





|
|
|
|
|
|
|
|
||
|
|
|
|
|
Approaches to Narrow Ridge
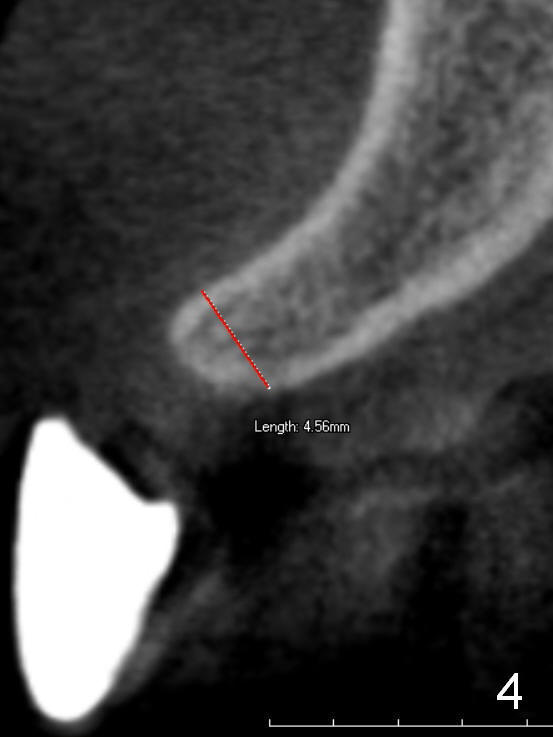
A man in his 50s returns to clinic for limited exam for the tooth #8 (possible occlusal trauma) 1.5 years after cementation of implant crown at the site of #7 (Fig.1). It appears that there is minimal bone resorption (mesial, >), as compared to the immediately postop PA (Fig.2). A narrow diameter implant must be a key to success (3.5x17 mm). Why narrow? Probably it is due to narrow mesiodistal space (Fig.3: 5.5 mm). This patient generally has wide buccolingual dimension, but at the site of #7, the ridge is 4.5 mm (Fig.4 CBCT coronal section).
How can the 3.5 mm implant be placed in the 4.5 mm ridge without obvious bone loss (Fig.7)? In fact, the implant was inserted by bone expansion using osteotomes (Fig.5,6). It is a quite technique-sensitive approach.
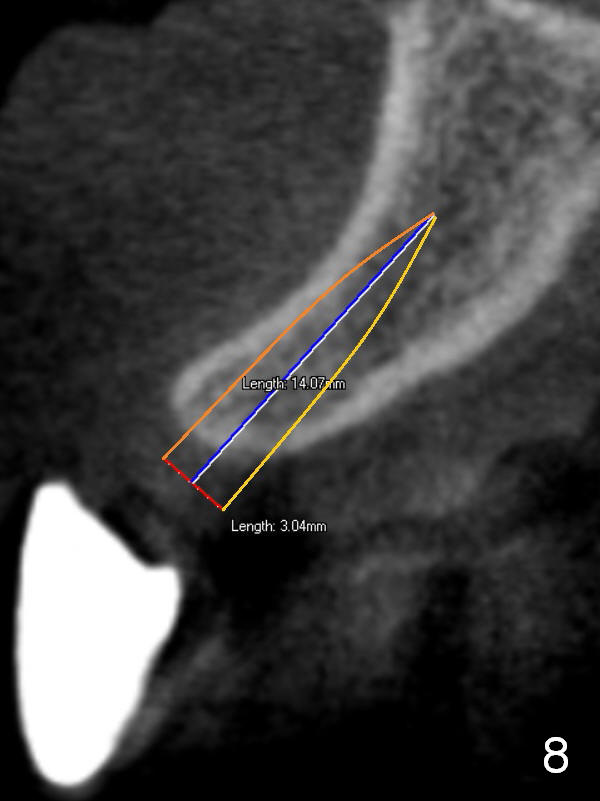
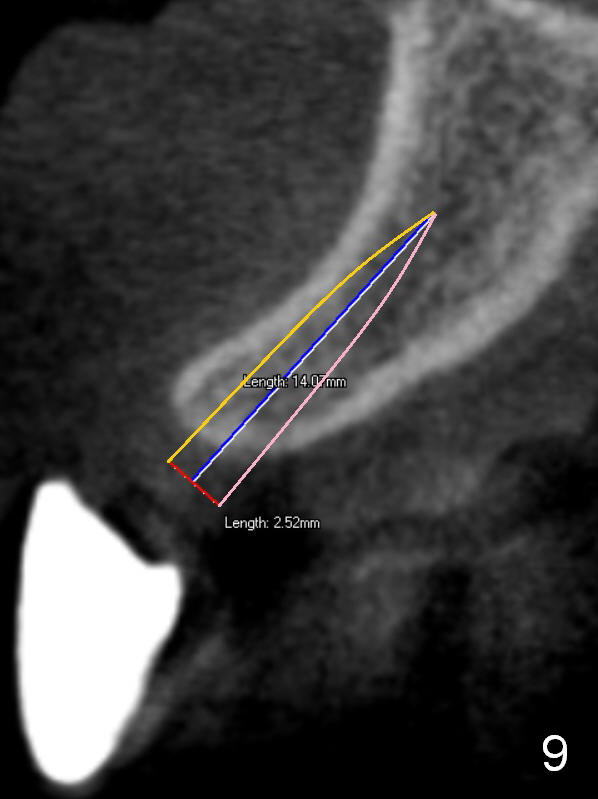
An alternative, probably safer one is to use narrower implants (3 mm (Fig.8) or 2.5 mm (Fig.9) one piece). A key to either approach is to start osteotomy as palatal as possible for restoration and the thin buccal plate. To avoid the disadvantage, try to place immediate implant as much as possible for a non restorable tooth.
Return to Upper Incisor
Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 04/12/2015, last revision 01/19/2018