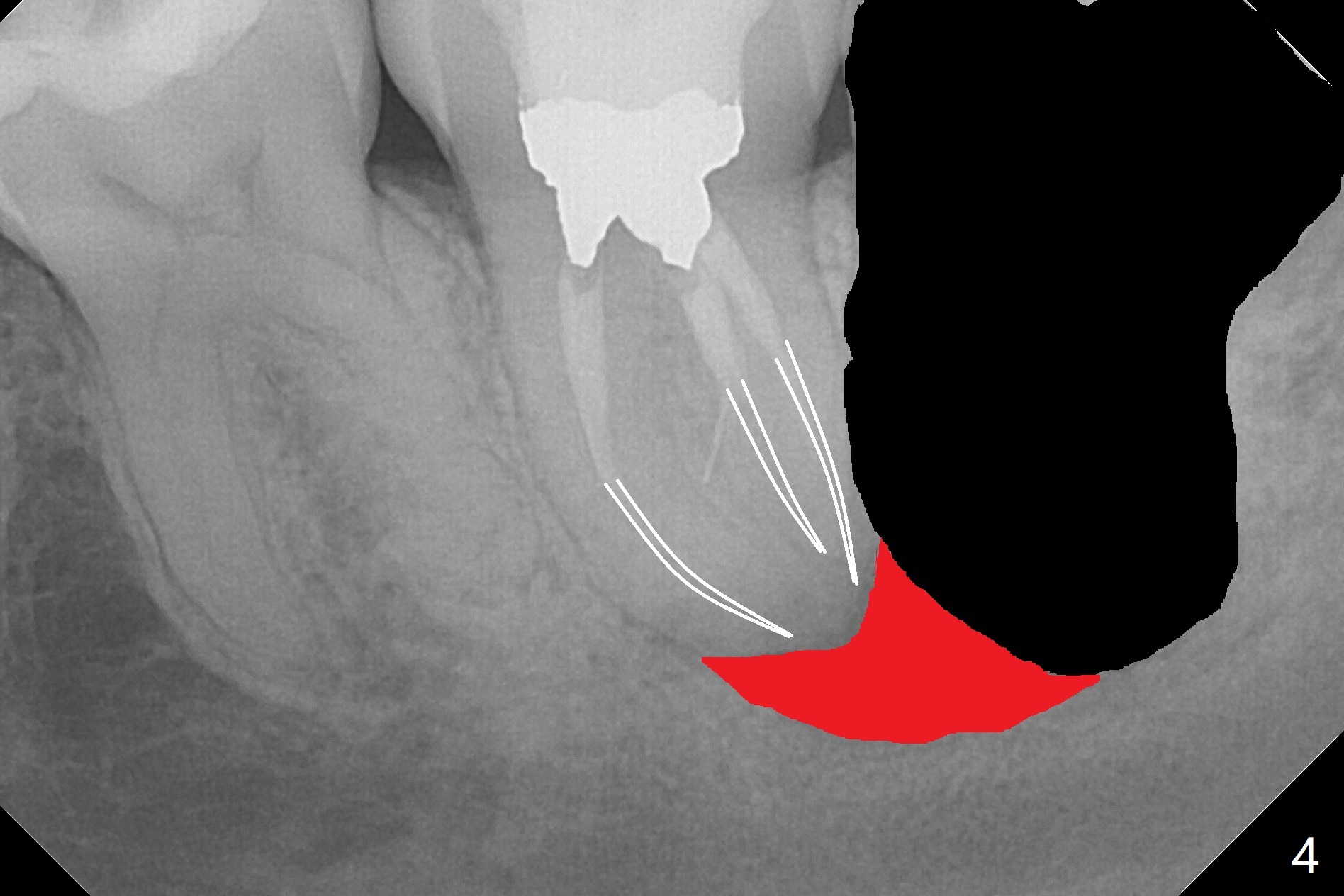
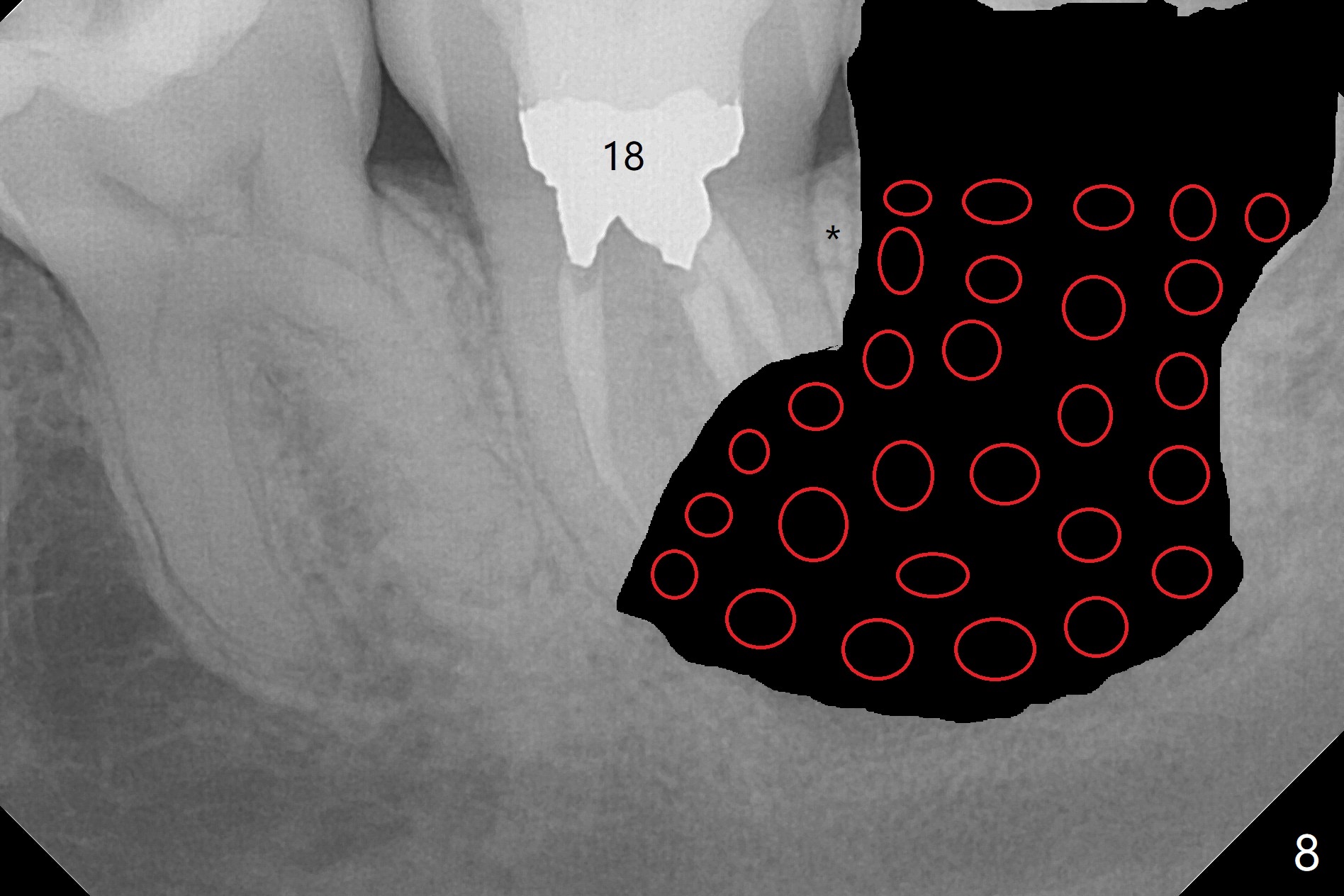
RCT Retreat, Apical Surgery Before 3rd Molar Bone Graft
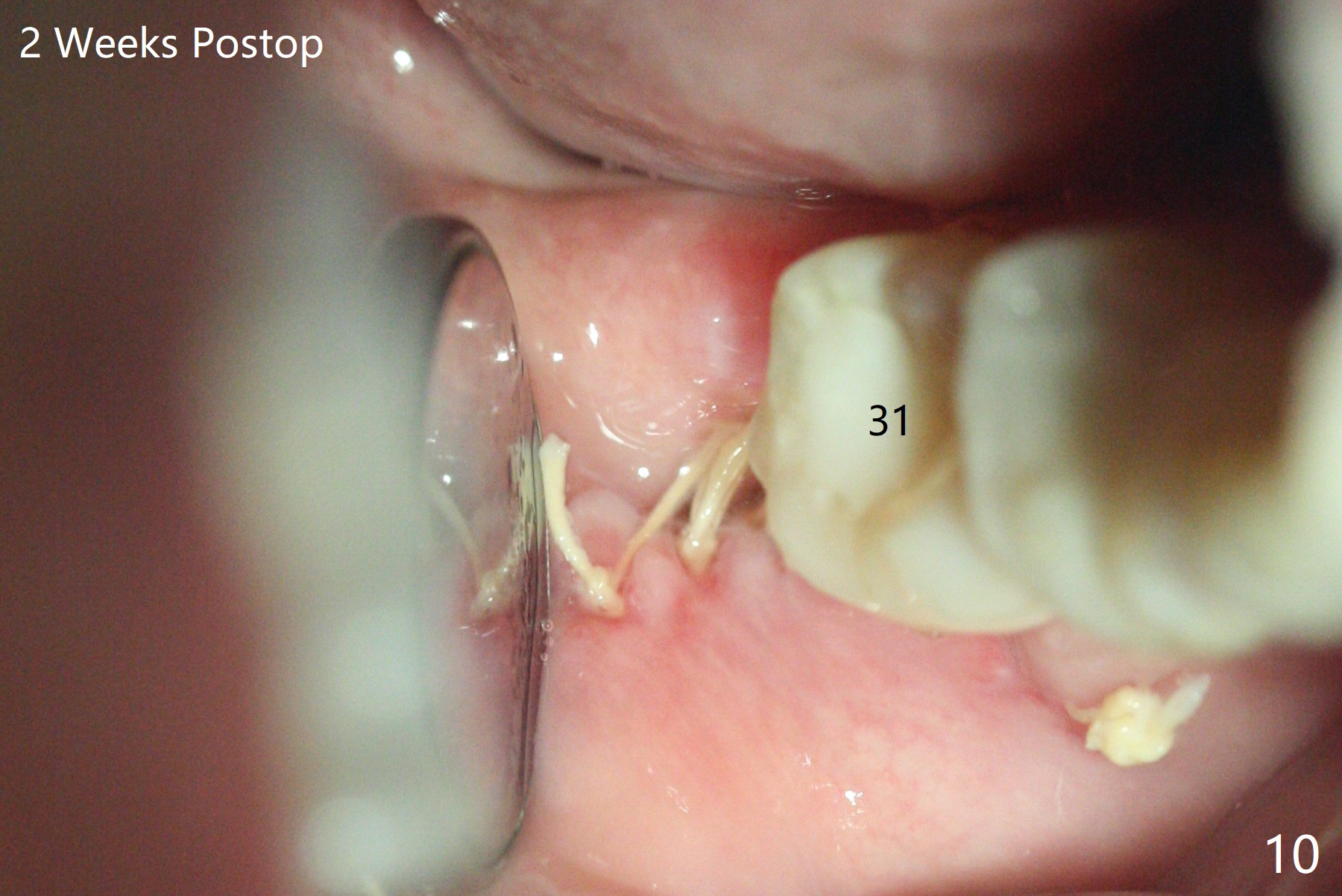
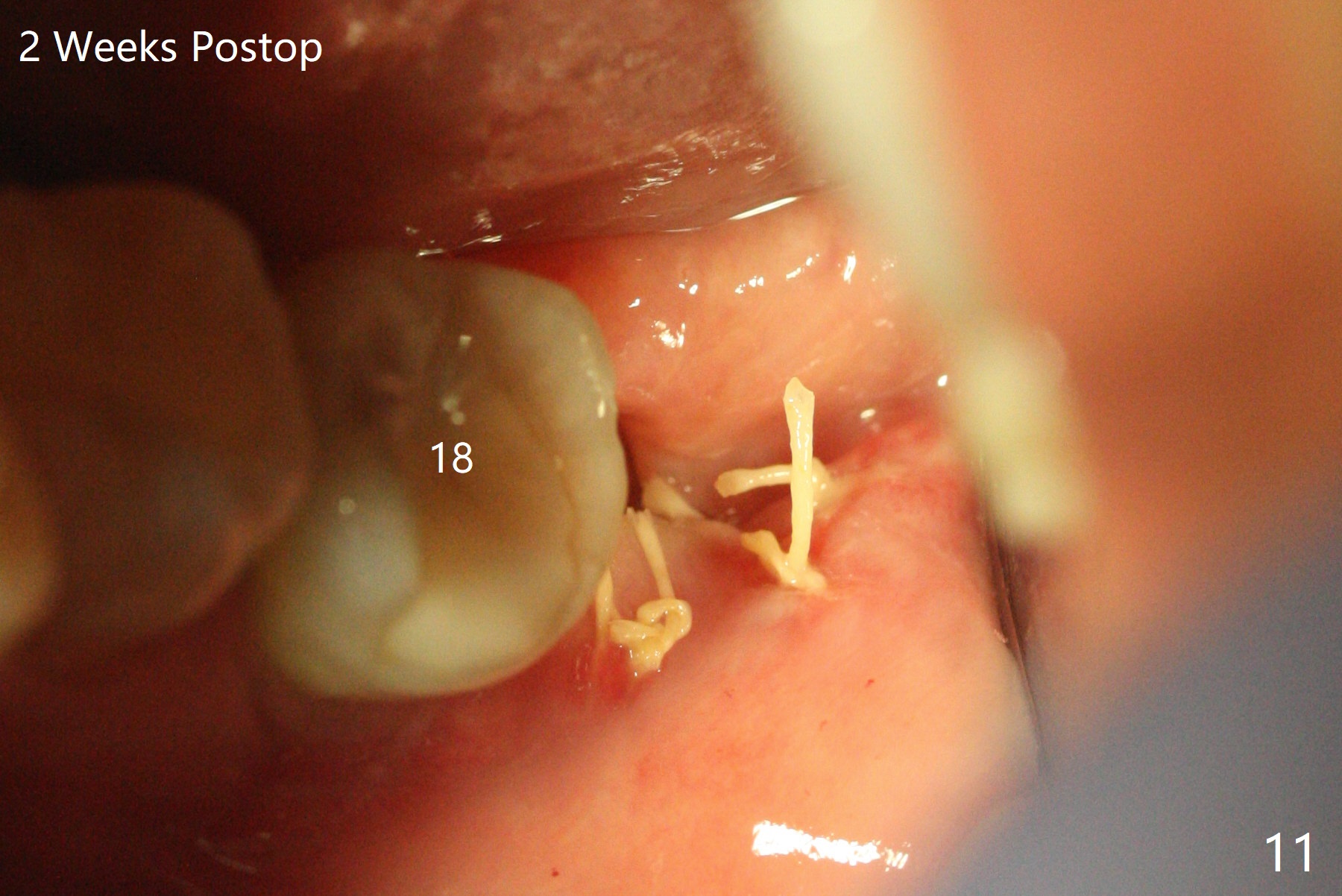
A 37-year-old woman requests extraction of the 3rd molars and orthodontic retreatment (Fig.1). Since the bone between #17 and 18 is thin and short (Fig.2 black *), bone graft is needed after #17 extraction. But the apical infection at #18 (Fig.2 white *) may affect graft survival. The patient agrees to have RCT retreatment done (Fig.3 white curved lines) before extraction (black area). The apical granulation tissue can be removed (Fig.4 red area) prior to bone graft (Augma). The latter will be also placed at #17 as a control. After endodontic consultation, the patient does not want RCT retreatment. She would like to have the 3rd molars extracted first and #18 removed if needed. After #17 extraction (Fig.5), apicoectomy will be performed at #18 (Fig.6 (white outline: surgical bur, use non-torque handpiece)). Following curettage of the apical lesion at #18 (Fig.7), bone graft will be placed (Fig.8 red circles). In fact the patient insists upon #1, 16, 17, and 32 extraction. After extraction, allograft (Fig.9 A (Ossogen, Mineralized Cort/Can (30%/70%), .25-1.0 mm) is placed in the mesioapical of the sockets of #17 and 32, while Osteogen Plug (O) and BioXclude in the distocoronal one (4-0 PGA suture). There is minimal bone between the 2nd and 3rd molars (black arrowheads). The allograft is intentionally pushed into #18 apical defect after enucleation (white arrowhead). The sockets are slightly open, although sutures are in place 2 weeks postop (Fig.10,11). It is unknown whether the bone graft is partially dislodged or not.
Return to
Plug
Xin Wei, DDS, PhD, MS 1st edition
11/01/2019, last revision
12/22/2019