





|
|
|
|
|||
|
|
|
|
|
||
|
|
|
|
|||
|
|
|
|
|
|
|
Immediate Repositioning Implant
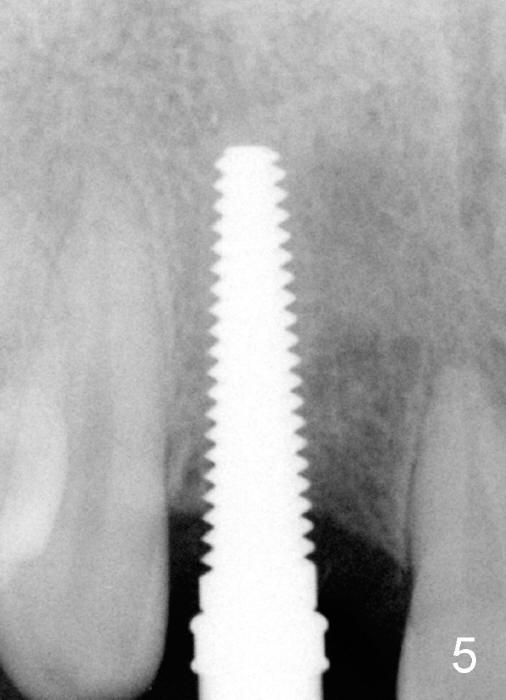
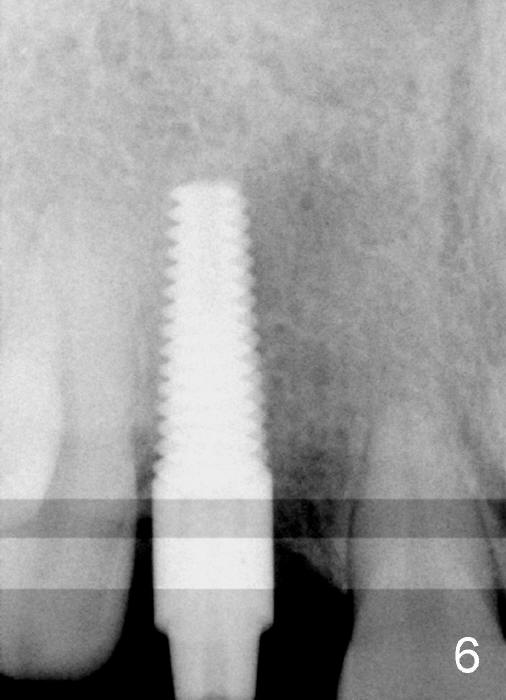
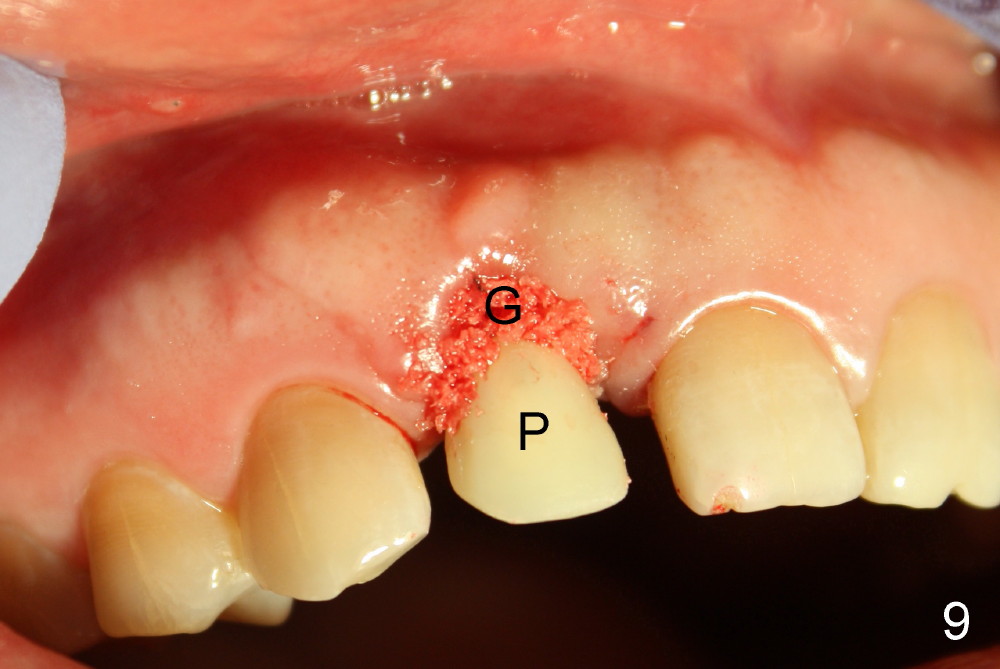
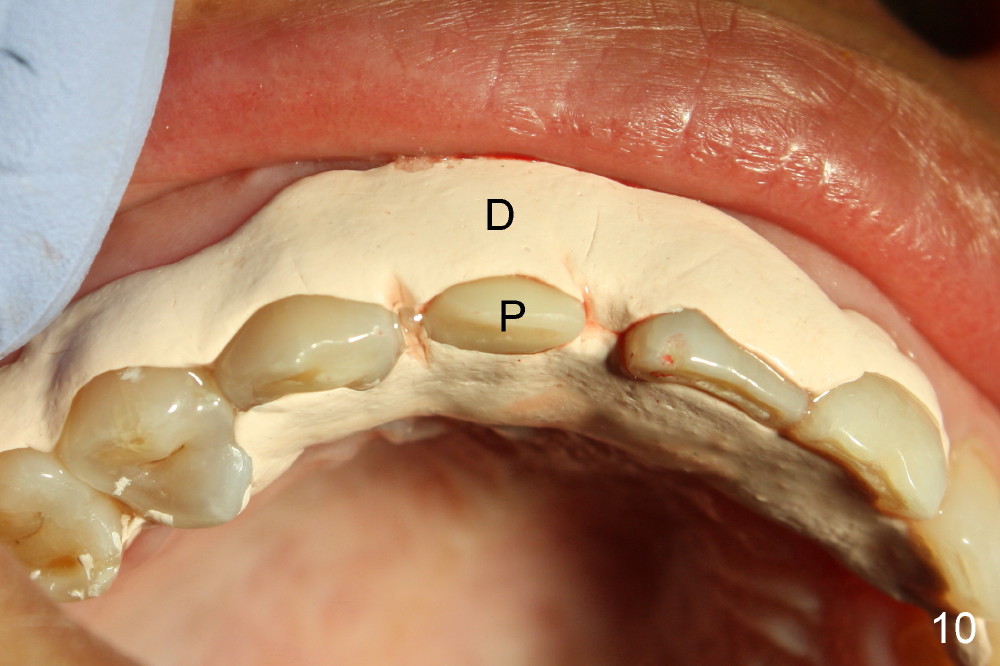
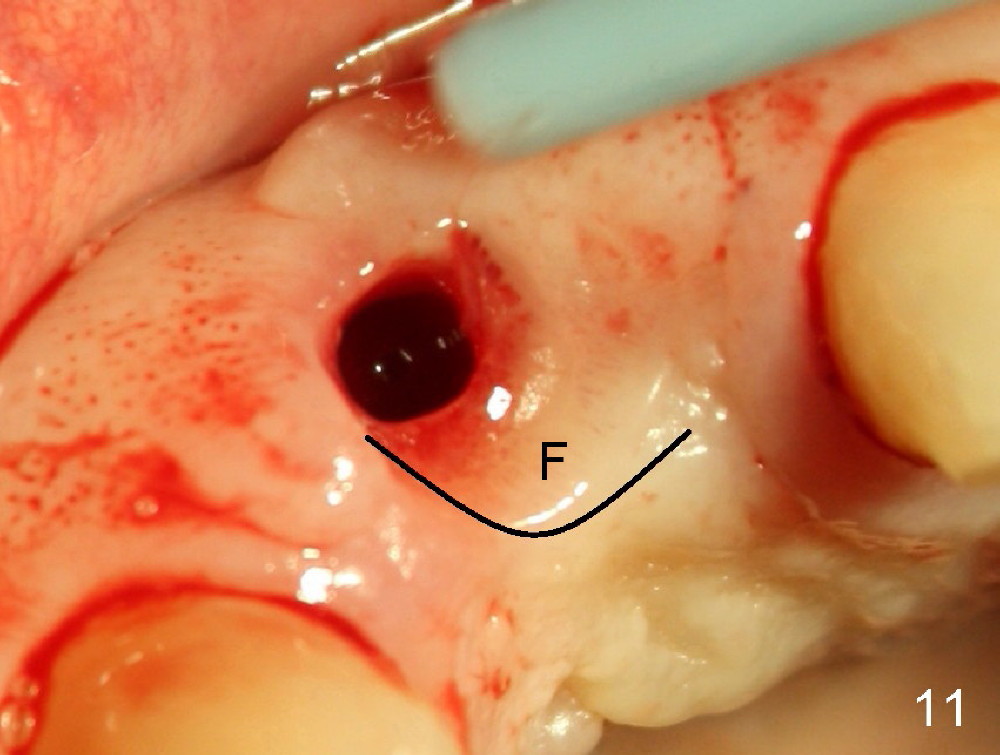
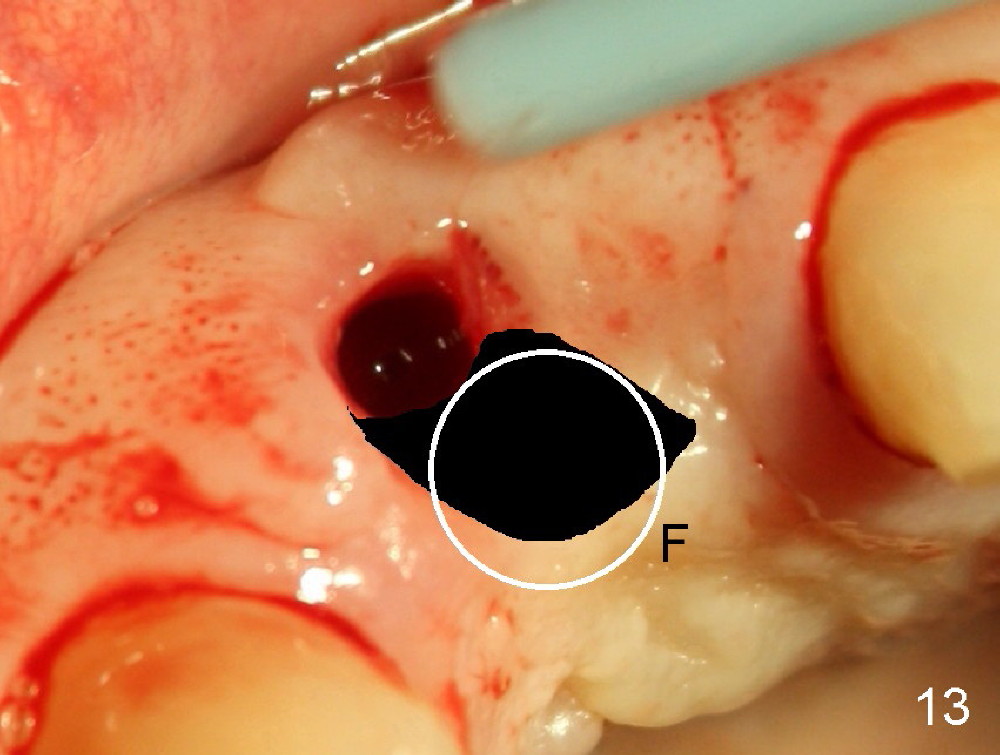
Malpositioned implant in the anterior region is cosmetically unacceptable. Immediate provisional allows us to note the issue immediately. The crown looks too long. Secondly, the provisional is easily dislodged, since the buccal aspect of the angled abutment is over trimmed (Fig.1). The implant (3.8x14 mm), which has been placed 3.5 months, is unexpectedly easily removed by reverse torque (Fig.2). The buccal wall is intact, whereas there seems to be enough bone lingually to place an implant. A small incision is made (Fig.11) so that the gingival tissue can be transferred buccally (Fig.12) and the immediate implant is to be placed palatally (Fig.13 white circle). There is no difficulty forming osteotomy in the palatal wall, followed by inserting 4.5x20 mm tap at the depth of 17 mm (Fig.3,5). But the tap is not palatal enough (Fig.4). By removing more palatal bone, the 4.5x17 implant (Fig.6) appears to be placed palatally enough for restoration (Fig.7; A: abutment; *: buccal gap). The biggest problem is that the palatal flap (Fig.7 arrowheads) cannot be pushed buccally; instead remains palatally. This leads to buccal tissue deficiency (Fig.8). Connective tissue graft is offered, but declined. The patient insists that she has low smile line. Following immediate provisional, mixture of allograft and synthetic graft is placed in the buccal gap (Fig.9). The overbuilt graft is held in place by perio dressing.
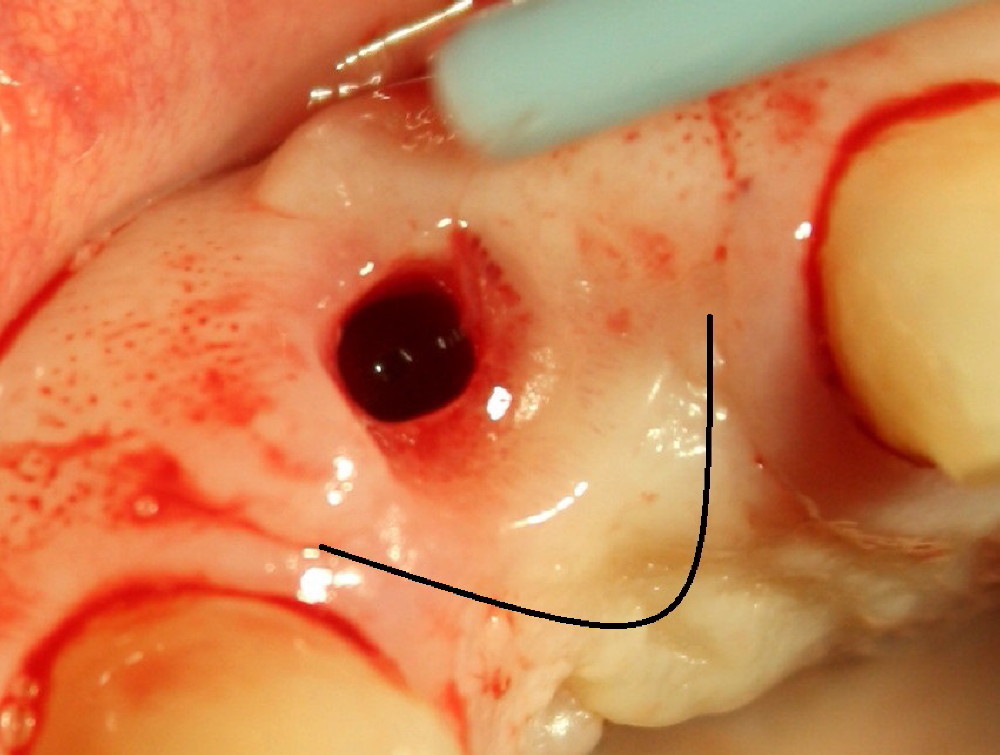
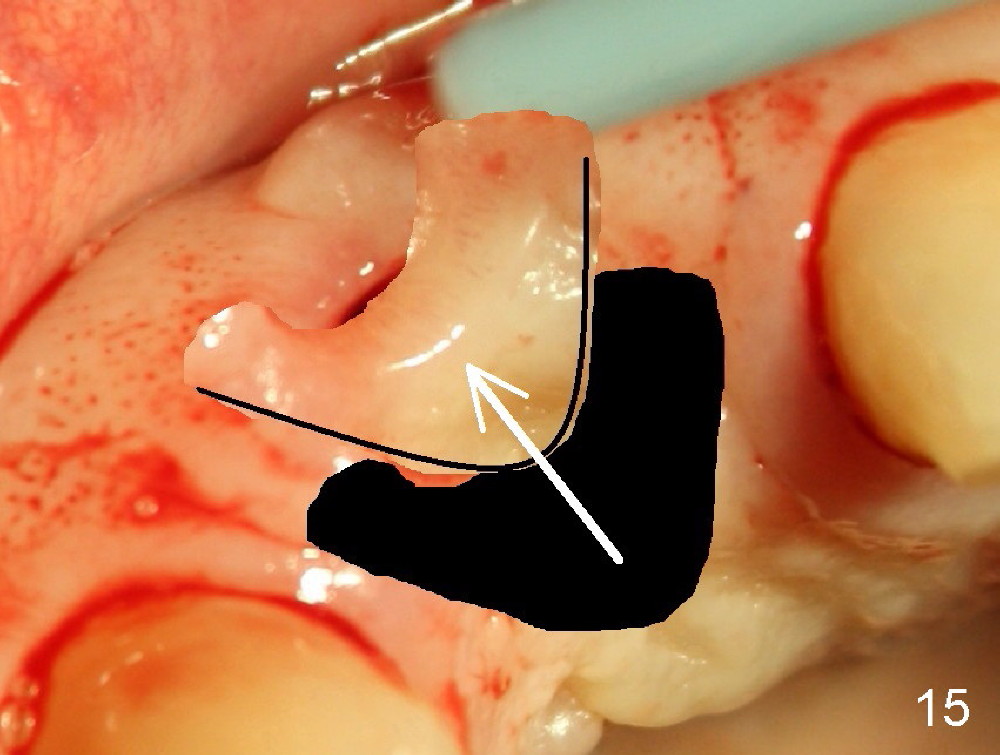
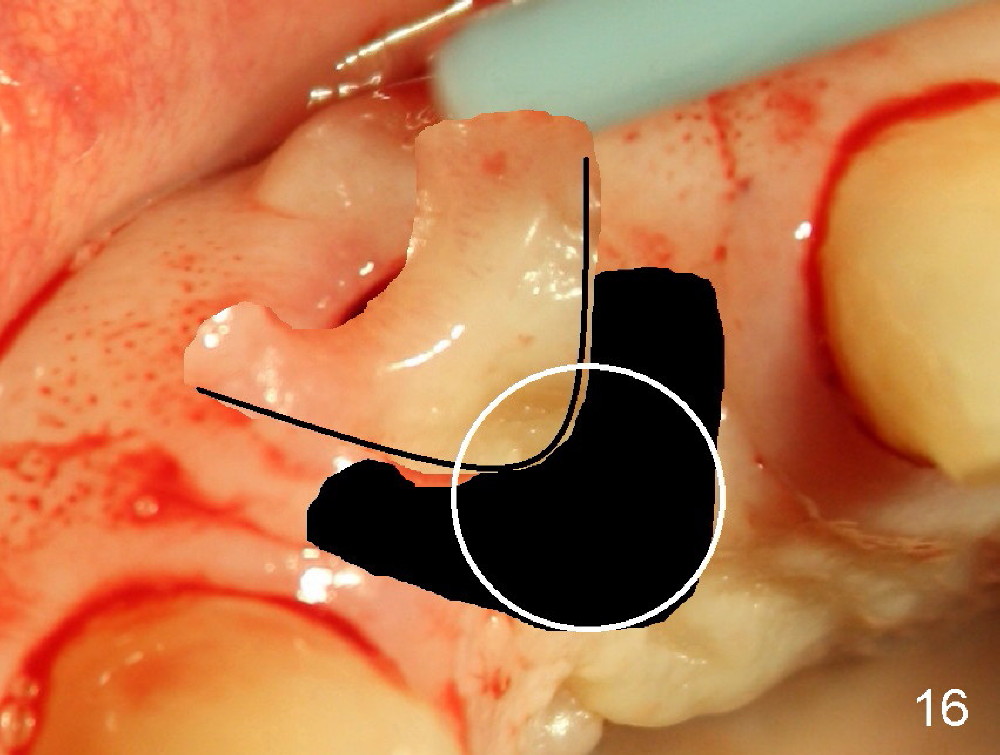
If a larger incision were made (Fig.14) and the flap were dissected freely (Fig.15), the buccal tissue deficiency would be less (Fig.16). Follow up is shown 2 3.
Return to Upper Incisor Immediate Implant, Professionals
Xin Wei, DDS, PhD, MS 1st edition 07/10/2014, last revision 03/01/2015