







|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
PA after Pilot Drill
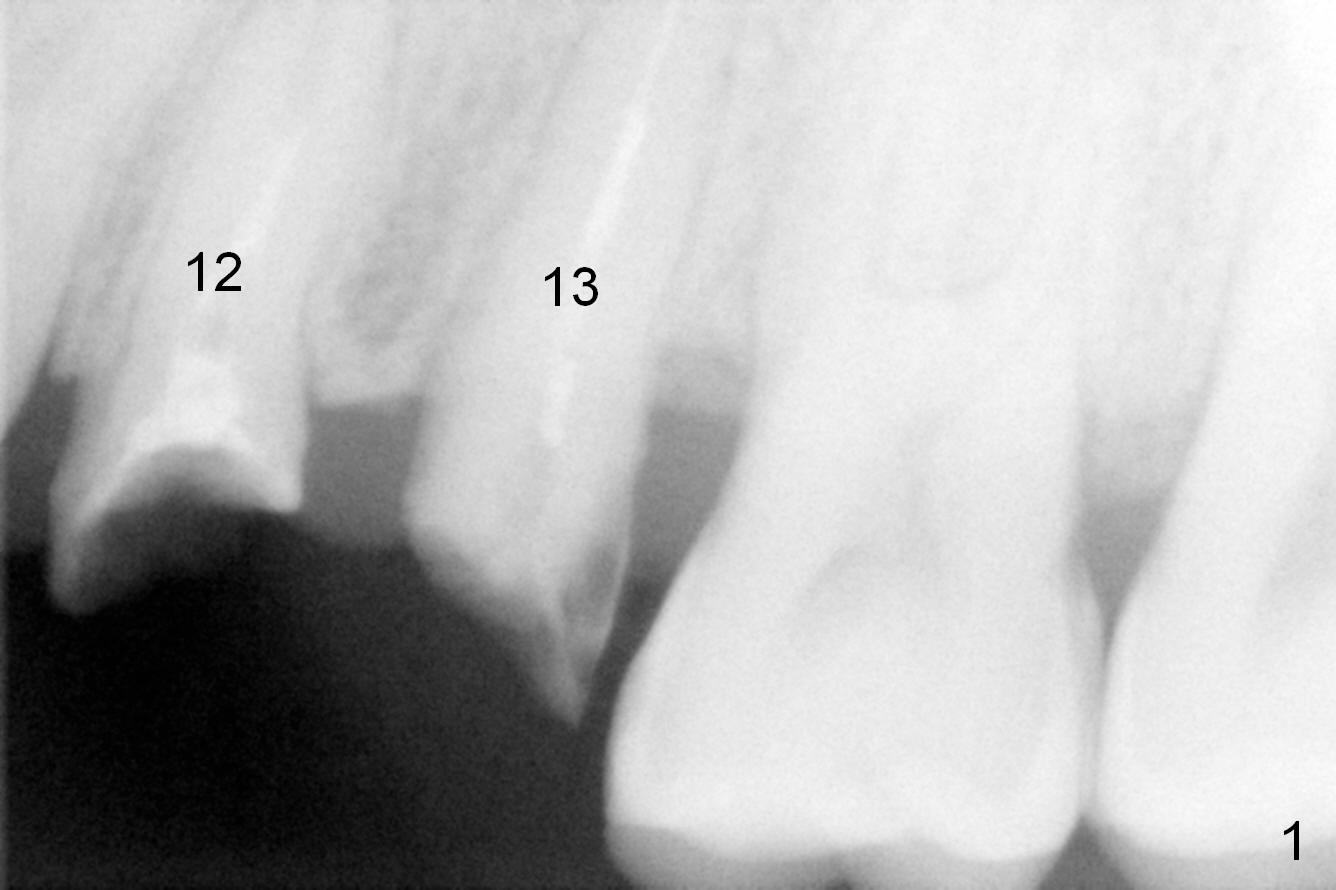
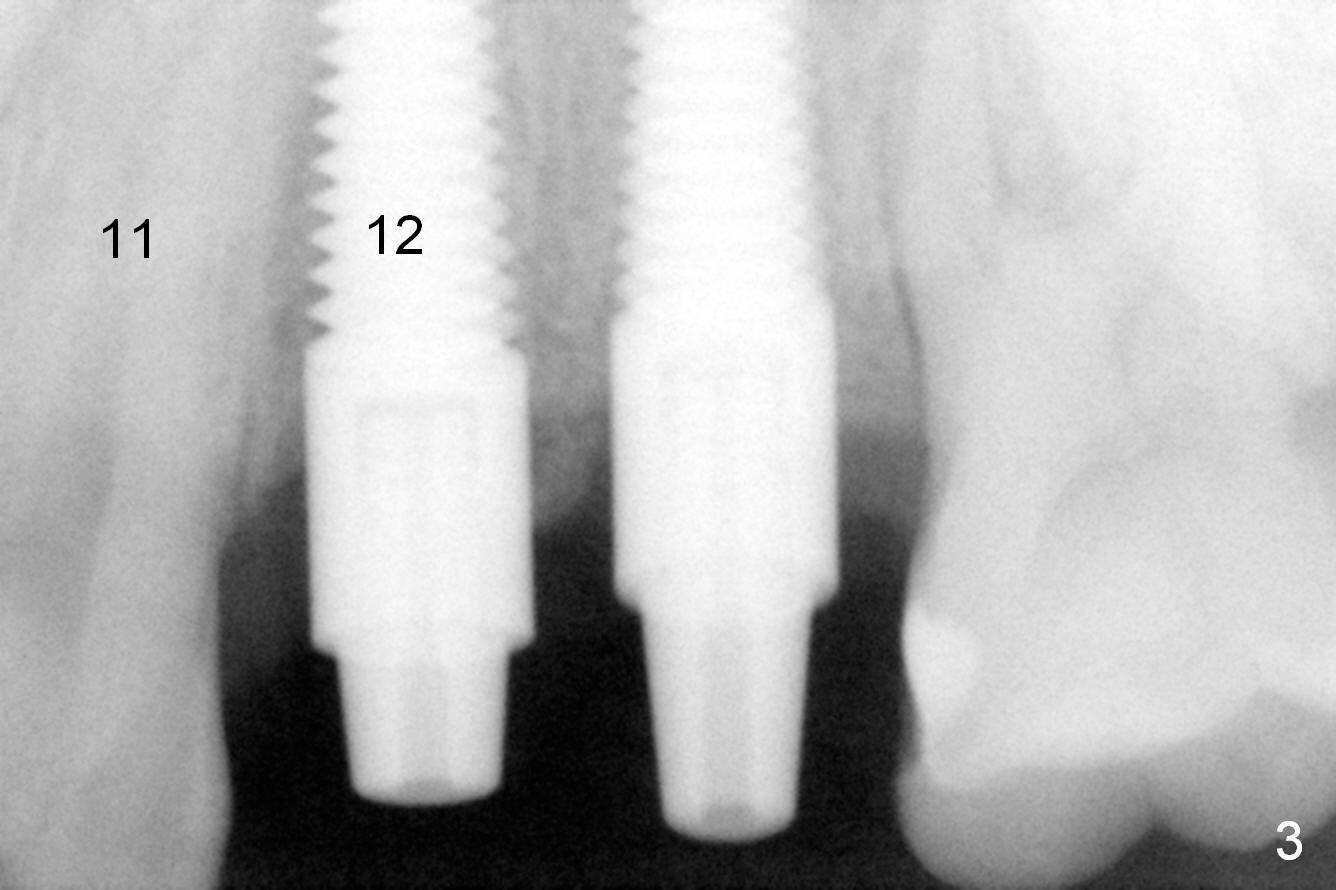
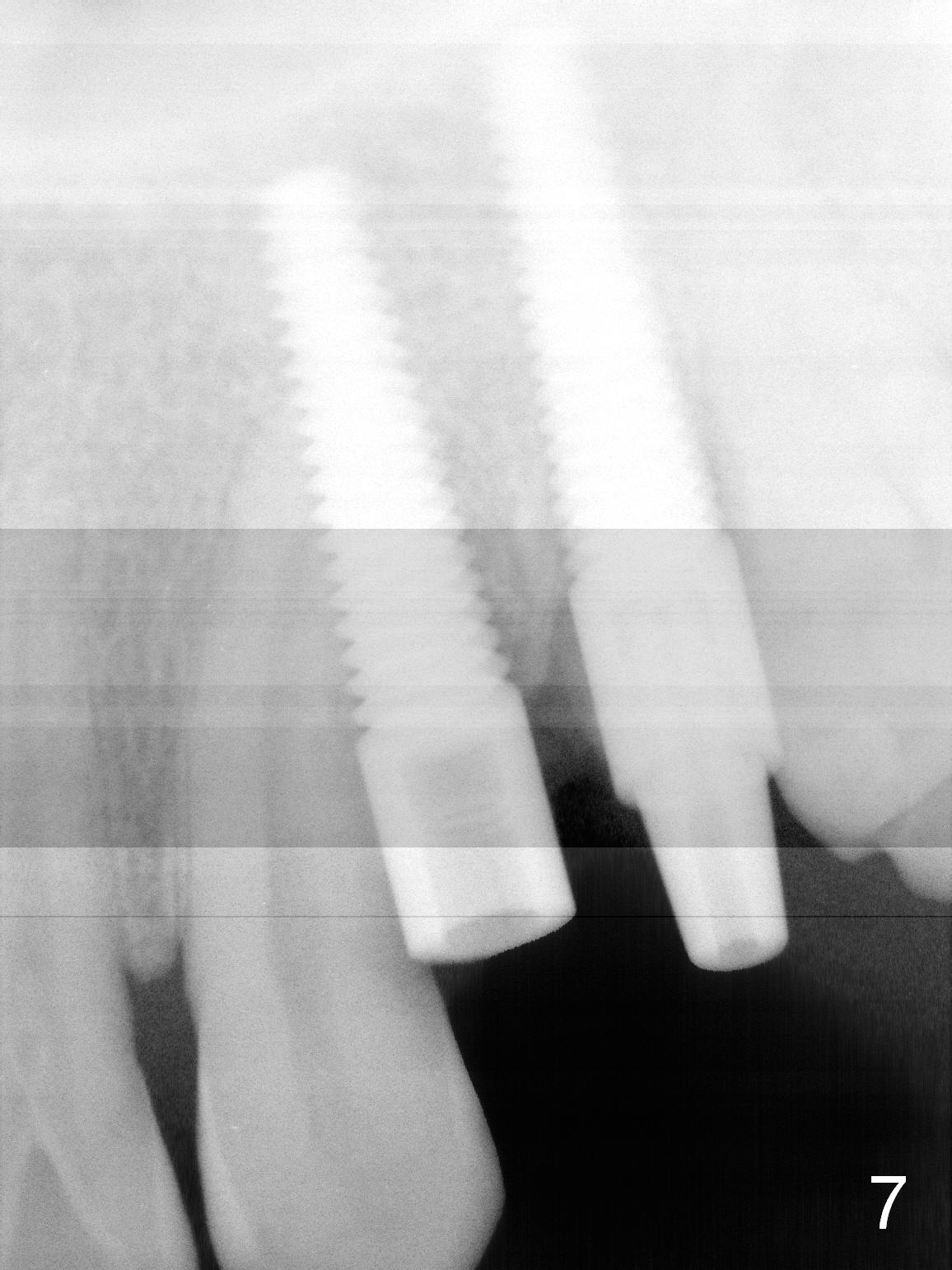
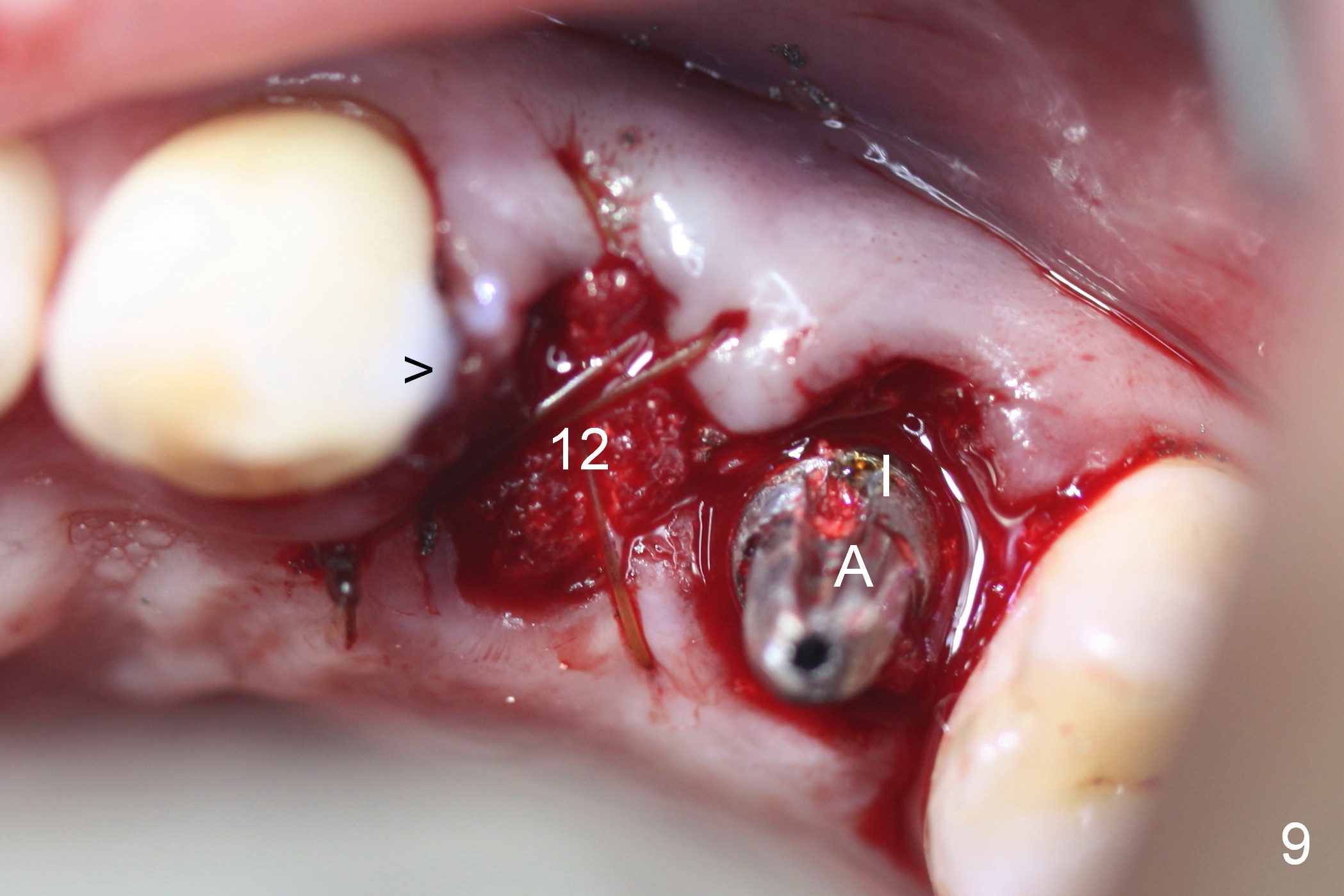
Taking 2 additional PAs with sensor 1 is frustrating (Fig.1,2), no apices shown. Osteotomy is done smoothly with 2 mm pilot drill at 20 mm, 2.5 mm reamer at 17 mm, and 3 mm reamer at 14 mm and 4.5x20 mm tap at 17 mm. The 1st intraop PA is taken with sensor 1 when 2 of 4.5x20 mm implants are placed (Fig.3); the implant at #12 is close to the root of the tooth #11. The 2nd PA is taken with sensor 2: the apex of #11 touches the implant at #12 (Fig.4). There is no separation when panoramic X-ray is taken (Fig.5). Effort is exerted to re-direct the osteotomy twice (Fig.6: tap; Fig.7: implant) without success. When the implant is removed, a PA is taken; it appears that the root of the tooth #11 has no damage (Fig.8). To obtain the best recovery, socket preservation is carried out with 50/50 cortical/cancellous allograft mixed with Osteogen (Fig.12 *) and Collagen Dressing (Fig.9: #12). A 2 (or 3)-unit provisional bridge (Fig.10: #12,13) is fabricated over the implant (Fig.9 I)/abutment (A) to cover these 2 sockets. After acid etching #11 D surface (Fig.9 >) and relining (Fig.11 *), the provisional bridge is bonded to the tooth #11 (Fig.11,12 black >) so that bone graft will be less likely dislodged.
In brief, PA should be taken after pilot drill, no matter how easy the case seems to be. It is difficult to change trajectory later on. Careful analysis of preop PA is equally important. Implant should not be placed outside of PA. The patient will return for #12 implant placement for the 2nd time 2.5 months postop.
Return to Upper Premolar Immediate Implant
前磨牙即种
Xin Wei, DDS, PhD, MS 1st edition 08/13/2015, last revision 05/02/2021