




|
|
|
|
|
|
|
|
|
|
|
|
|
|
Repair Chipped Crown and Treat Perimplantitis
The abutment screw loosens several times when the temporary and permanent crowns are in place. Finally the lingual surface of the definitive restoration is over-trimmed with subsequent micro-fracture (Fig.1,2). When the posterior support is established with #18,19 implant crown cementation, repair of the incisal edge defect is attempted. The abutment screw access is sealed with cotton pellets and flowable composite, followed by packable one (Fig.3) with clearance (Fig.4).
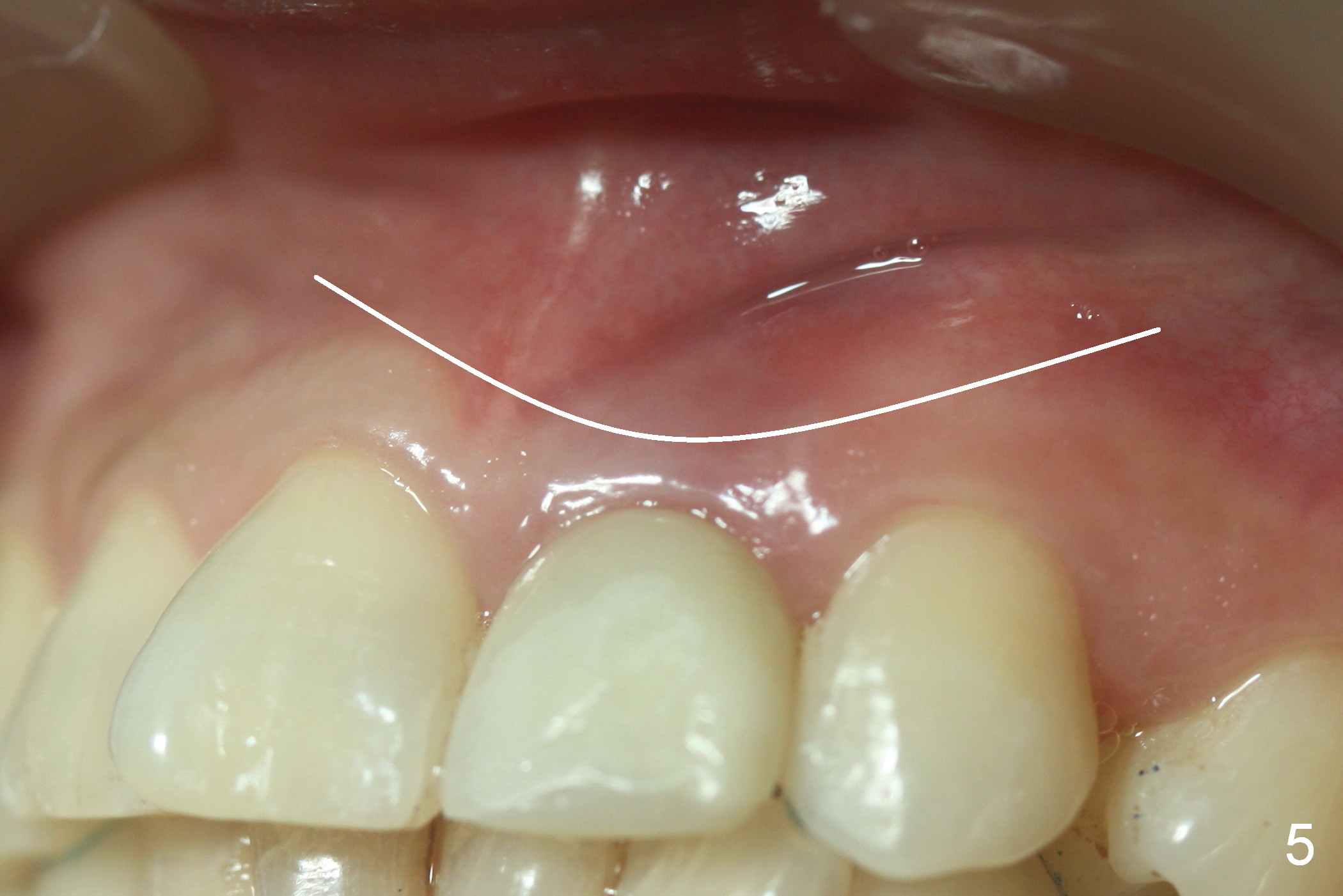
Purulent smell persists with labial gingival erythema 16 months post implant placement (Fig.1,3,5). It appears that bone graft is needed around the coronal threads. A semilunar incision will be made for access for cosmetic reason (Fig.5). PRF will be prepared. Titanium brush, Chlorhexidine, H2O2, NS and Metronidazole should be available in the surgical field. Photos are to be taken immediately preop.
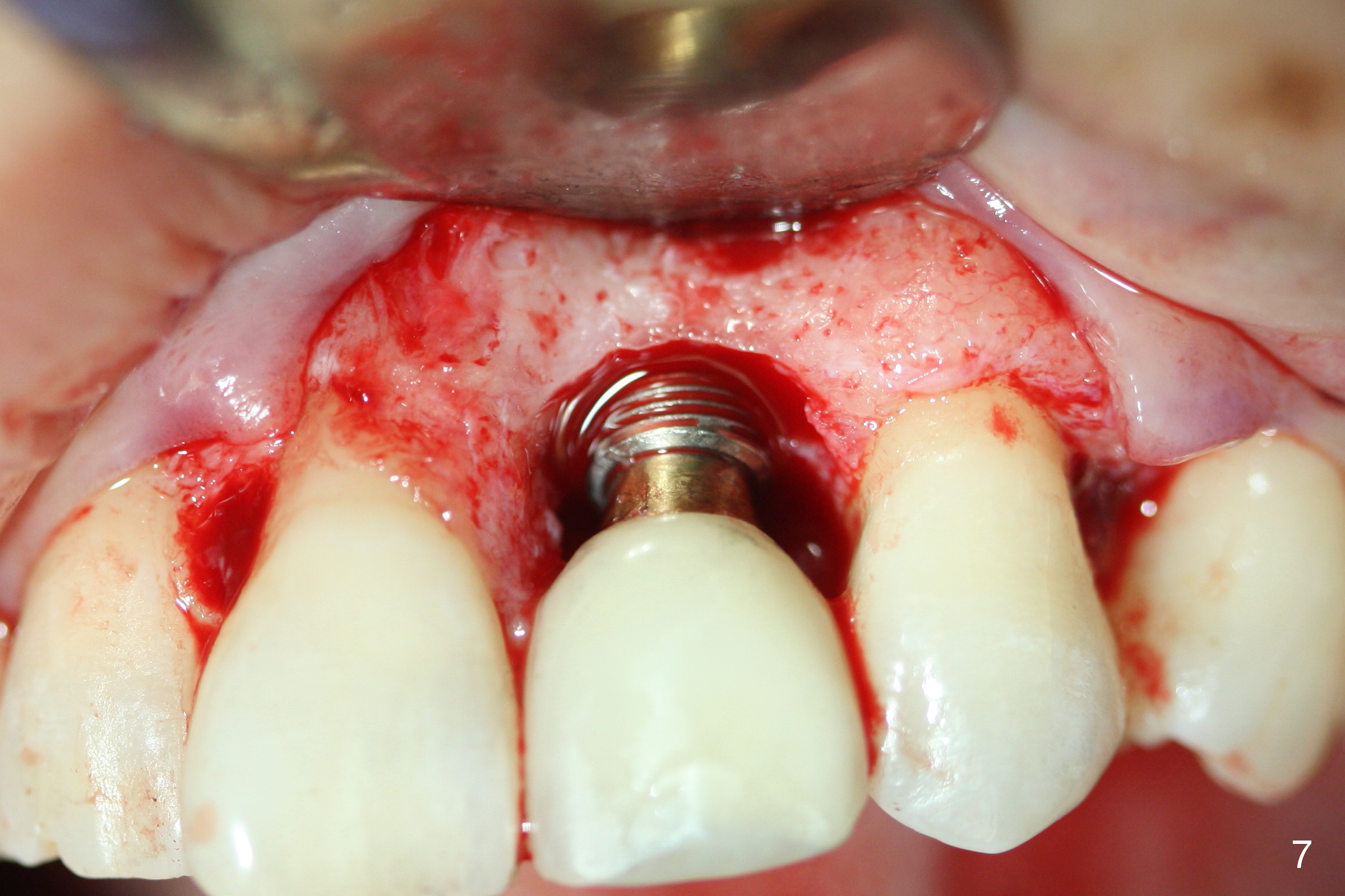
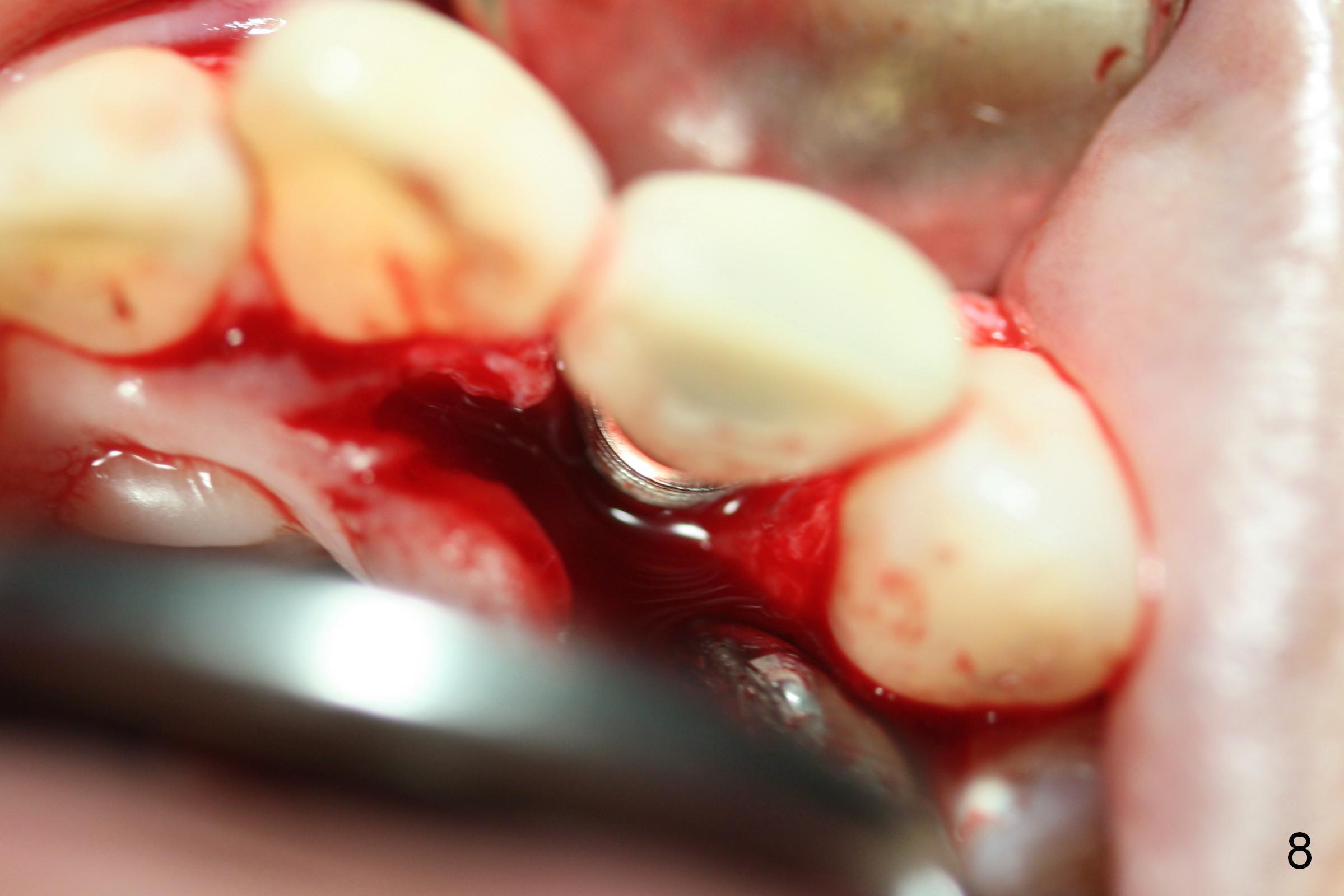
In spite of good oral hygiene due to waterpik, there is persistent gingival hemorrhage on brushing. Two months and a half later, surgical approach is adopted. Since the gingival margin at the affected area is lower than that of the neighboring teeth, gingival sulcus incision is made. The latter reveals resorbed bone margin (Fig.6 arrowheads) with granulation tissue. After removal of the latter, the implant threads are found to be exposed (Fig.7). The palatal sulcus incision reveals thread exposure apparently without granulation. More critical is that the implant is placed too palatally. After Titanium brush with Normal Saline irrigation, allograft is placed with PRF (limited amount) and 6-month membrane coverage. The implant should have been smaller than 4.5 mm and placed more apically with flap to avoid peri implantitis.
When the patient returns 3 weeks postop, gingival recession is evident with chief complaint of bone graft washout by water pik with light hemorrhage (Fig.9,10). If the gingival recession remains stable for another 2 months, a new crown will be fabricated. The patient agrees to have the implant removed 2 years 9 months post cementation.
Return to
Upper Incisor Immediate Implant,
Peri-implantitis
Xin Wei, DDS, PhD, MS 1st edition 07/10/2016, last revision 06/13/2018