|
|
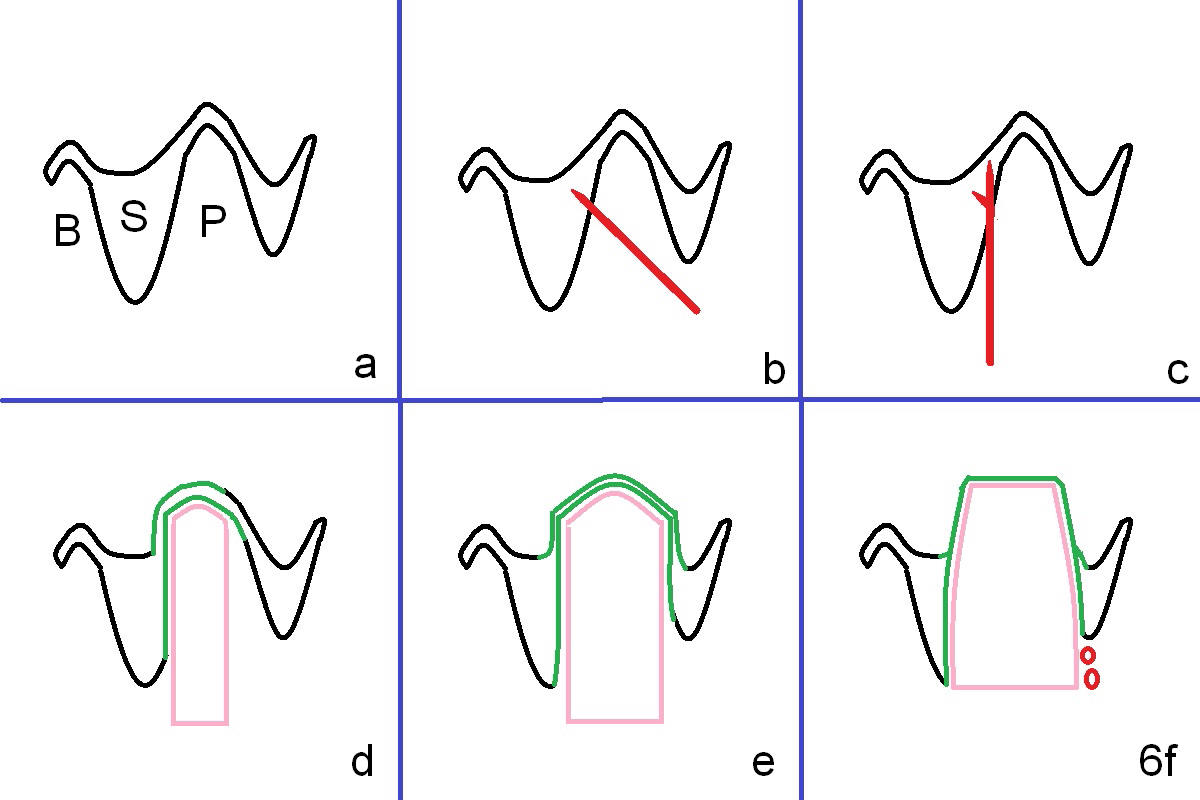
Fig.6a is an illustration of the socket after extraction (bucco-palatal section). The septal (S) bone may be longer than the palatal wall. B, P: buccal and palatal sockets.
By time sequence, this case will be the 1st case of the control group of local antibiotic study. After extraction, the socket will be packed with gauze saturated with 2% Xylocaine with 1:50,000 Epinephrine. Hemostasis helps remove infected granulation tissue and identify anatomic structures of the socket. Most likely, osteotomy is initiated in the palatal wall of the septum obliquely (Fig.6b).
Once penetrating the wall, the trajectory of the pilot drill will be changed so that the coronal end will be in the center of the socket (Fig.6c).
With combination of osteotomes and reamers (Fig.6d,e pink), the sinus floor will be lifted (green lines); at the same time, the osteotomy will be shifted palatally by itself due to the slope of the palatal wall of the septum.
Finally a bone-level implant is placed (Fig.6f) with bone graft covering the exposed threads (red circles). Place Osteotape inside the socket against the gingiva prior to bone grafting.
Xin Wei, DDS, PhD, MS 1st edition 08/06/2015, last revision 04/28/2018