.jpg)
,6x9,%206.5x5.7(3),%20Vanilla.jpg)
.jpg)
.jpg)
|
|
|
|
|
|
|
|
|
Difficult Control of Depth in Upper Molar Extraction Site I
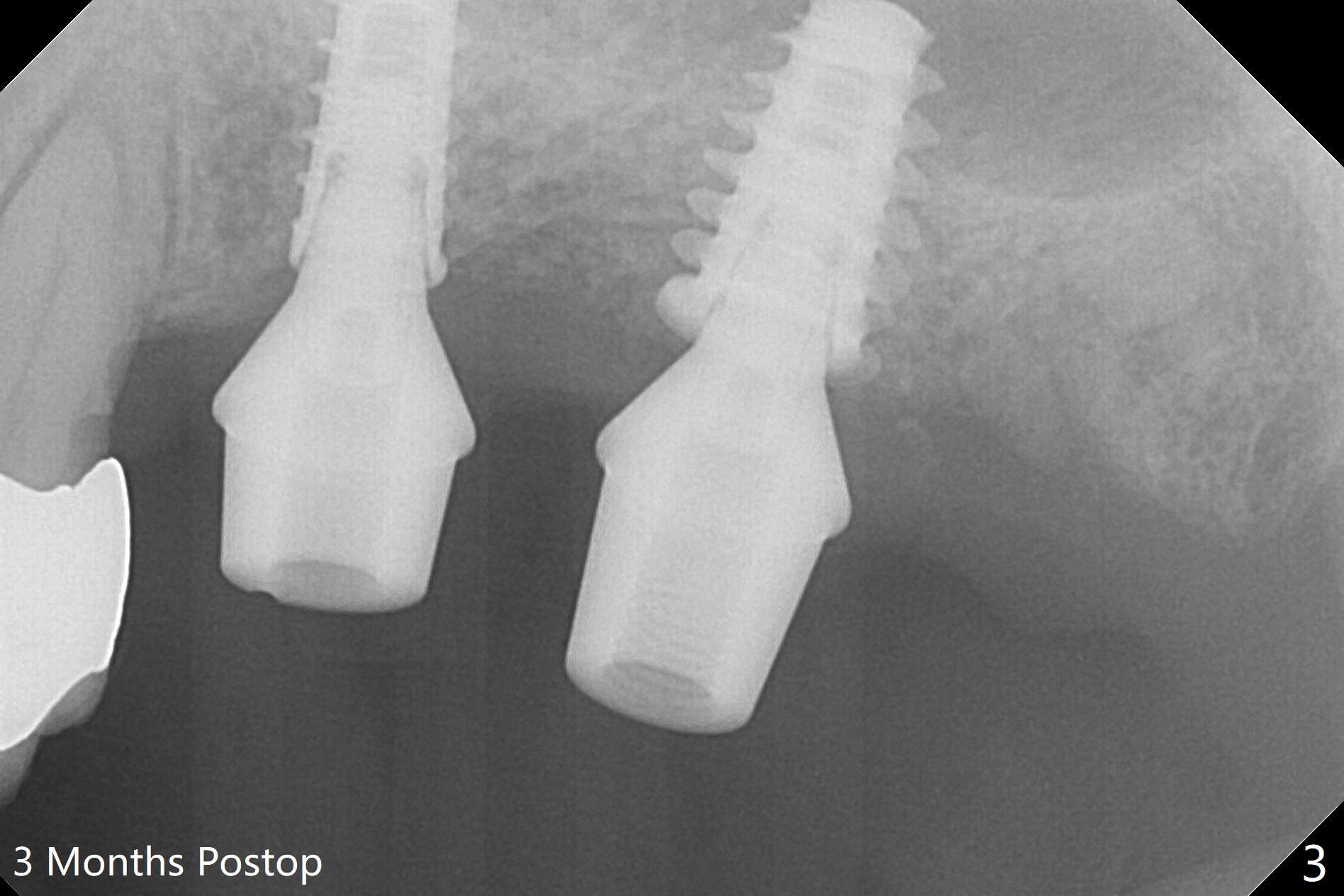
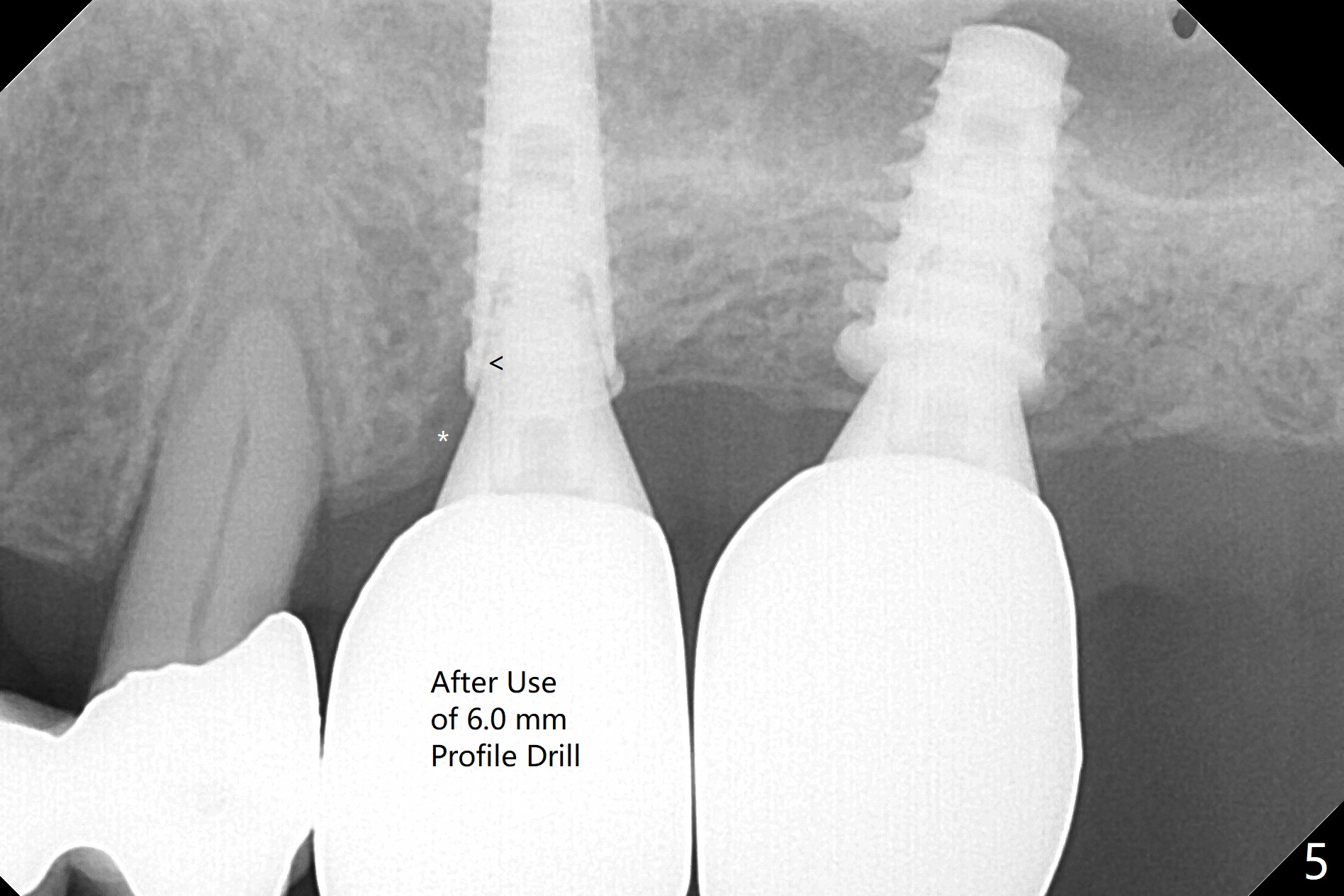
Due to irregular shape of freshly extracted socket at #15, control of depth is difficult. The sinus membrane is perforated after use of bone spreader, probably associated with drills longer than expected. SM taps (5.0 and 5.3 mm) do not achieve stability. When a 5.5x9 mm IBS dummy implant is inserted at #15, initial stability is obtained (Fig.1). Osteotomy at the edentulous area of #14 is uneventful with insertion of a 4x11 mm dummy implant (without involving the sinus floor apparently clinically as well, Fig.1). After adjustment of trajectory, a 4x11 mm definitive implant is placed at #14 with ~ 35 Ncm, while a 6x9 mm implant is placed at #15 with ~35 Ncm (Fig.2 (*: Vanilla Graft with Osteogen)). Periodontal dressing is applied around the abutments and neighboring teeth. There is mild oral and nasal hemorrhage postop. In fact the patient has history of coronary artery stent with oral Plavix intake. The medicine stops 4 days preop and is advised to resume after hemostasis is achieved. The patient returns 3 months postop (Fig.3). After changing abutments to 5.5x5.7(3) mm, impression is taken. The crown/abutment at #14 is loose 1 year 10 months post cementation. After use of 5.5 mm profile drill, the crown/abutment is reseated, but the seating is incomplete (Fig.4 <) because of contact of the abutment with the mesial crest (*). A larger profile drill does not help (Fig.5). When a narrower abutment (4.5x7.5(3) mm) is torqued, it appears to be completely seated (Fig.6). After distal surface adjustment of the abutment, impression is re-taken. There are 3 other unfavorable conditions: poor crown/implant ratio and trajectory and #18 missing.
Return to Upper Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), Armaments No Deviation
Xin Wei, DDS, PhD, MS 1st edition 11/28/2017, last revision 01/14/2020