


|
|
|
|
|
|
|
|
Severe Gingival Recession with Medical Conditions
A 65-year-old man has history of Type II diabetes and stroke. He is taking a blood thinner (Xarelto 20 mg qd). The tooth #11 has been mobile for several years. Fig.1 is a CBCT taken 2 years 8 months earlier. The affected tooth has now supraerupted (Fig.2 arrow) with apical abscess (arrowhead).
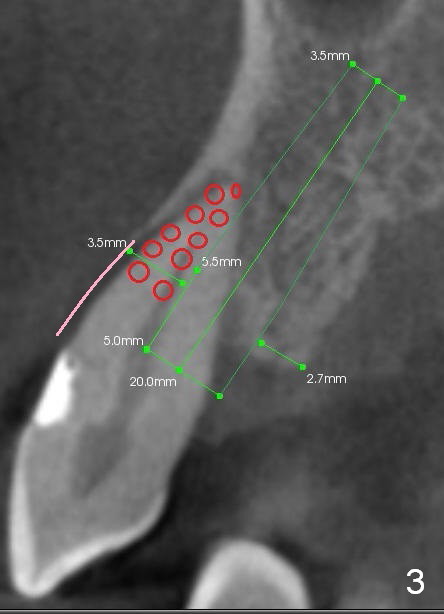
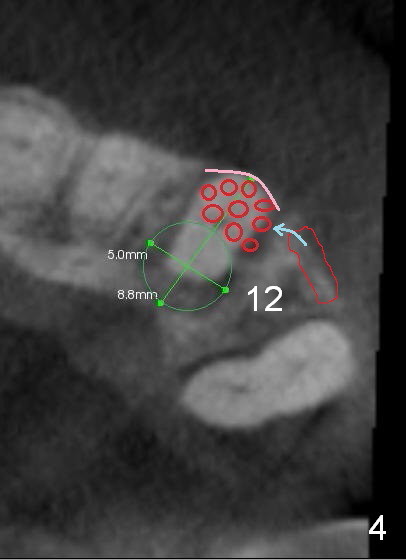
Bone defect at present should be more severe than CBCT coronal (Fig.3) and axial (Fig.4) sections indicate. After palatal placement of a 5x20 mm tissue level implant (Fig.3 green area) and an appropriate abutment, an immediate provisional is to be fabricated. A block graft is harvested from #12 edentulous region (buccal plate) to the buccal defect at the site of #11 (Fig.4 curved light blue arrow). Prepare surgical handpiece and chisels. The remaining bony defect will be filled with allograft and Osteogen (red circles). The graft site is going to be covered by Osteotape (Fig.3,4 pink curved line), while the donor site is given mixture of allograft and Osteogen and Collagen Dressing. When the soft tissue deficiency is found, connective tissue graft is to be harvested from the palate. If visibility is compromised for these steps, an incision will be made as shown in Fig.5. This should be done with caution considering the medical conditions. Before surgery, ask the patient whether the blood thinner has stopped for a few days or not and how diabetes control is.
How does the surgery turn out to be?
Return to Upper
Cuspid Immediate Implant
尖牙即种
Xin Wei, DDS, PhD, MS 1st edition 03/21/2015, last revision 05/29/2021