


.jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Extensive Crack Line
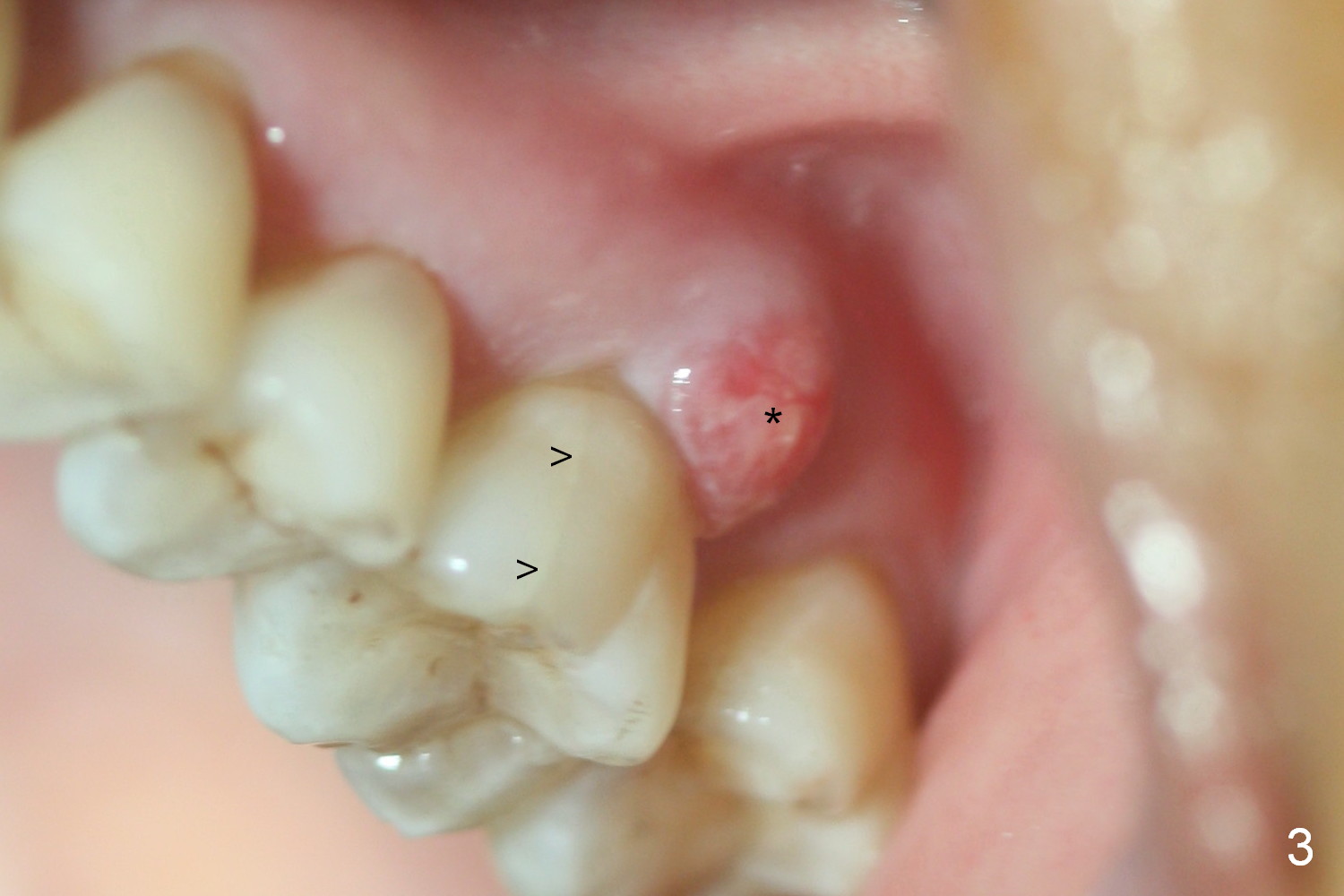
Approximately 2 months ago, the patient had vague pain in the upper left quadrant. The tooth #15 appeared to have crack tooth syndrome. Recently she developed severe pain and saw a periodontist. When she returns to our office, there is an obvious crack line lingually (Fig.1 <) with a nearby abscess (*). The crack line happens to be visible in X-ray (Fig.2 black <). The buccal abscess is larger (Fig.3 *); more surprising is hardly visible mesiobucal crack line (>).
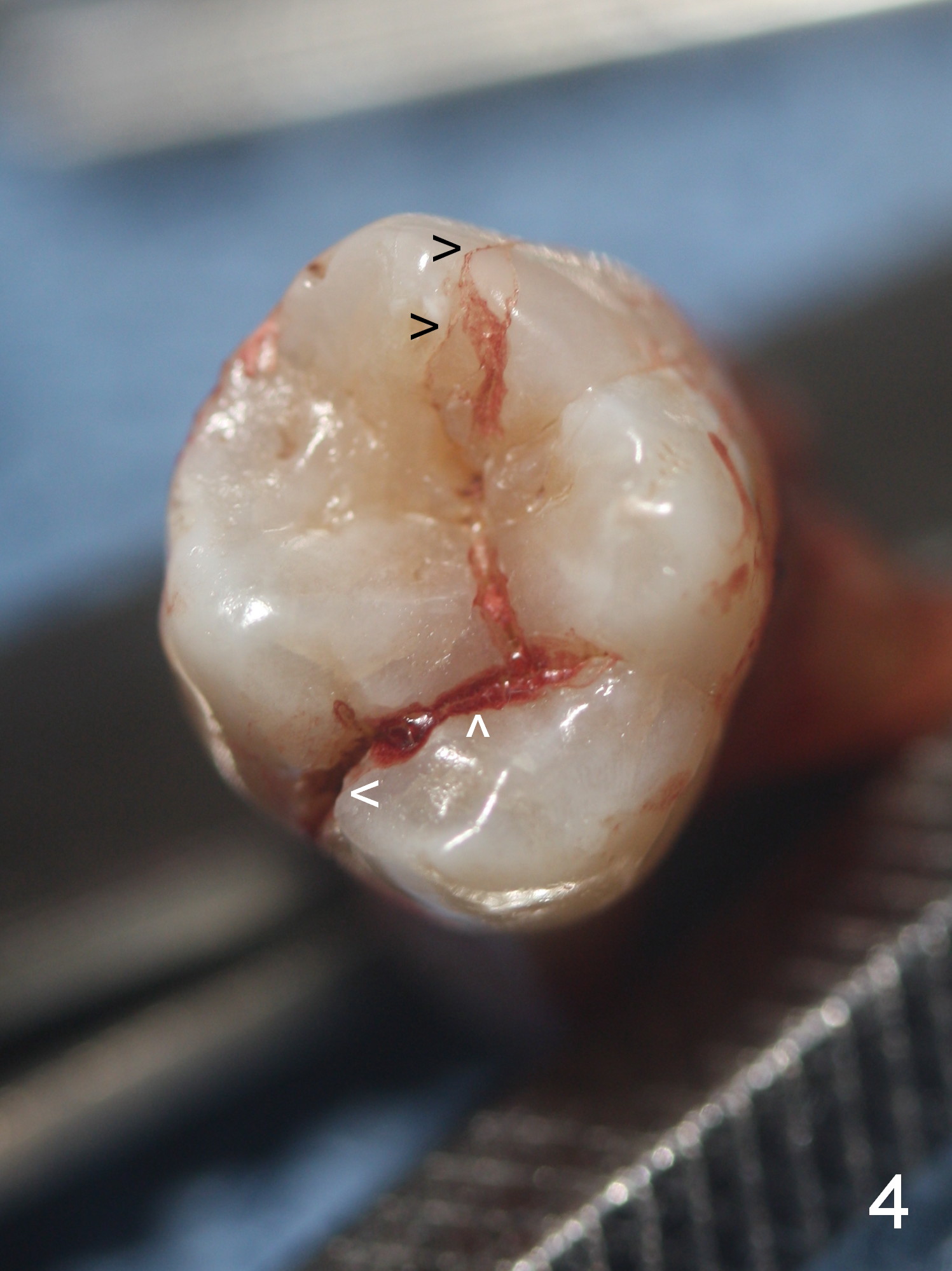
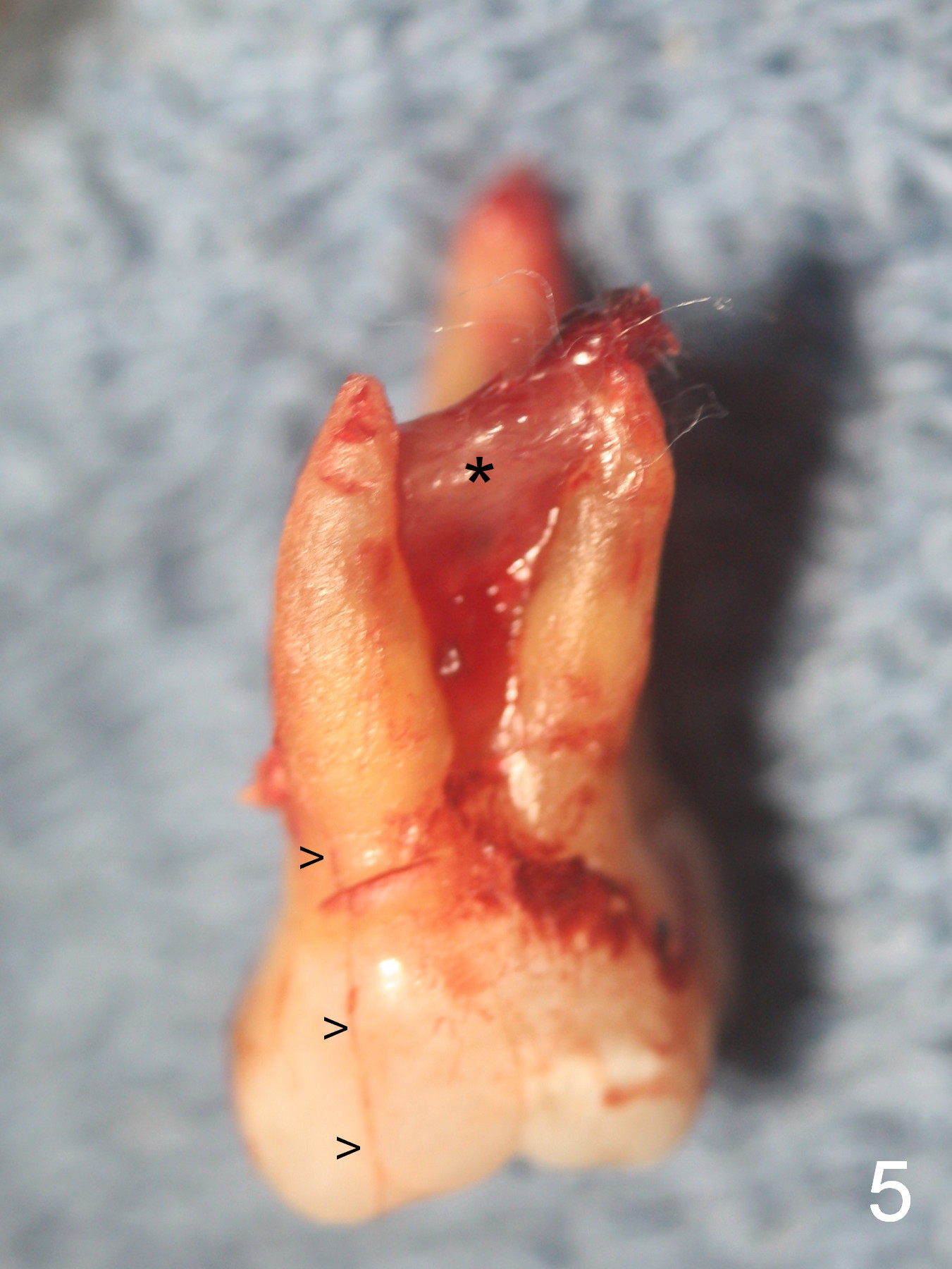
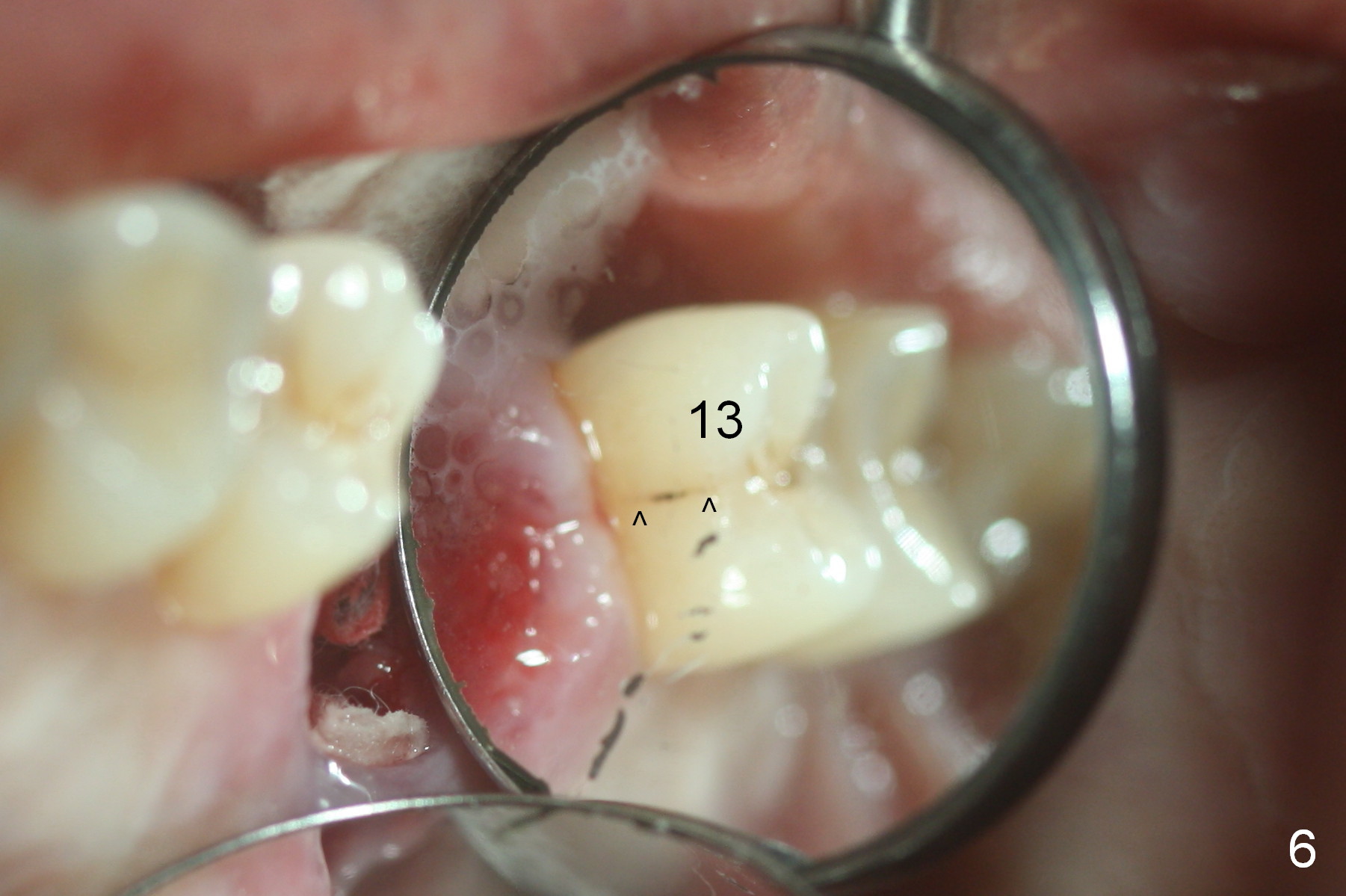
When the tooth is extracted, the lingual crack line (Fig.4 white <) is contiguous with the mesiobuccal one (black >). The latter corresponds to the white arrowheads in Fig.2. In all the crack line is extensive. The buccal and palatal plates are defective coronally. The large granulation tissue in the furca (Fig.5 *) suggests bone loss in the crestal septum. Most surprising is a crack line in the distal surface of the tooth #13 (Fig.6 ^) and in the mesial surface of #15 (Fig.7). Night guard will be fabricated after an implant crown is cemented at #14.
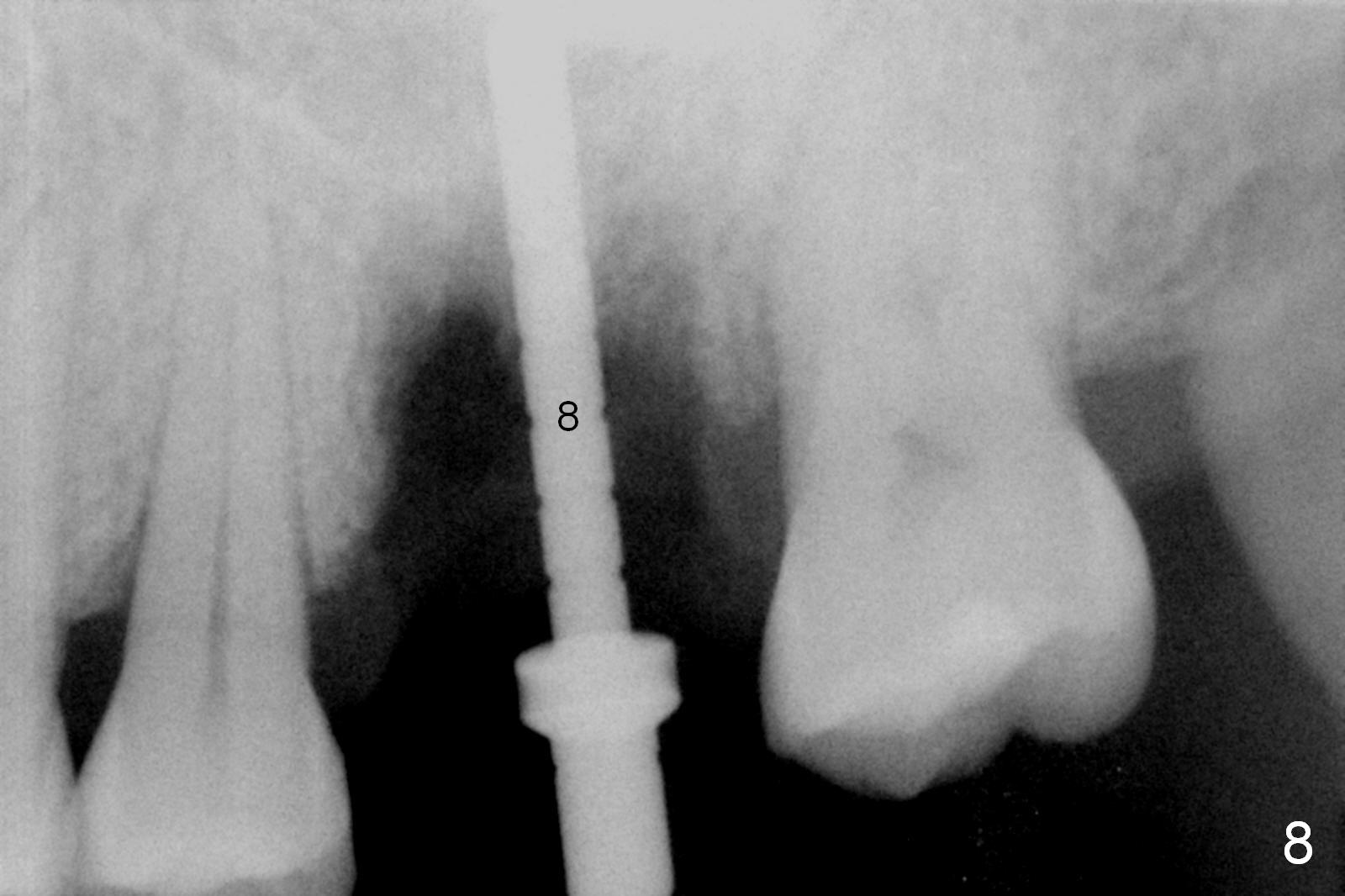
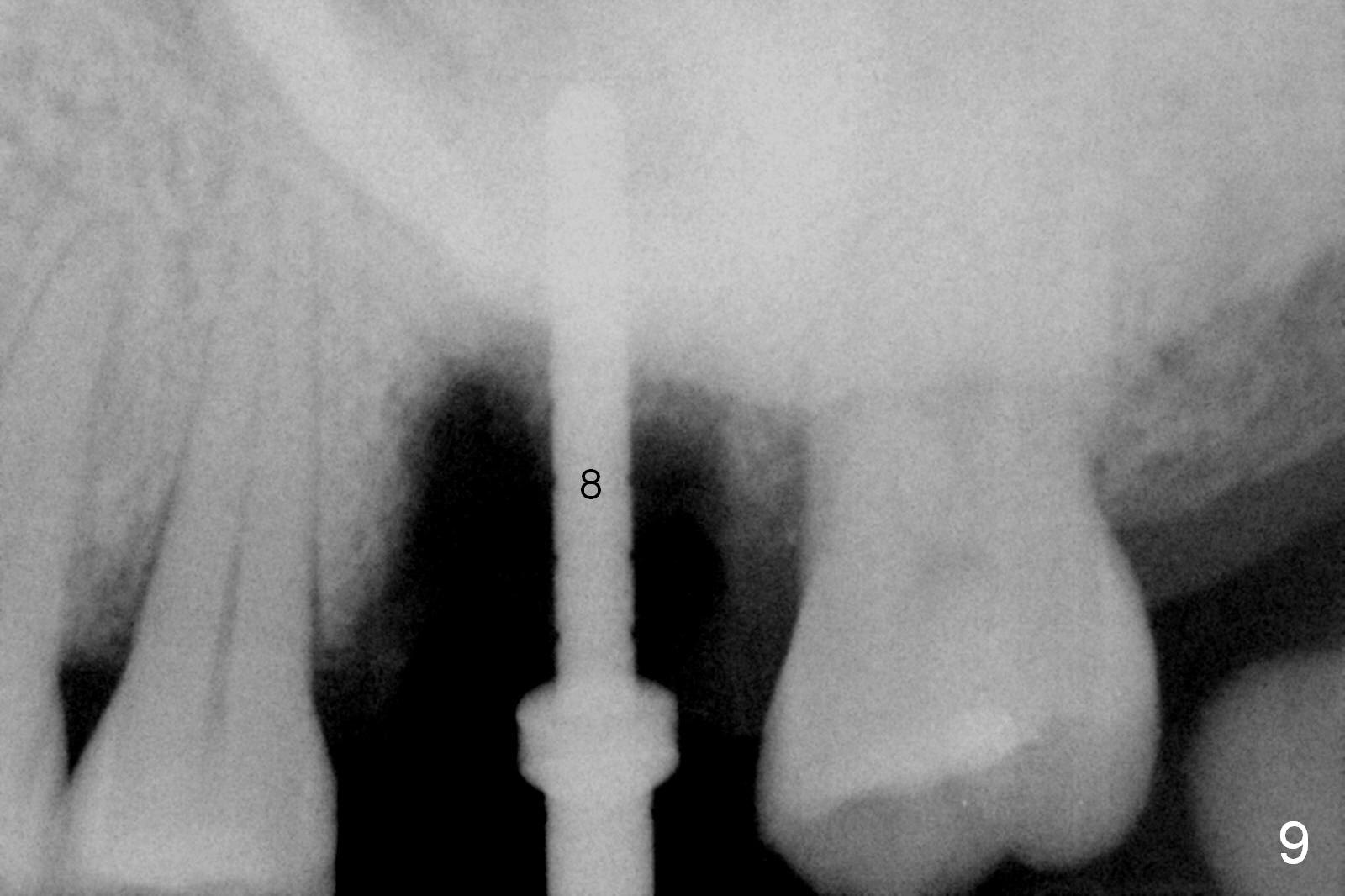
Osteotomy is initiated in the palatal slope of the septum 8 mm deep (Fig.8,9). A 5x11.5 mm implant is placed with insertion torque of 35 Ncm with ~ 2 mm sticking into the sinus with bone graft and 1.5-2.5 mm outside the septum. The latter is covered by bone graft (Fig.10 *). There is no nasal hemorrhage postop.
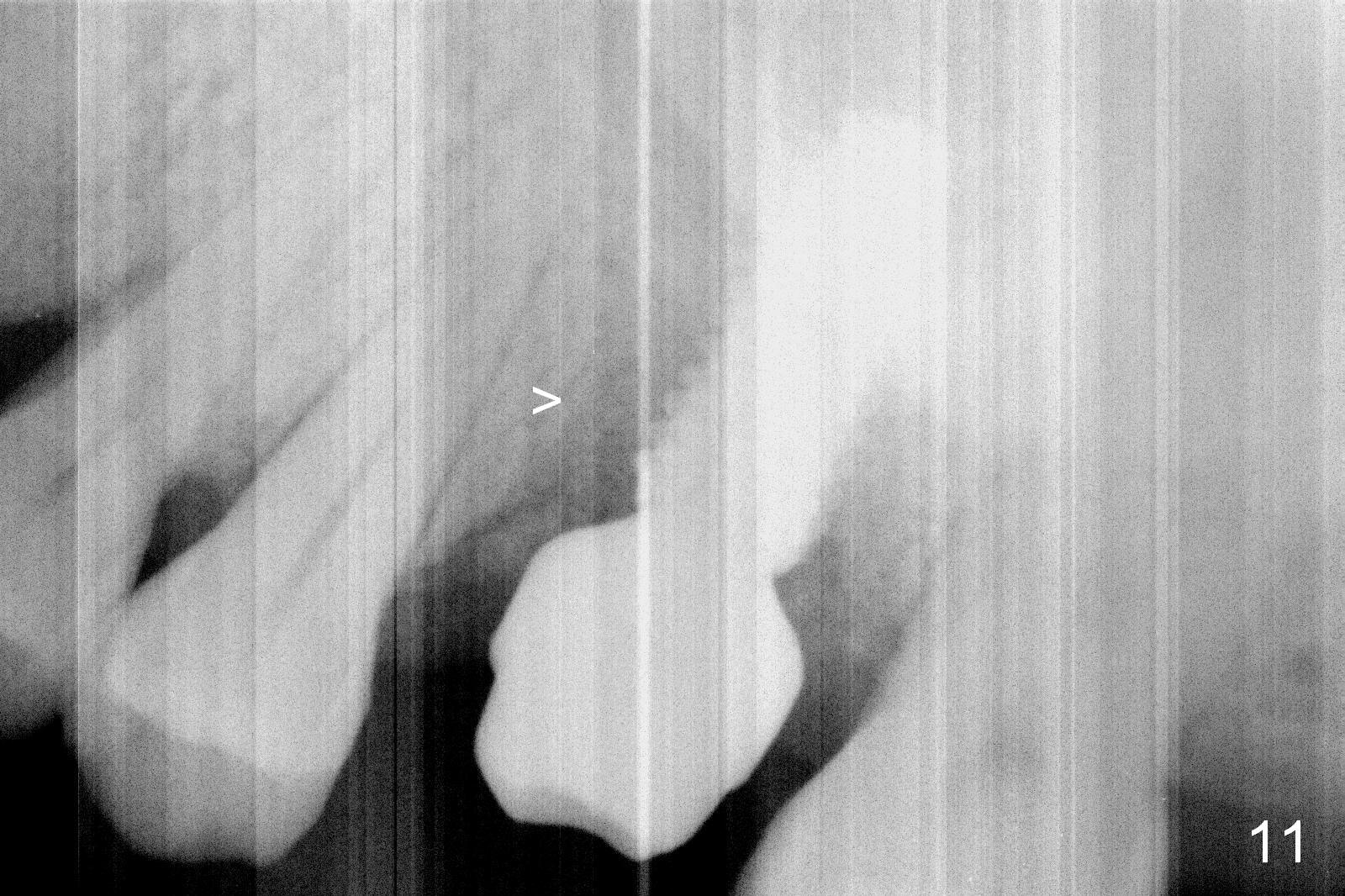
Oral hygiene is excellent postop. The socket heals around the abutment. Four months postop, the native bone appears to be approaching the implant surface (Fig.11 >).
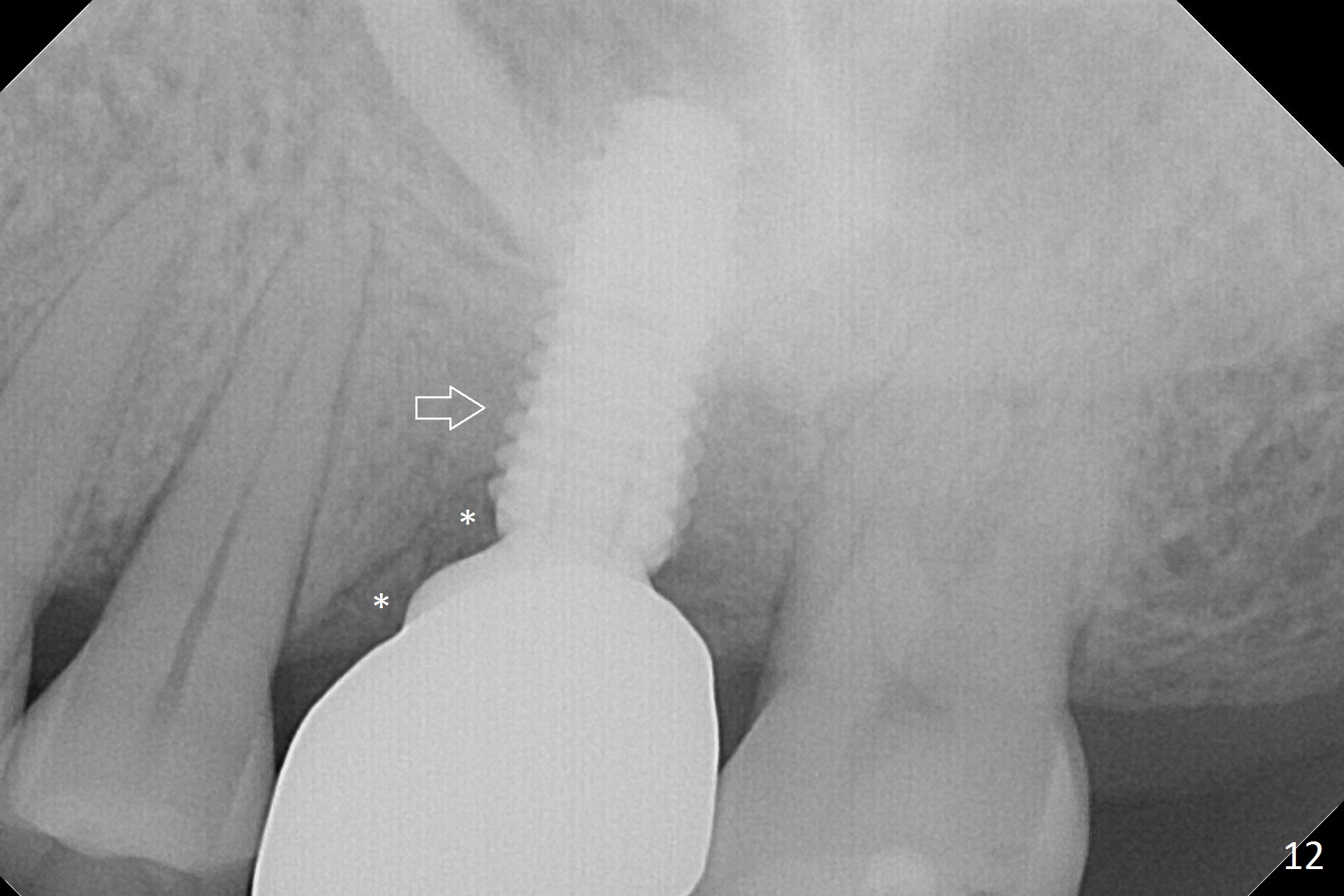
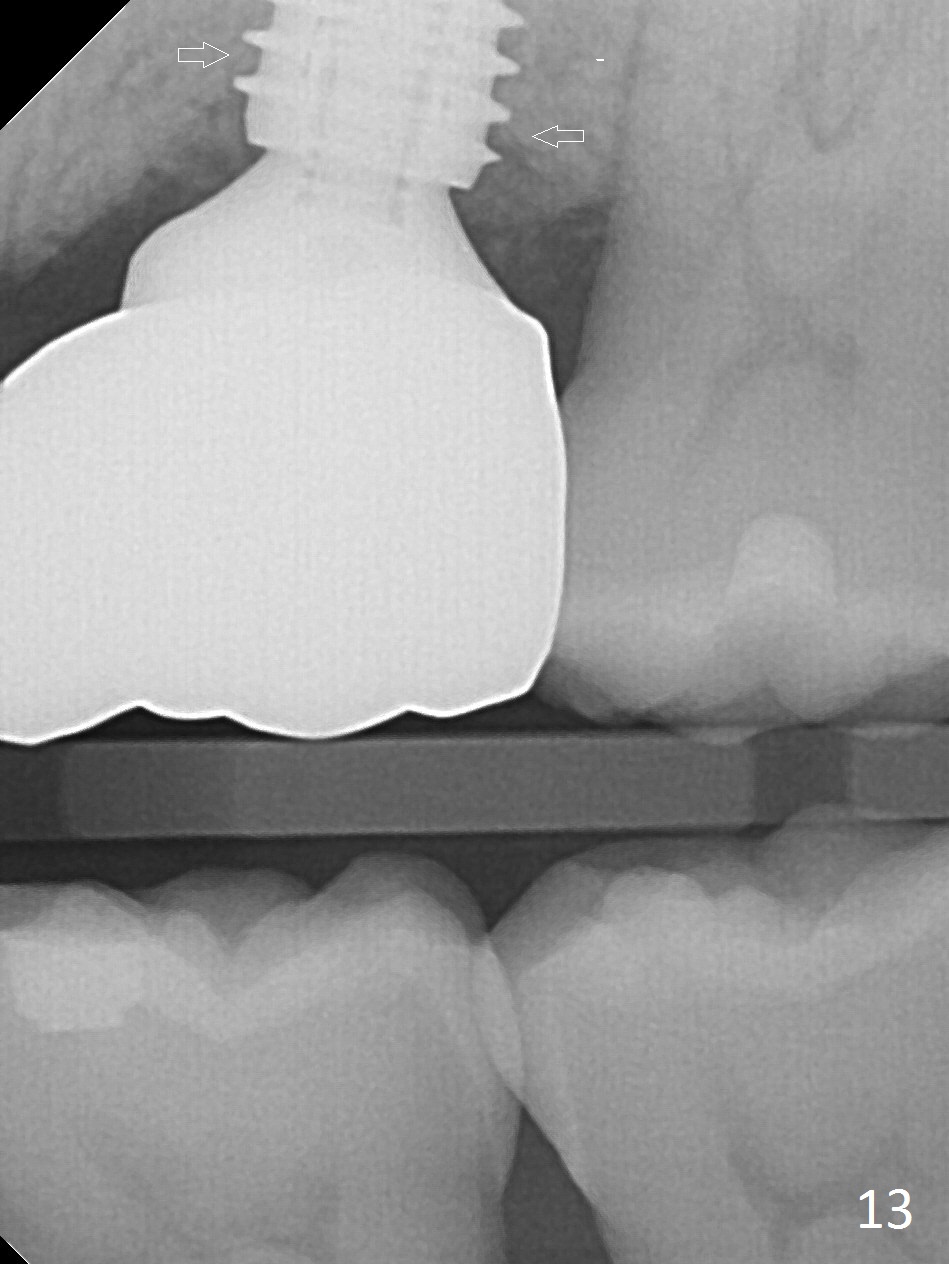
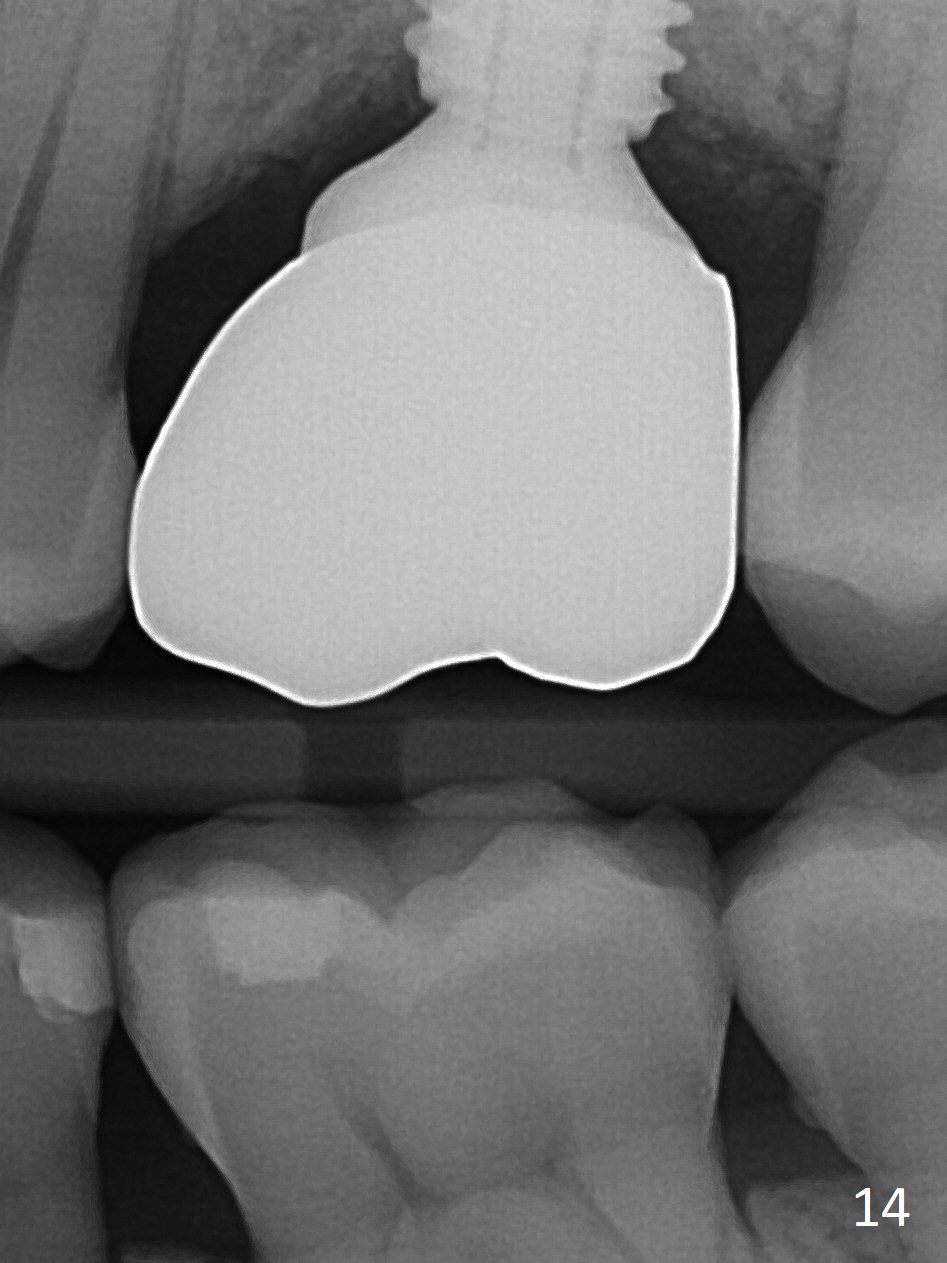
The patient experiences palatal gingival tenderness 5 months post cementation, probably due to loose proximal contacts and excessive use of floss. PA shows new normal bone next to the upper threads (Fig.12 arrow), while new less dense attached to the most coronal threads (*). BWs (Fig.13,14) shows that new bone has grown into the area between the most coronal 2 threads (arrows). When the crown and abutment are removed, the gingiva looks normal except minor laceration buccally. A 7.5x4 mm healing abutment is placed. If the infection resolves, pick up impression will be taken to add porcelain to the proximal surfaces to prevent food impaction.
Return to
Upper Molar Immediate Implant,
Prevent Molar Periimplantitis (Protocols,
Table)
Xin Wei, DDS, PhD, MS 1st edition 07/11/2016, last revision 05/10/2017