


|
|
|
|||
|
|
|
|
|
|
|
|
|
|||
Bone-level Immediate Implant for Upper Molar
A 60-year-old man has poor dentition (Fig.1). The tooth #3 is symptomatic with a mesiobuccal fistula. PA shows large periapical radiolucency associated with the mesiobuccal root (Fig.2 *). It appears that the tooth is non-salvageable. The roots of this tooth are widely furcated. The septum should be large unless destroyed by infection.
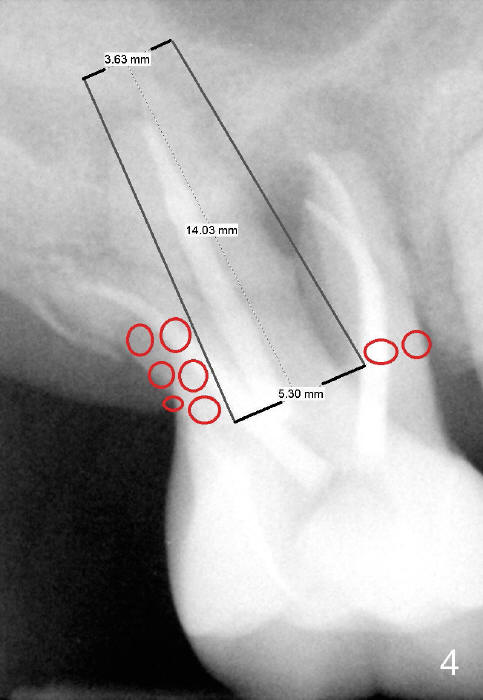
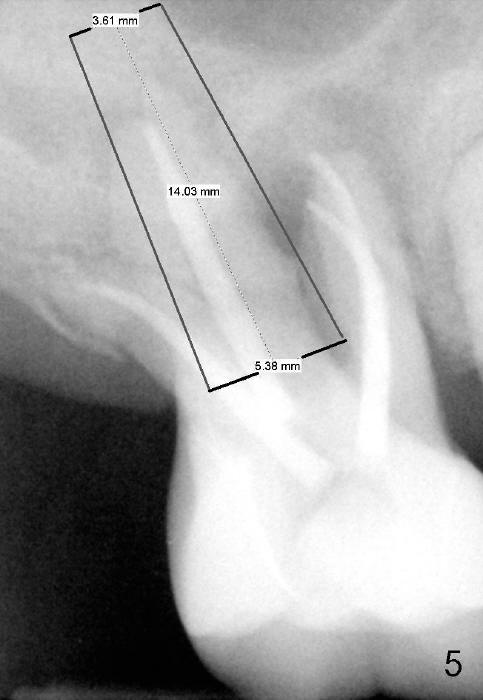
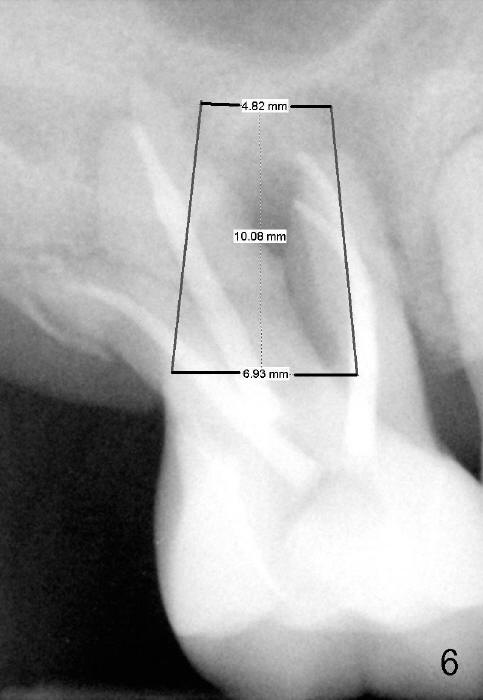
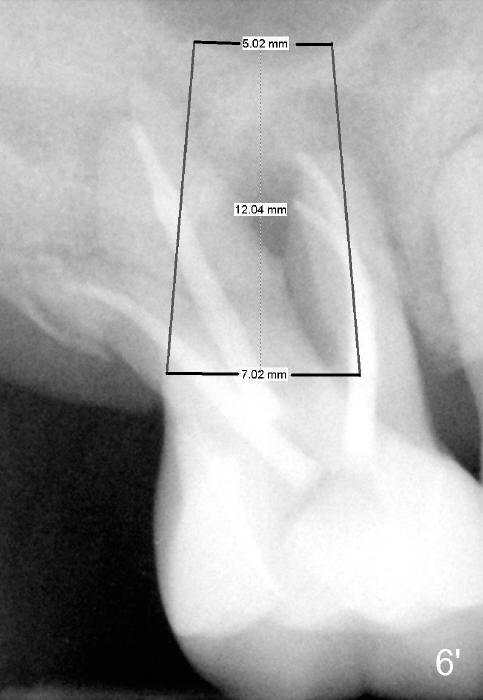
If the septum is basically intact, a 5.3x12 bone-level implant is placed in an ideal trajectory for restoration (Fig.3). The mesial and distal margin of the implant is at the level of the alveolar crests (arrows); bone graft is placed evenly to cover the coronal threads (red circles). If the septum is defective to some degree, a longer implant is placed distally (Fig.4) with more bone graft placed distally. Or the implant is placed deeper (Fig.5). If the septum is severely defective, an extra wide, but shorter implant (6.9x10 mm bone-level SM) is used (Fig.6). Or an extra wide UF implant with extra 2 mm length may offer better primary stability (Fig.6' (with sinus lift)). The primary stability of the extra wide implants is derived from contact with the mesial and distal socket walls.
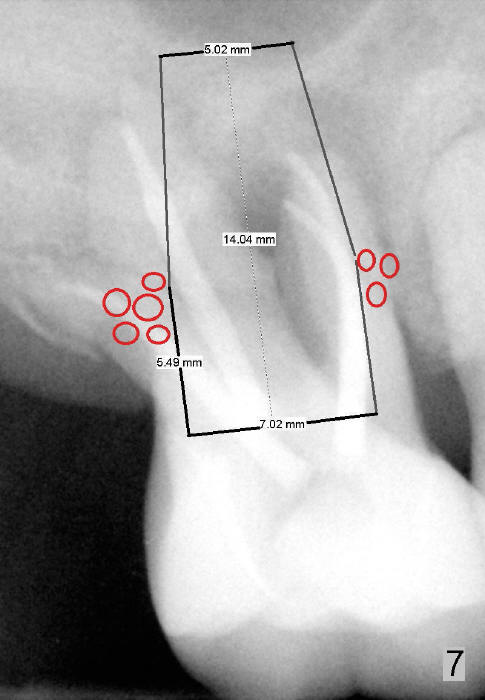
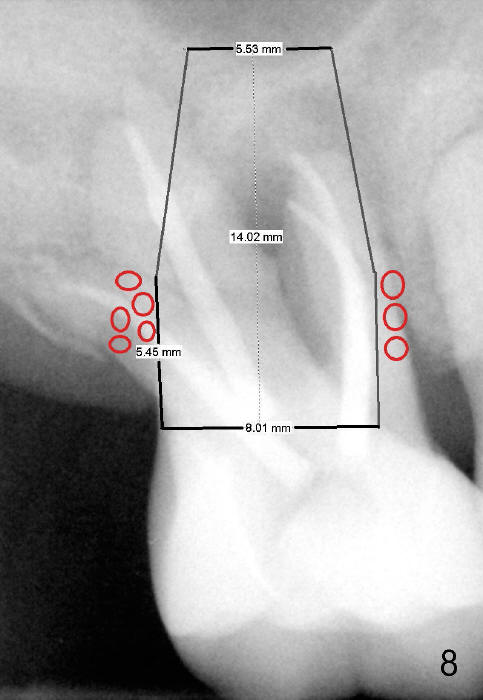
If primary stability is questionable with the bone-level implants mentioned above, a 7x14 mm gingiva-level implant will be the next alternative (Fig.7). If primary stability is still insufficient, a 7x17 mm (with sinus lift) or 8x14 or 17 mm will be placed (Fig.8). The larger the implant, the less bone graft is used (compare Fig.7,8).
Return to Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 01/01/2015, last revision 01/01/2015