

|
|
|
|
||
|
|
|
|
|
|
|
|
||||
Palatal Placement
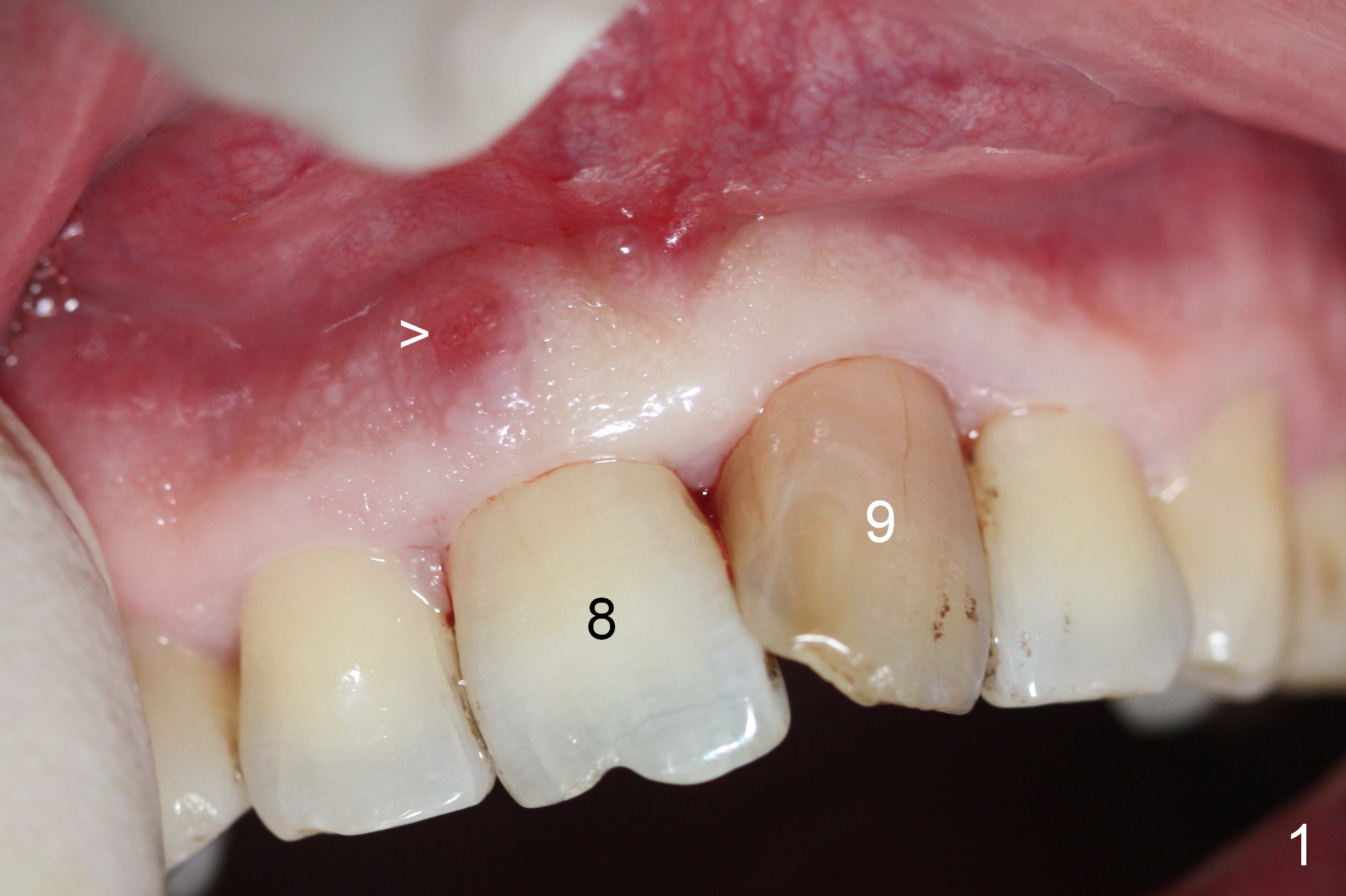
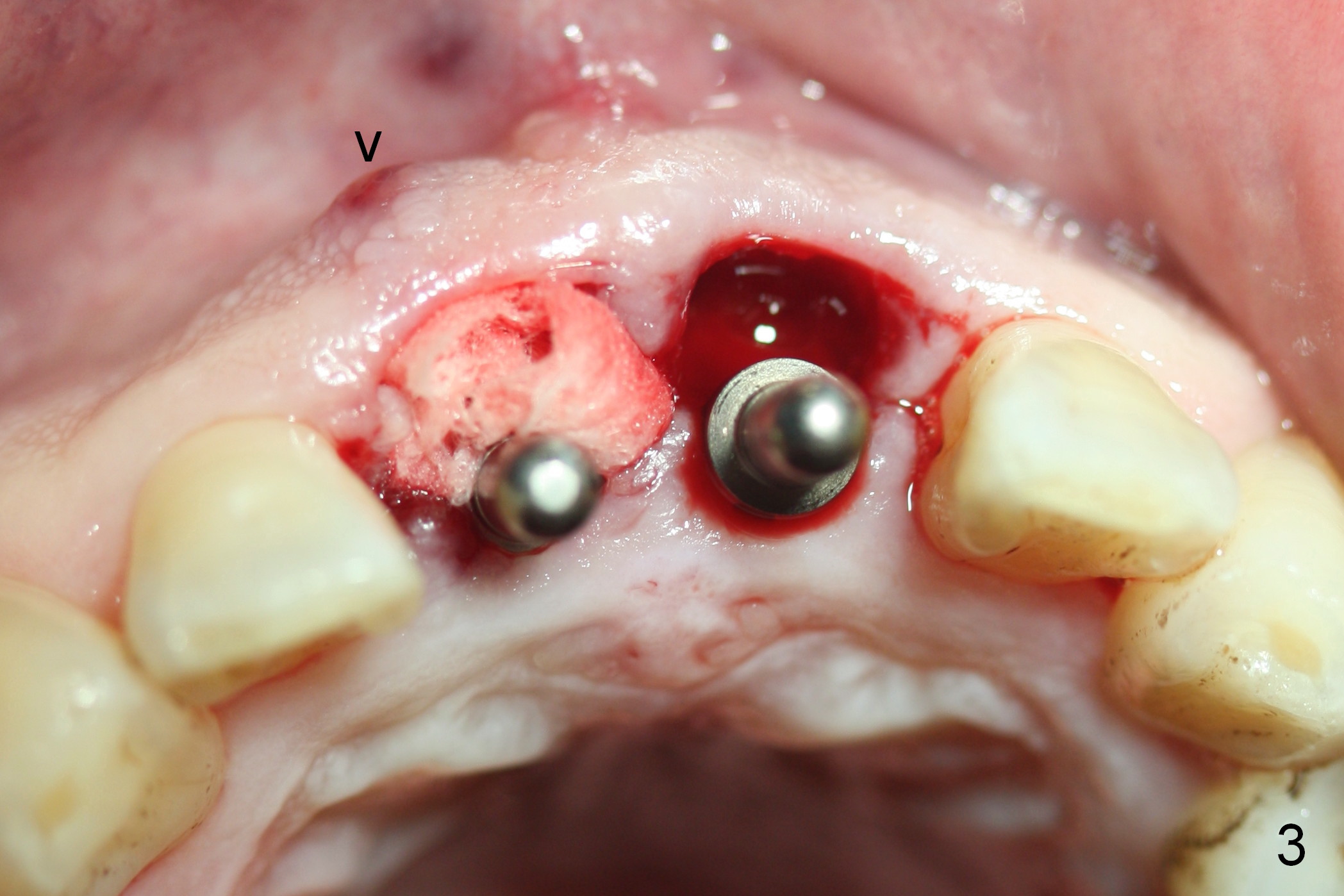
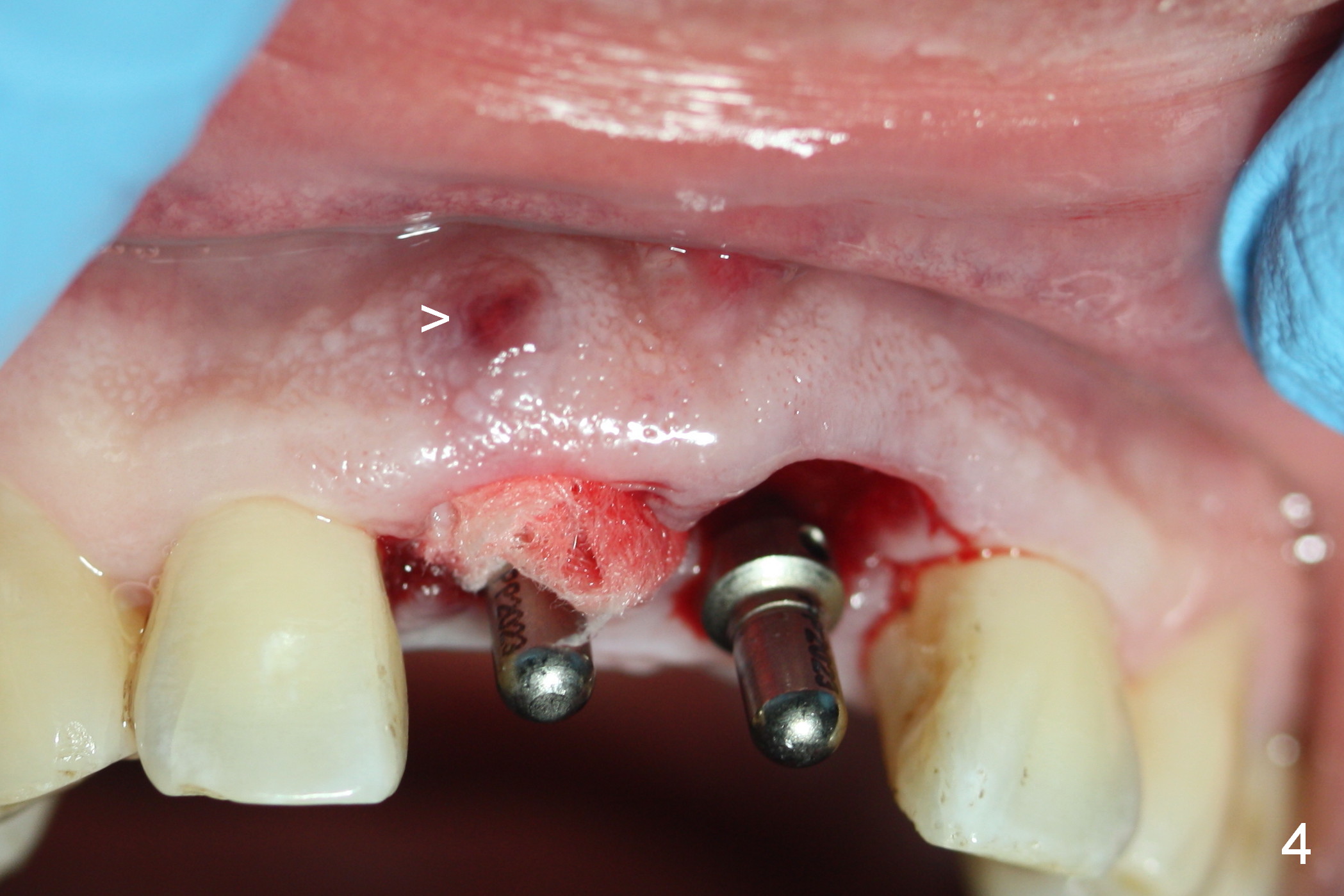
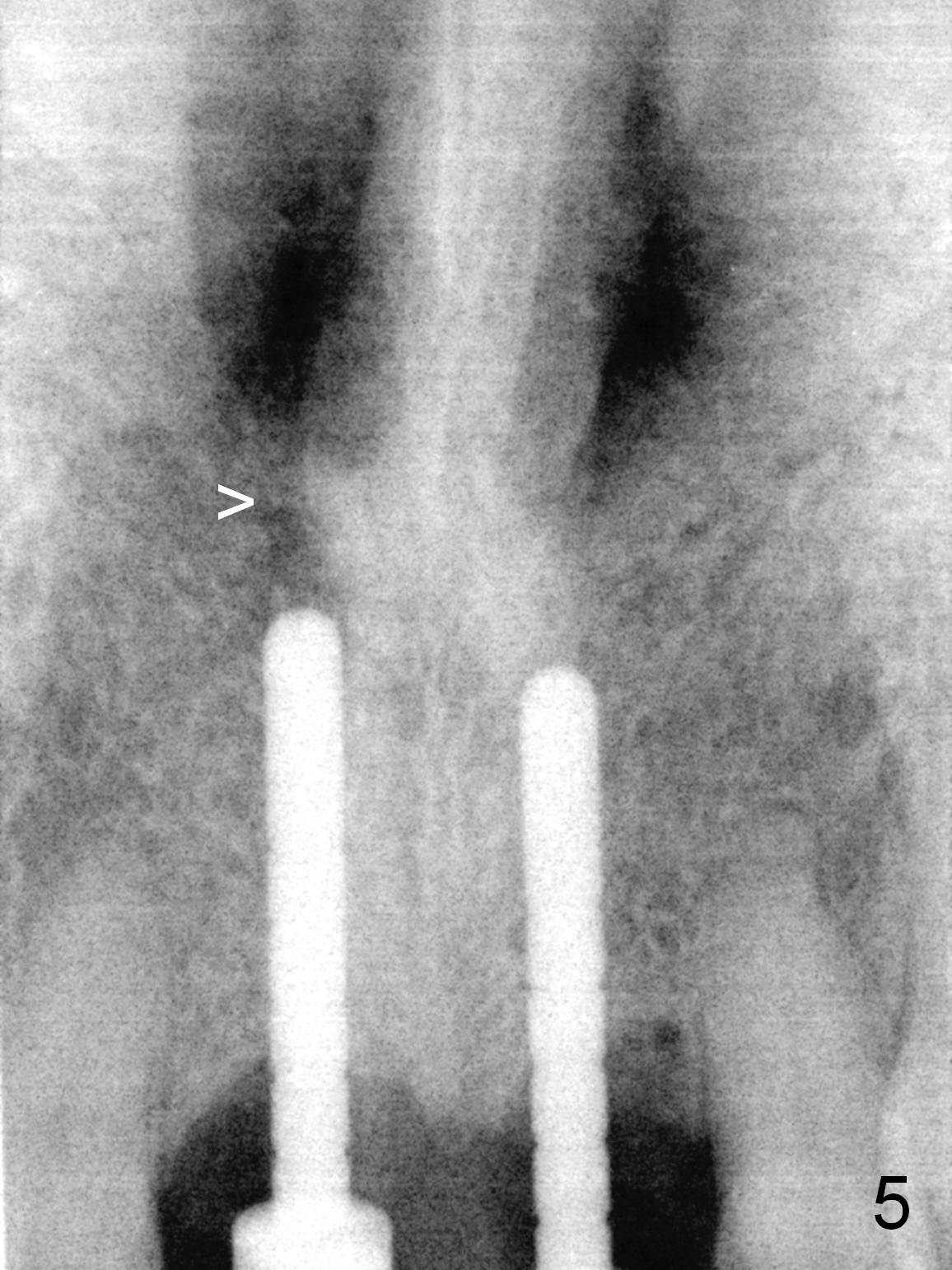
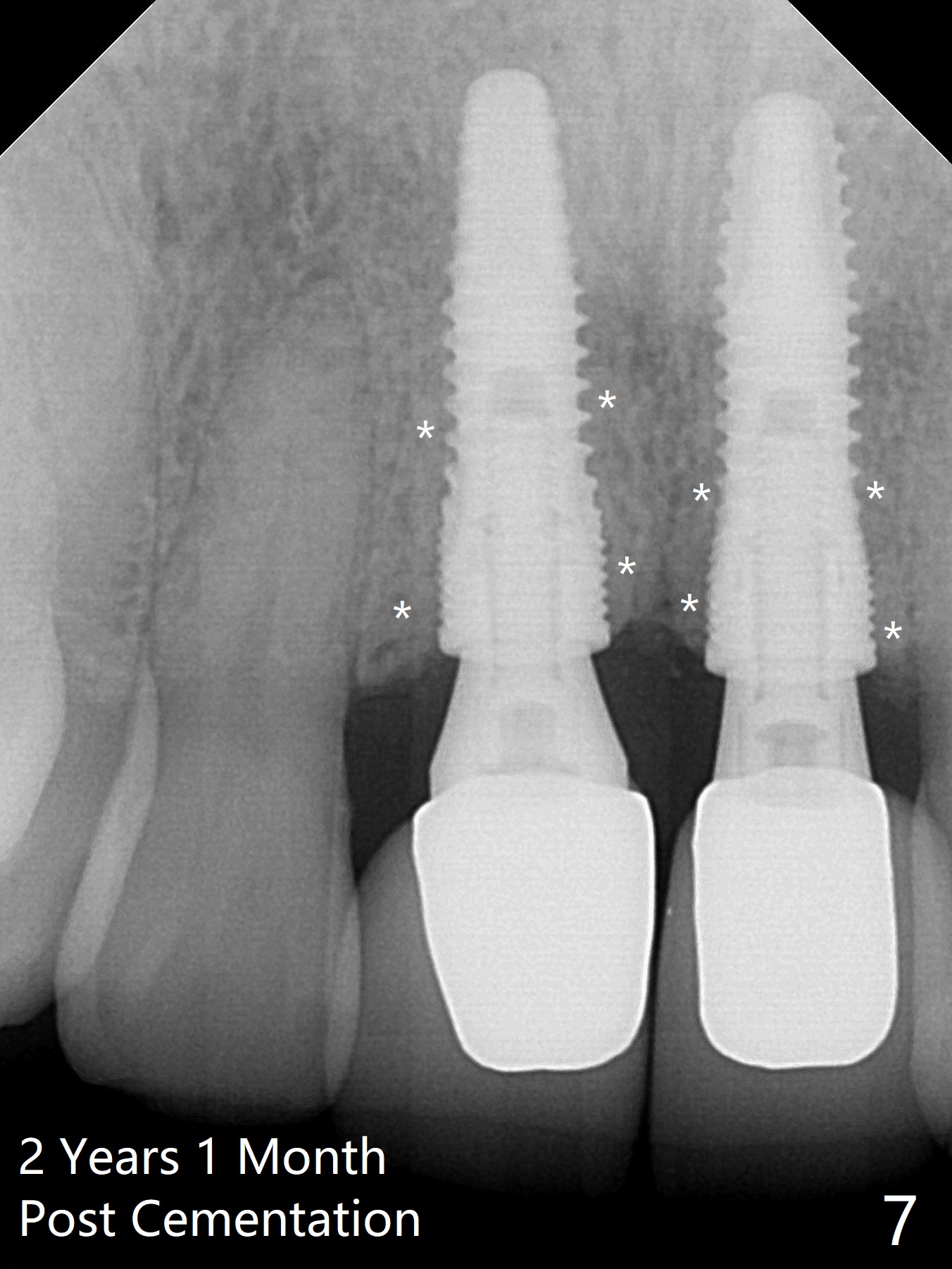
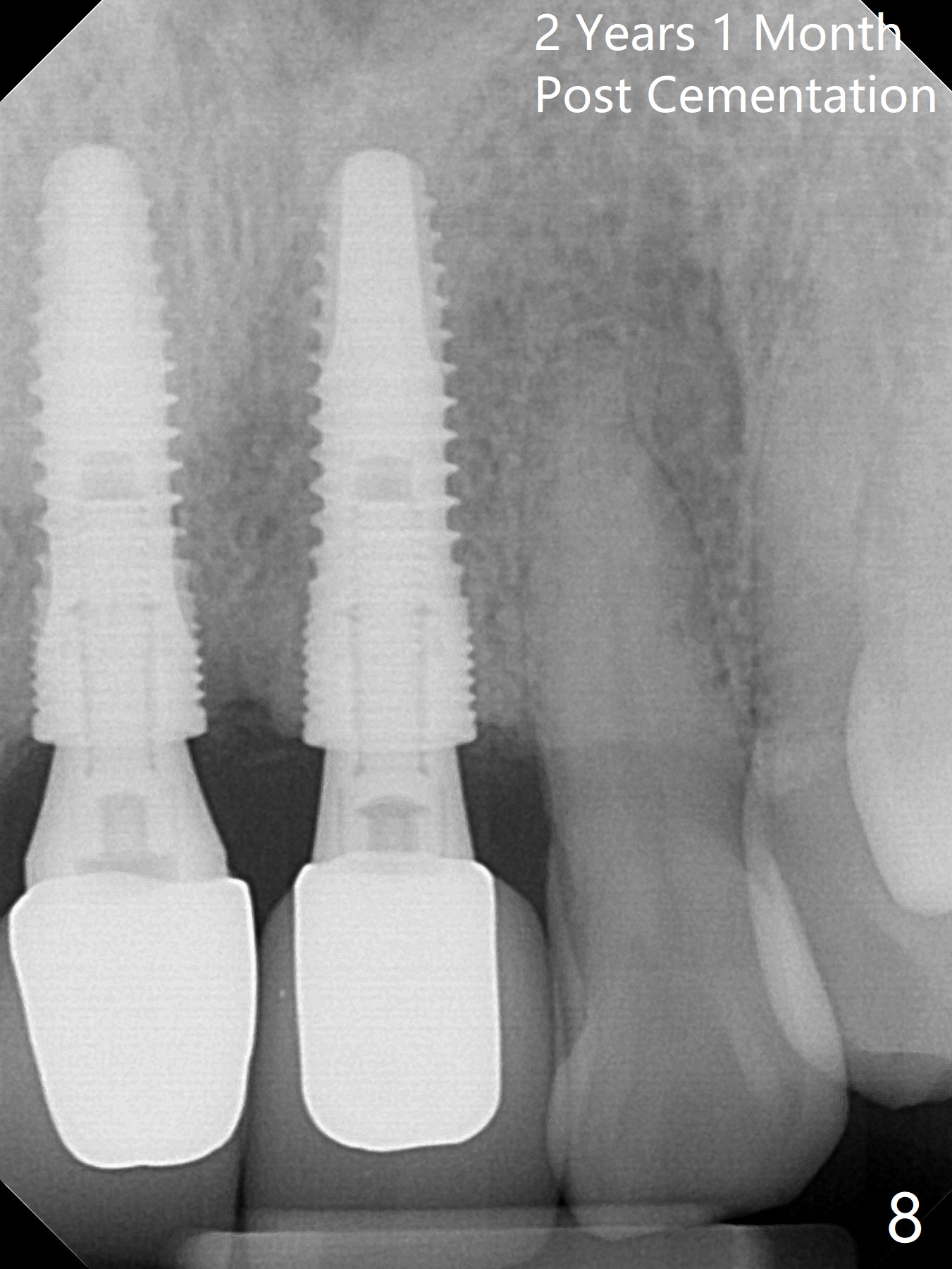
Fig.1 is the buccal view of the affected teeth (#8,9) with a fistula (>) after administration of local anesthetics (including 2% Xylocaine, 1:50,000 Epinephrine). The extraction socket at #8 is wide buccopalatal; the osteotomy will be initiated as palatal as possible (Fig.2 *), as shown in Fig.3-5 with parallel pins in place. When a 2 mm pilot drill is being used at #8, there is sudden empty feeling; the nasal floor is most likely perforated (Fig.5 >). When the parallel pin is removed from the osteotomy site of #8, there is moderate hemorrhage. Hemostasis is achieved when 4.1x14 mm implants are placed (Fig.6, insertion torque >50 Ncm). Temporary abutments (T) are placed for immediate provisionals. The patient returns for restoration almost 10 months postop. There is no bone loss 2 years 1 month post cementation (Fig.7). The bony structure around the coronal part of the implants is special (*). The gingiva looks healthy (Fig.9).
Return to Upper Incisor Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 11/24/2015, last revision 02/14/2019