|
|
|
|
|
|
|
|
|
|
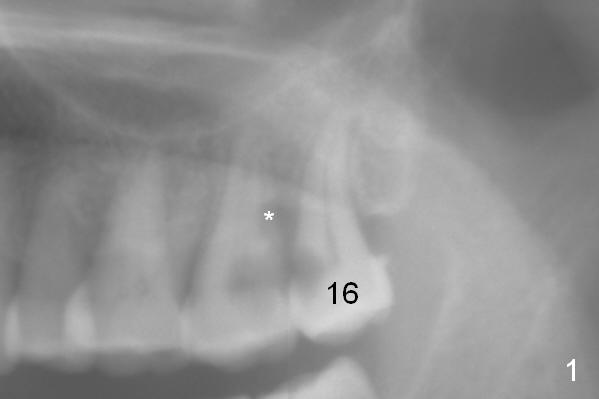
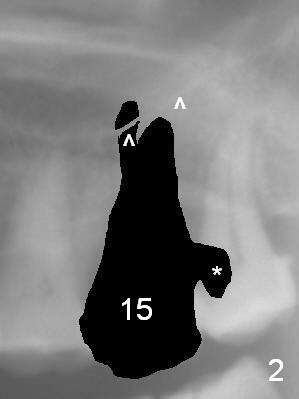
Keep Neighboring Tooth Temporarily as Reference for Implant Placement
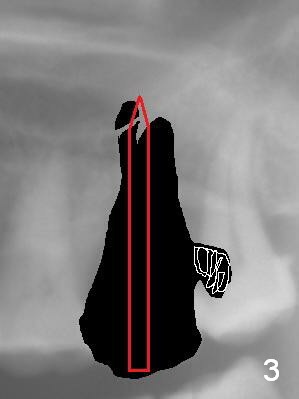
A 53-year-old woman has toothache in the upper left sextant. It appears that the teeth #15 and 16 are non-salvageable due to proximal root caries (Fig.1 *). The tooth #15 is extracted first and the socket will be packed with 2% Xylocaine, 1:50,000 Epinephrine gauze. The decay at #16 will be removed to reduce intraop contamination (Fig.3 *), followed by insertion of a piece of gauze (Fig.3 white). Rounded tapered (RT) osteotomes (Fig.3 red arrow) or drills will be used for sinus lift (Fig.1 ^: sinus floor). With the 3rd molar temporarily in site, the trajectory of the osteotomy is easily controlled.
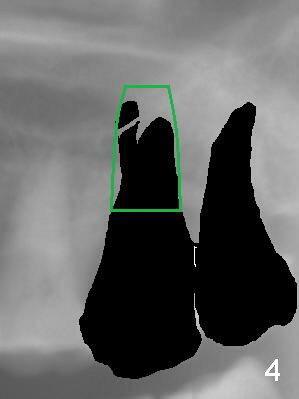
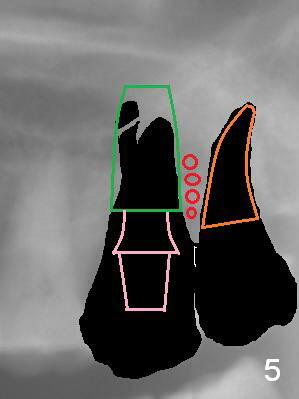
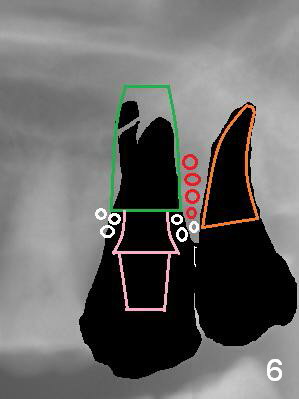
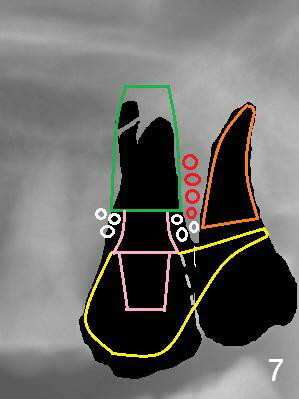
Once an implant is placed at the site of #15, the tooth #16 is extracted (Fig.4). With a piece of gauze in the implant well, allograft/Osteogen is placed around the implant (Fig.5 red circle), while collagen plug in the socket of #16 (Fig.5 brown) if necessary. After removal of the gauze from the implant well, an abutment is placed (Fig.5 pink). More graft is placed around the implant shoulder (Fig.6 white circles). An immediate provisional at #15 could be extended distally to cover the #16 socket (Fig.7 yellow). Two weeks later the provisional is modified (Fig.7 grey dashed line) to remove the distal extension.
Return to
Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 05/06/2016, last revision 05/26/2019