.jpg)



|
|
|
||
|
|
|
|
|
|
|
|
|
|
Sinus Perforation
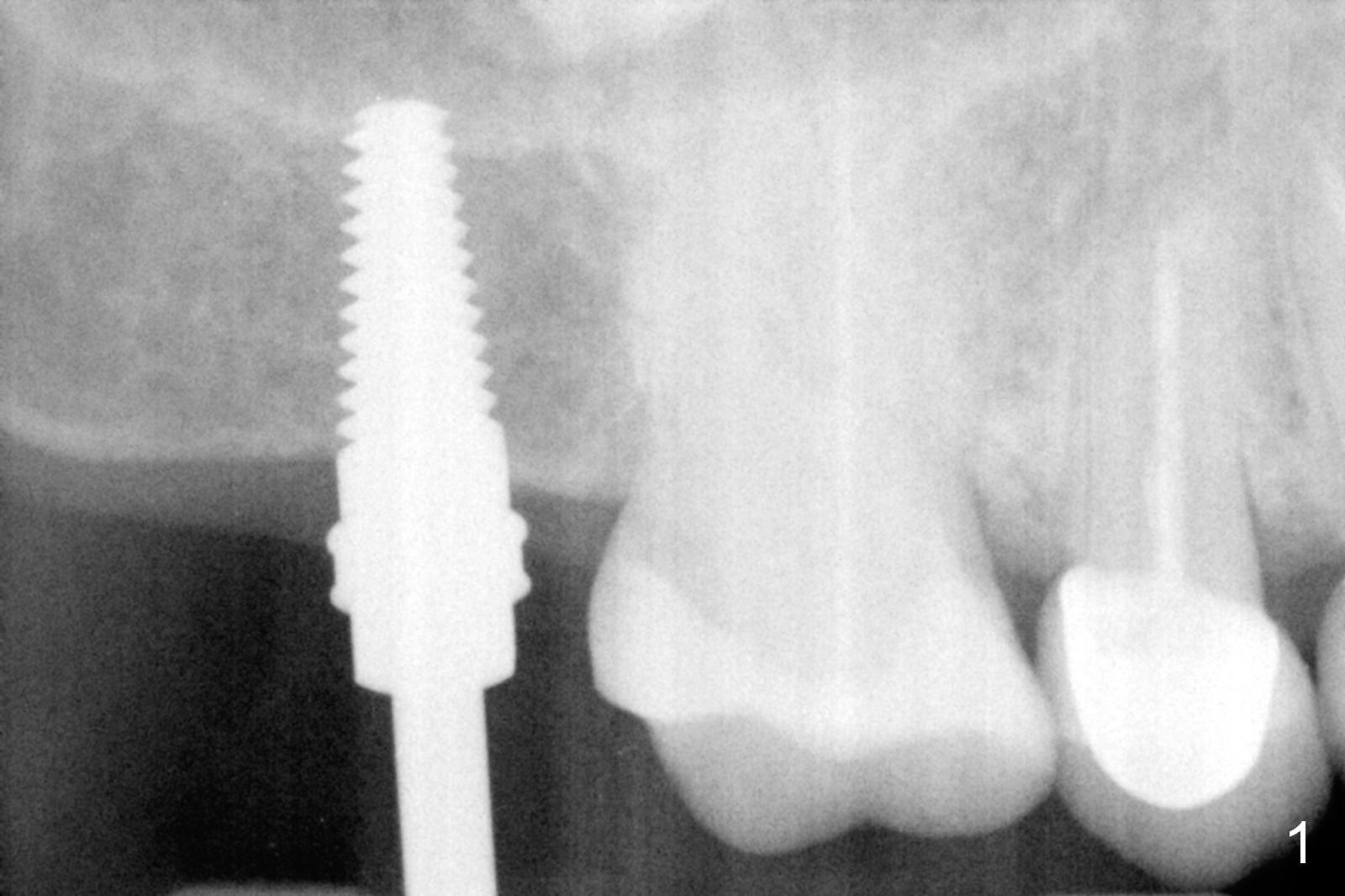
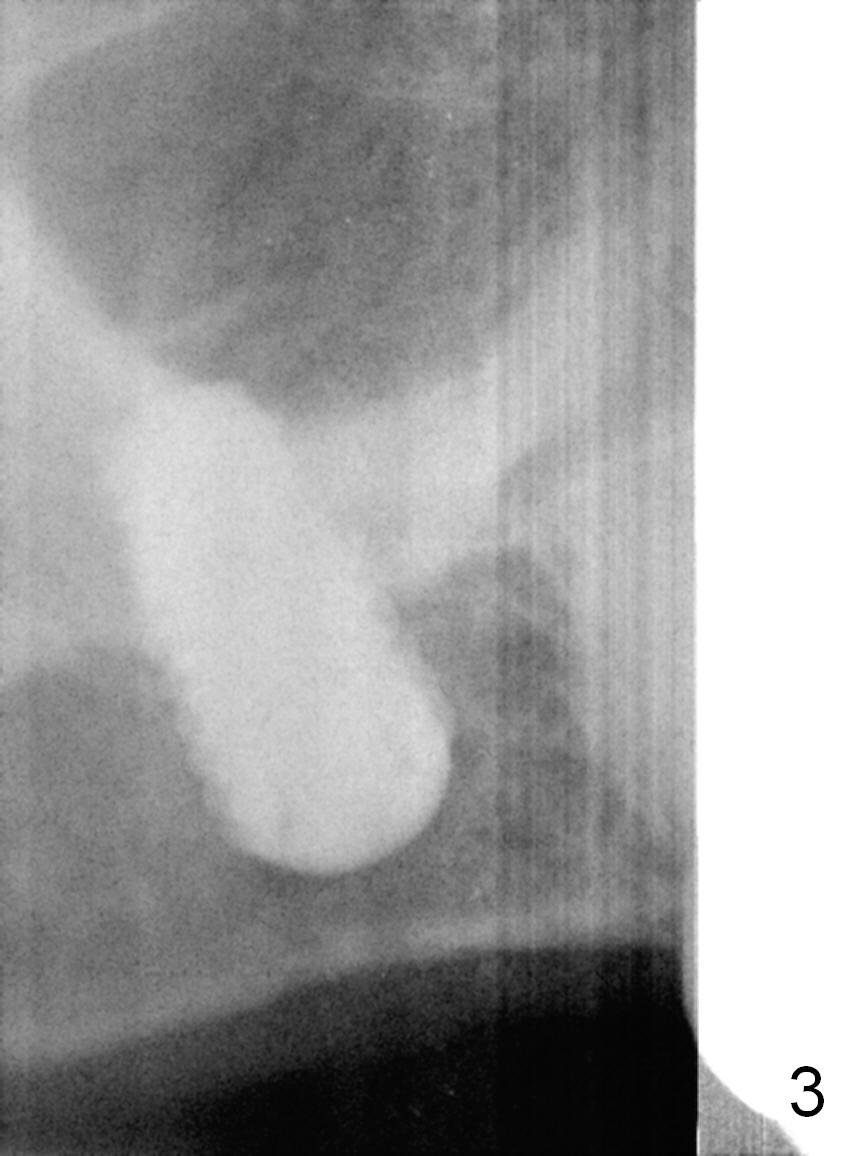
#15 blade is used for incision and initial bone expansion and condensation, followed by bone scalpels, bone blades and round tapered osteotomes (RT) 2-4. The sinus floor is barely penetrated by 4.5x11 mm Tatum tapered tap (Fig.1). After using 5x11 mm tap, sinus lift is accomplished with allograft. A 5.5x10 mm UF implant is placed with a latch driver with insertion torque > 65 Ncm. Wrench does not seat the implant as deep as expected. It appears that the implant does not go through the sinus floor. The implant is removed, followed by tapping RT 2-4 deeper. When 4.5x11 mm tap is being reused, the sinus membrane is perforated. Osteogen plug is inserted, followed by the implant, which is placed deeper than expected with low stability (Fig.2). Placement of a cemented abutment appears to turn the implant as well. The abutment is removed and a healing screw is placed (Fig.3). The access is closed with Collagen plug. There seems to be sinus discharge into the pharynx postop with tenderness on the nasal bridge. The patient is scheduled to return 15 days postop to have the implant removed.
An incision will be made for better vision. Manual driver is used to avoid pushing the loose implant into the sinus. The osteotomy is filled with Osteogen plug, which is sutured in place. If the condition turns out to be excellent, place 6 mm UF tap prior to 6x6 or 8 mm implant.
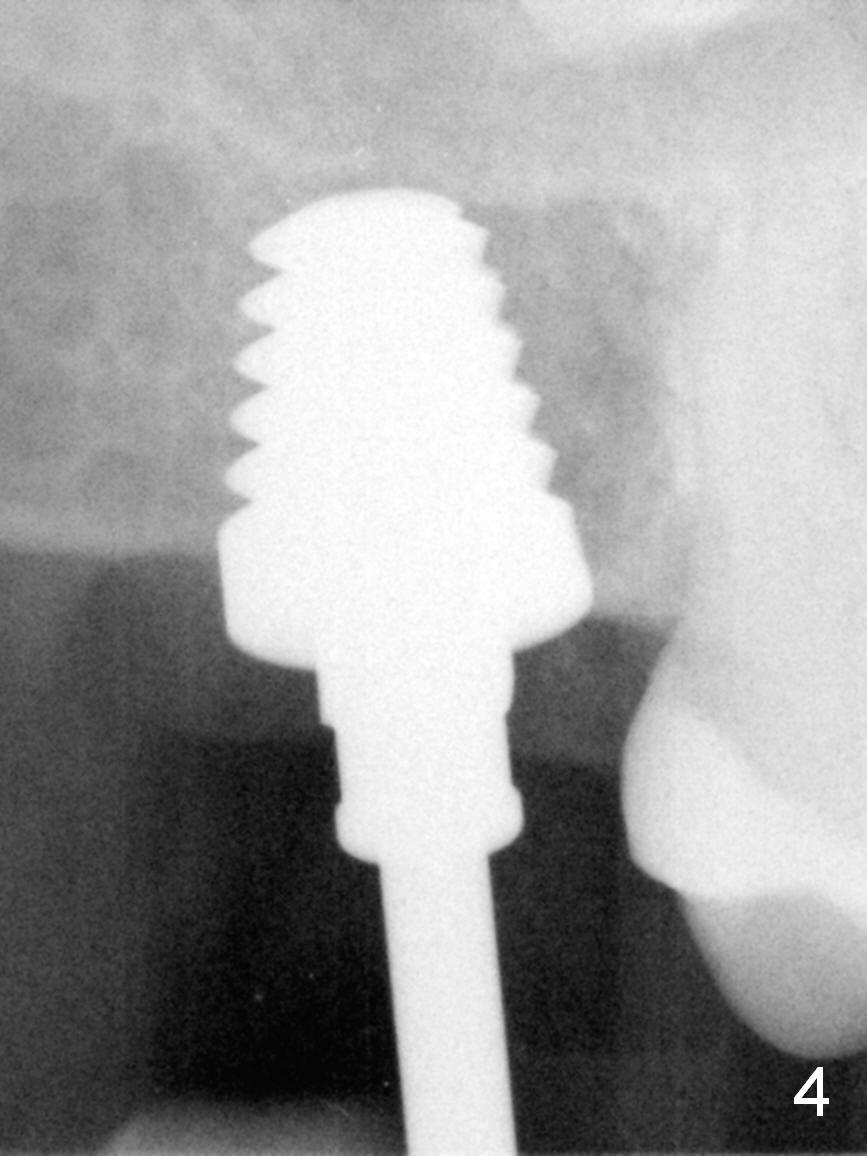
The patient returns 23 days postop. After incision, a latch driver has to be used to remove the mobile implant due to limitation of the space and difficulty in holding a hand instrument. There is no sinus perforation. The granulation tissue is removed from the wall of the osteotomy. Metronidazole is used for disinfection. UF taps (6, 6.5 and 7 mm) turn out to be small. Stability is achieved with a 8x11 mm Tatum tapered tap (Fig.4), followed by a 8x11 mm implant with insertion torque of 60 Ncm (Fig.5). Sinus symptom disappears immediately postop and the wound heals 8 days postop. A healing cuff is placed with triple antibiotic ointment 2 months postop.
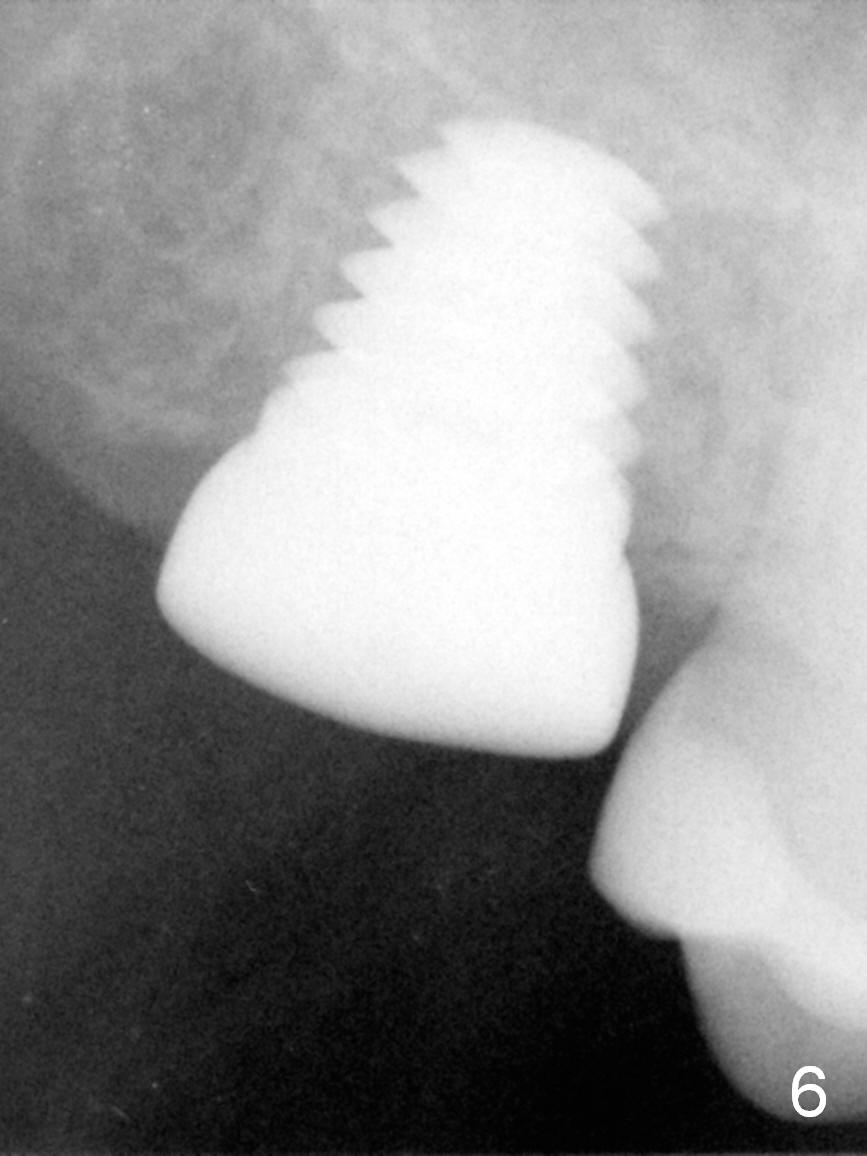
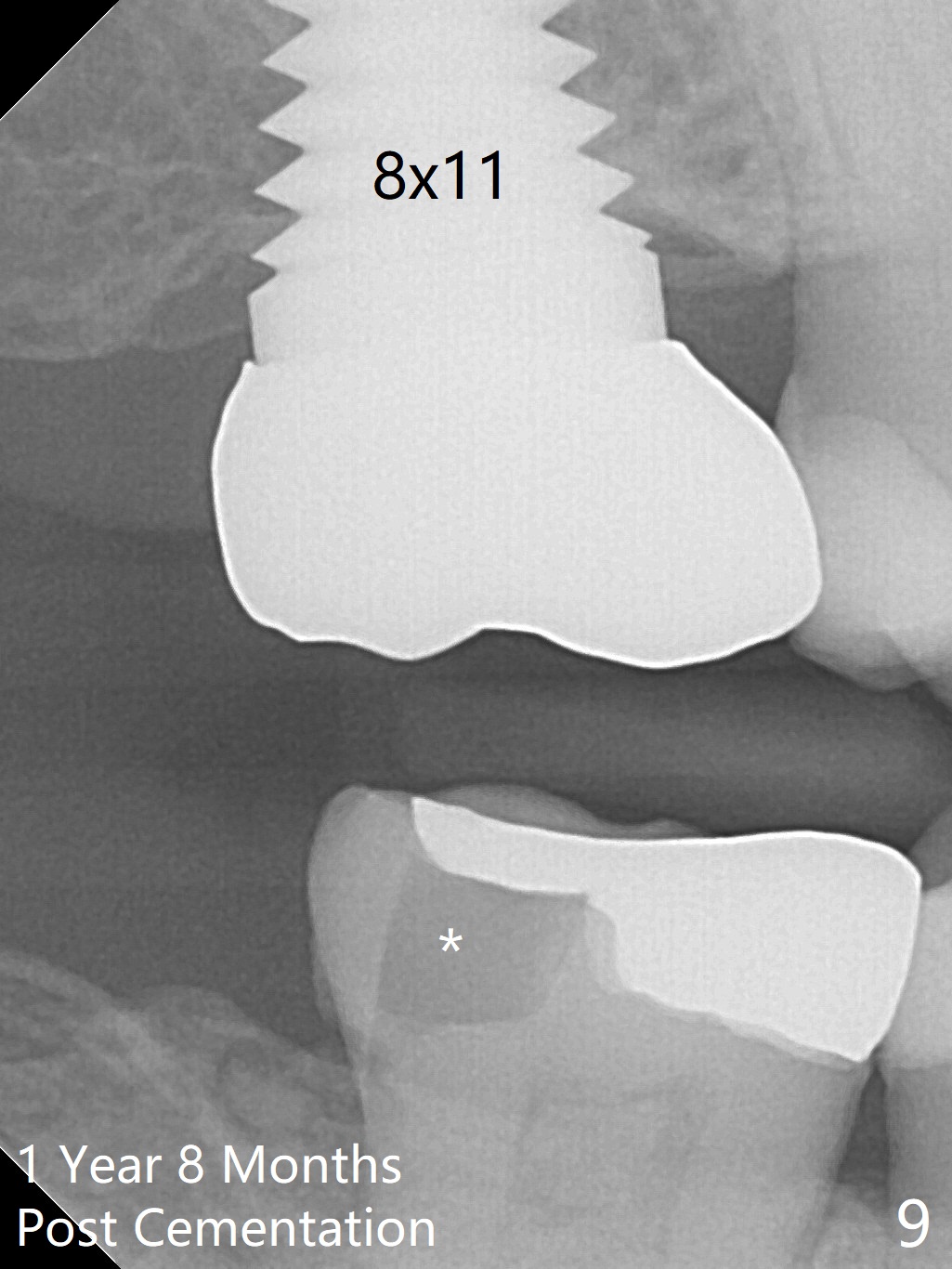
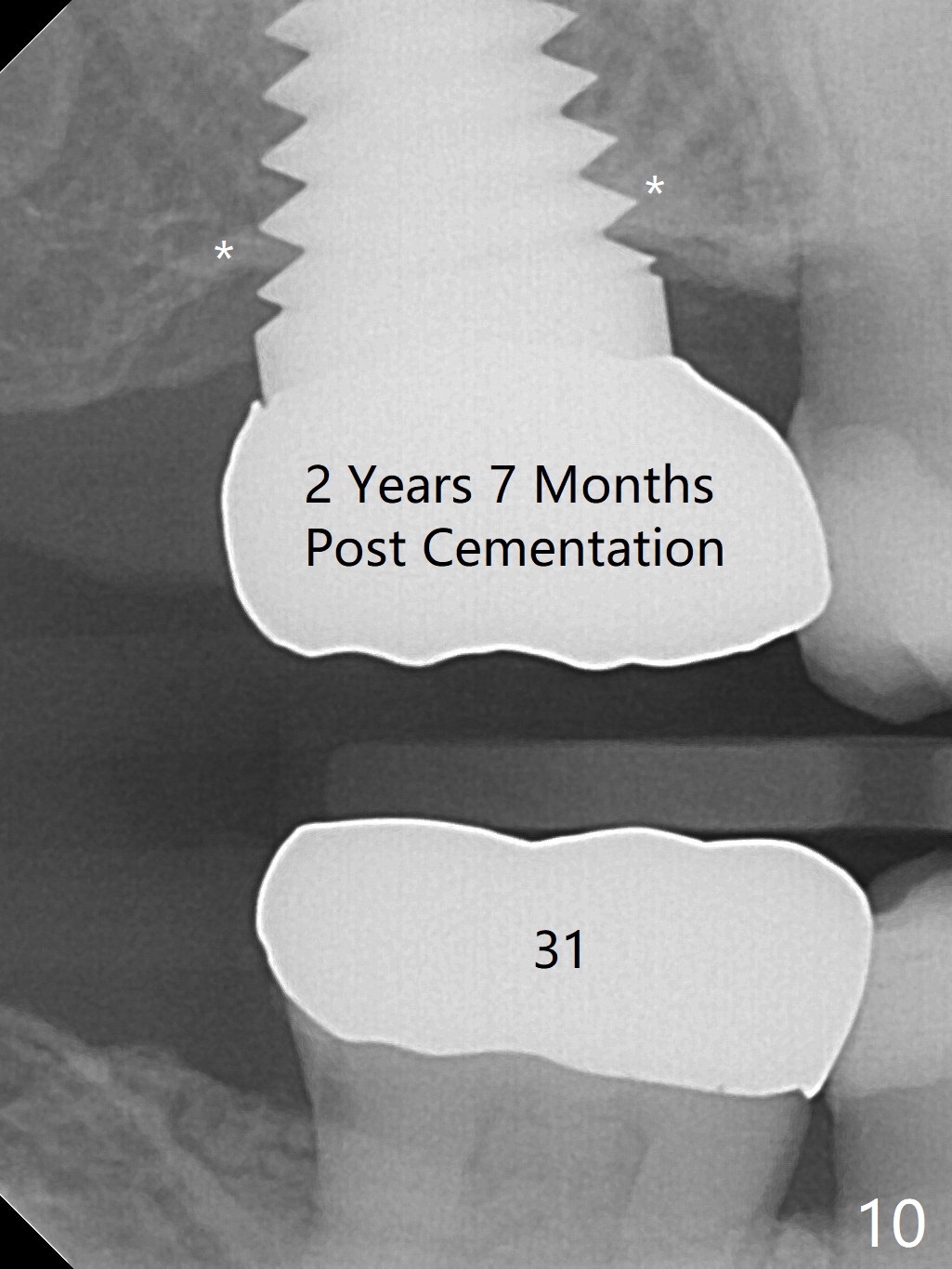
Next visit (10 days later, 2.5 months postop), the patient returns for final restoration. The implant appears to have osteointegrated (Fig.6). When a 6x3 mm abutment is placed (Fig.7), severity of the opposing tooth supraeruption is noticeable (Fig.8). Heavy reduction is conducted prior to impression. There is no bone loss 1 year 8 months post cementation (Fig.9). In fact the Zirconium onlay of the opposing tooth fractures (*). The bone density around the most coronal threads increases 2 years 7 months post cementation (Fig.10 *), while the high noble crown of the tooth #31 has been fabricated to prevent future crack (heavy mastication).
Return to
Upper Molar Immediate Implant,
IBS Improvement,
Training
Course
2 #8,
10,11
Xin Wei, DDS, PhD, MS 1st edition 07/02/2016, last revision 05/24/2019