


|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Immediate Implant for Fearful Patient
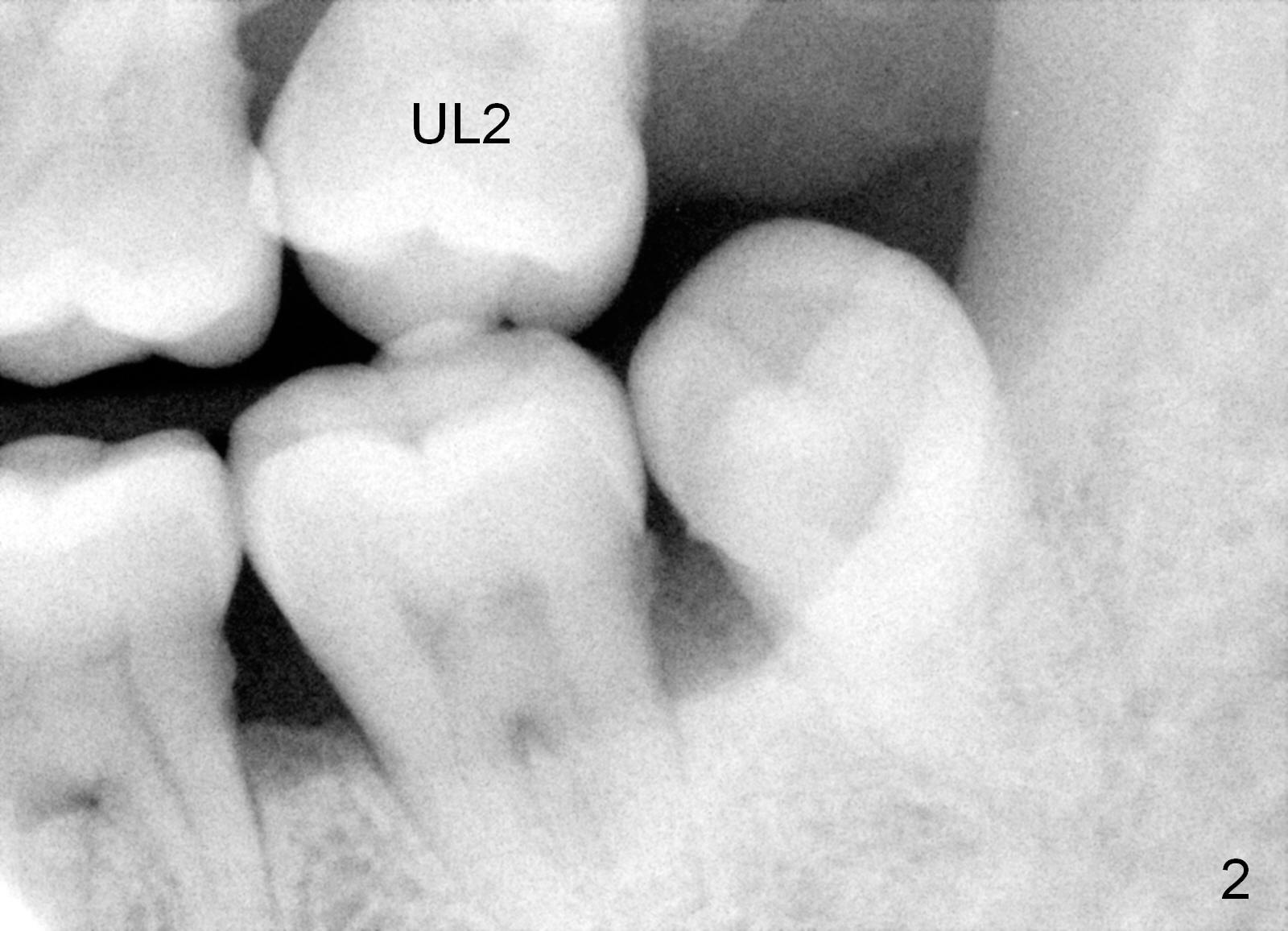
A 49-year-old lady is scared of dentistry. She presented with chronic periodontitis 7 years ago. The lower right 2nd molar had been missing (Fig.1 LR2), while the upper right 2nd molar shifted distally (arrow). Her chief complaint was mobility of #15 (Fig.2,4 UL2 with severe bone loss (*)). The tooth was extracted with expectation of return for implant placement in 6-8 weeks.
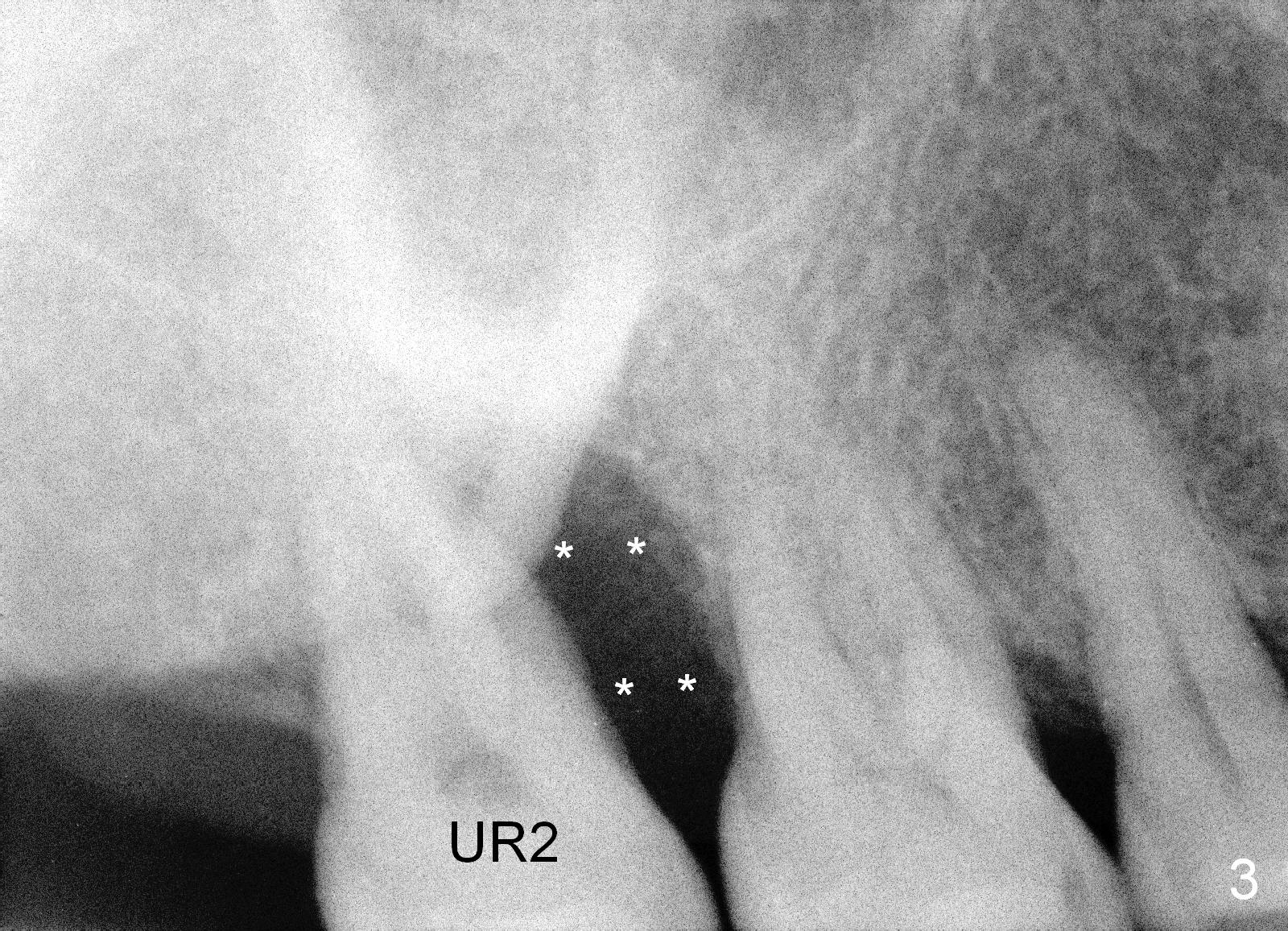
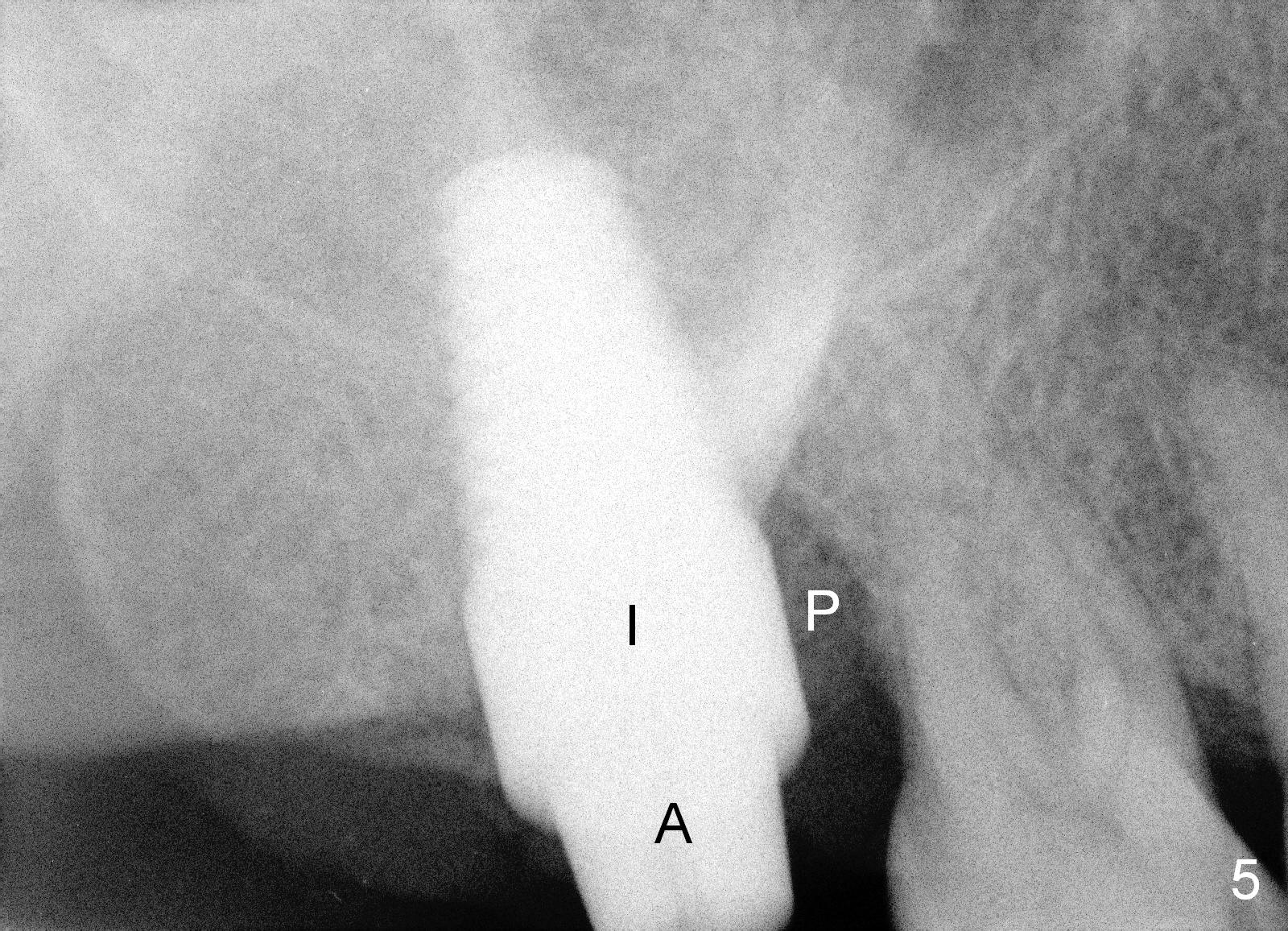
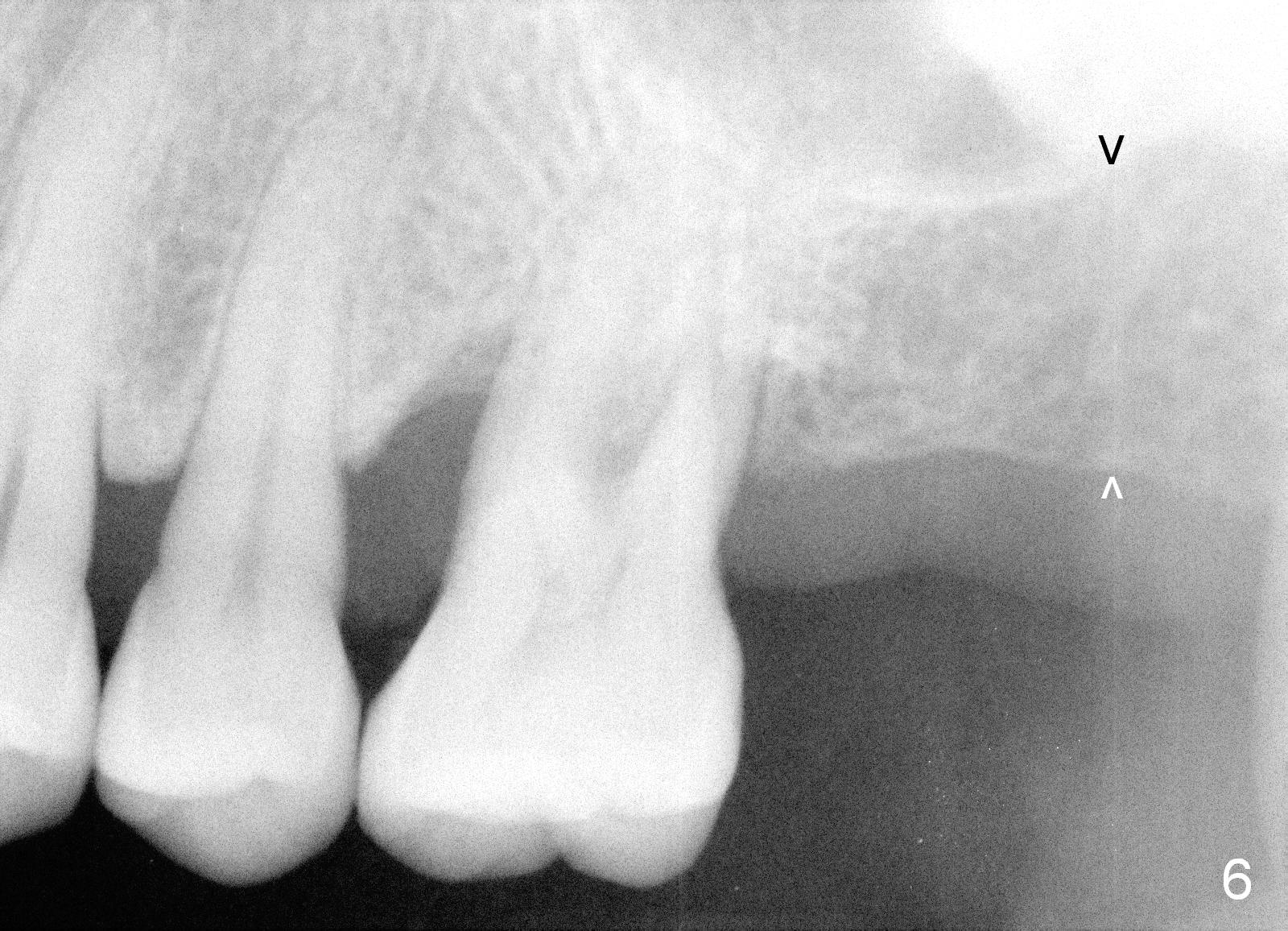
When she returns 7 years later, the tooth #2 has perio abscess with severe bone loss (Fig.3). She refuses to take antibiotic for infection control, but agrees to have immediate implant for #2 because of 1-staged surgery (Fig.5 I: 8x17 mm; A: abutment; P: bone powder (graft)). She is aware of delayed implants at the sites of #15 and 31 later. The bone height at the site of #15 reduces from 12 mm (Fig.4) to 7 mm (Fig.6) in 7 years.
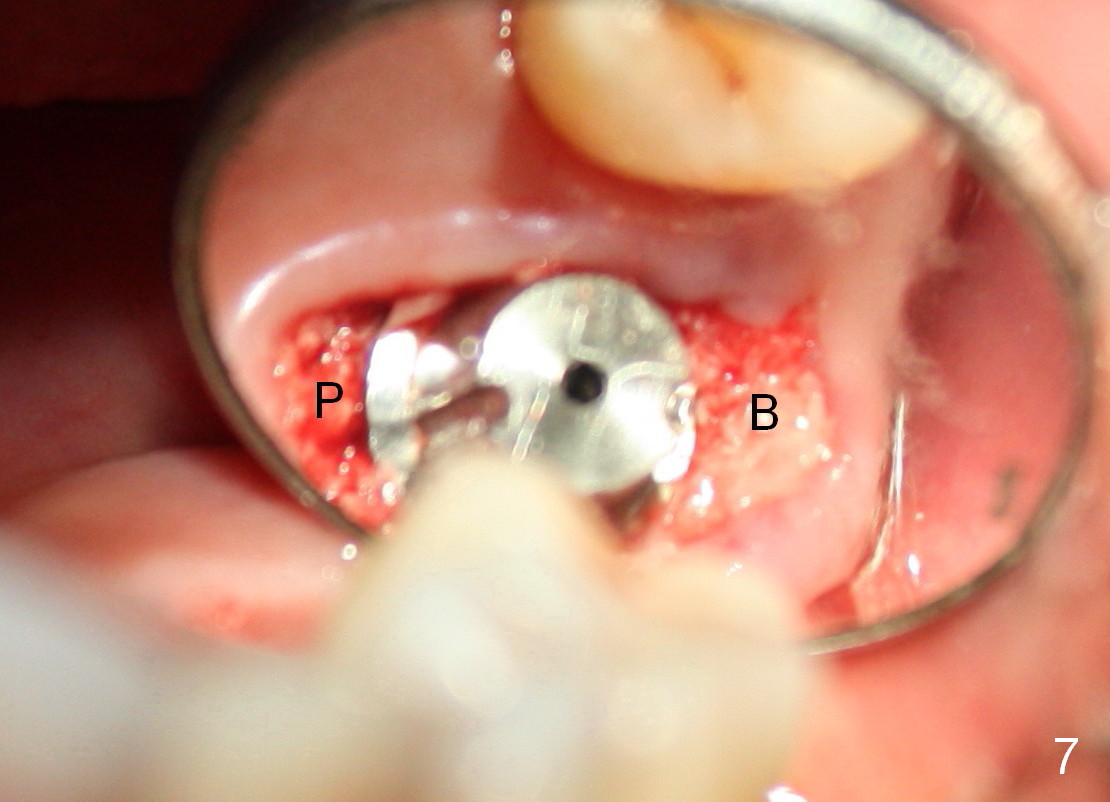
The large implant obliterates the socket mesiodistally (Fig.7); the buccal (B) and palatal (P) gaps are filled with bone graft, which is held in place by an immediate provisional.
The tissue-level implant is placed subgingivally (mesially); insertion torque is 15 Ncm. The same diameter cylindrical implant with larger surface area may achieve higher insertion torque with supragingival margin. The latter is easy for restoration.
When the patient returns 5 months postop (Fig.8), the immediate provisional is dislodged. The mesiolingual implant margin is subgingival. Under local anesthesia, gingivectomy is performed with Diodie Laser, followed by insertion of a healing abutment (cuff).
Return to Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 04/22/2015, last revision 09/25/2015