|
|
|
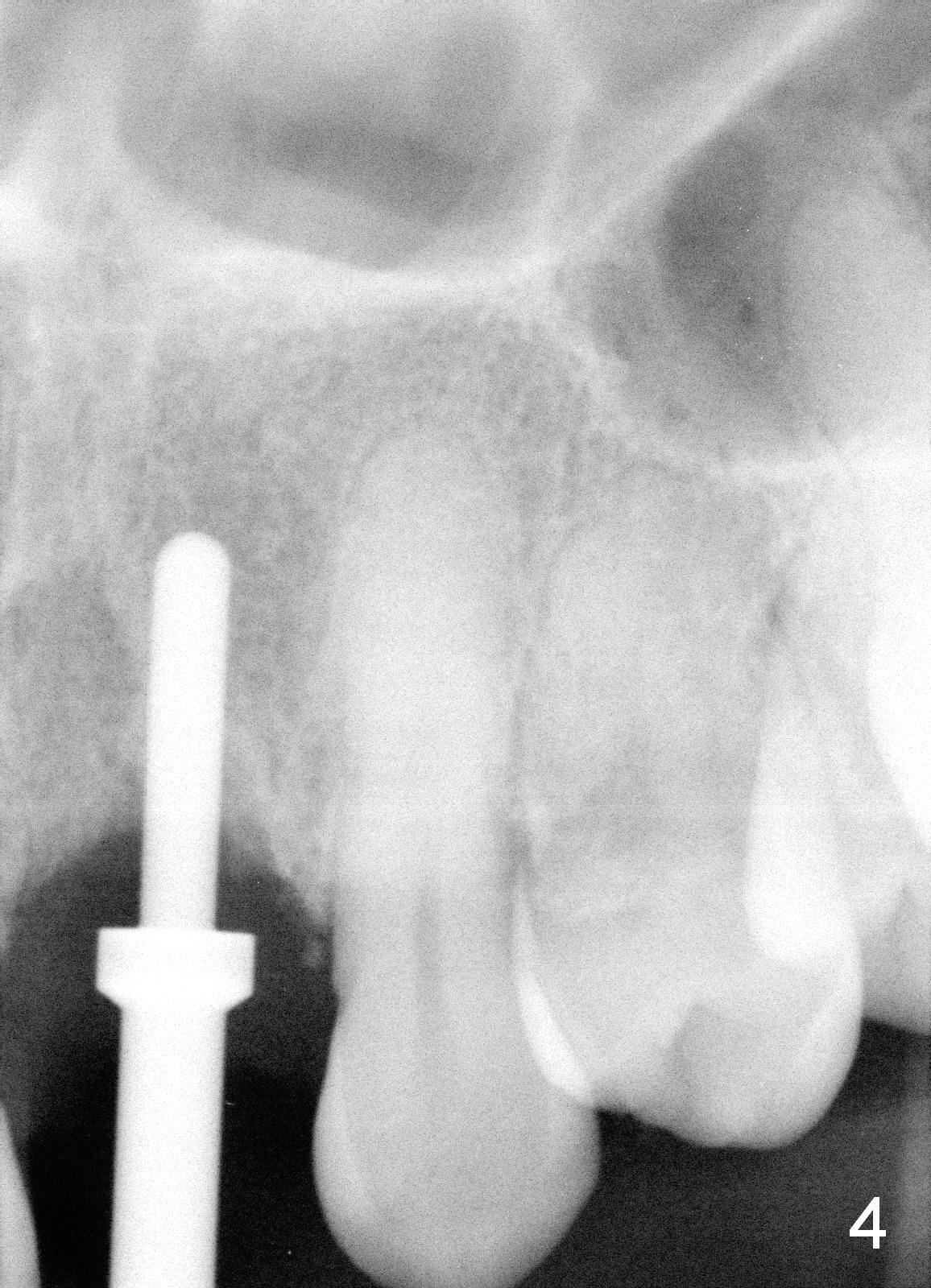
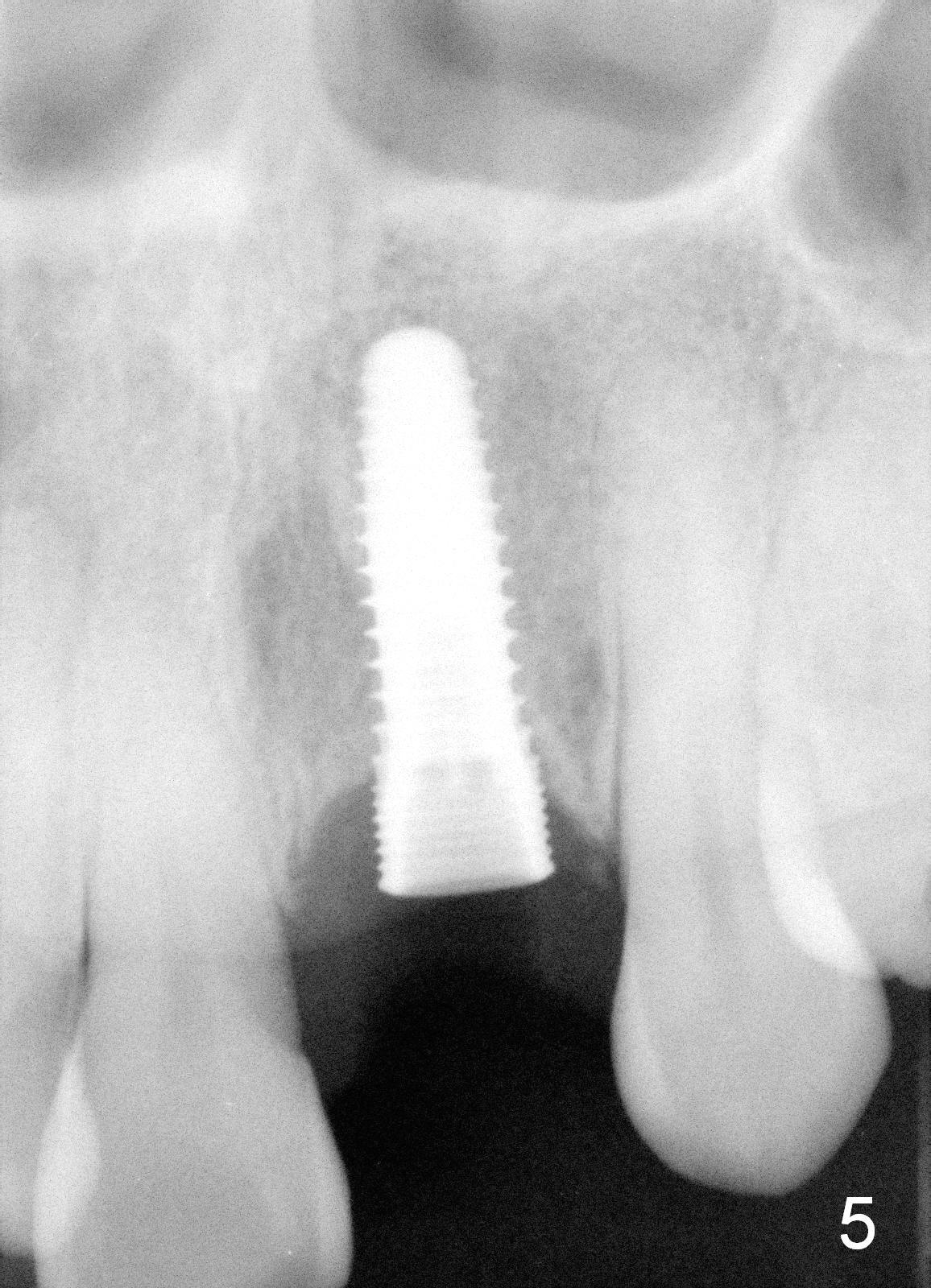
After extraction, exploration reveals that both the buccal and lingual plates are lost coronally. Mid buccal and lingual crest is 5 mm from the gingival margin. Osteotomy is initiated in the lingual aspect of the shallow socket with a 2 mm pilot drill 14 mm from the gingival margin. The bone density feels low. A parallel pin is inserted (Fig.4). Then the osteotomy extends to 18 mm, followed by a 3.8 mm tapered drill at 16 mm and 4.1 at 14 mm. A 4.5x14 mm implant is placed with insertion torque >60 Ncm (Fig.5). The implant remains lingual, whereas there is an approximate 3 mm buccal gap, which will be bone grafted.
The implant plateau is at the most coronal crest level and approximately 2-4 mm from CEJ of the neighboring teeth. The crestal defect is expected to heal with bone graft.
Ideally the apex of the implant should not be too close to the nasal floor. In case segmental osteotomy is required, there is room for transverse cut.
Xin Wei, DDS, PhD, MS 1st edition 02/26/2015, last revision 01/19/2018