
|
|
|
|
|
|
|
|
Osteotomes or Taps Form Implant Site
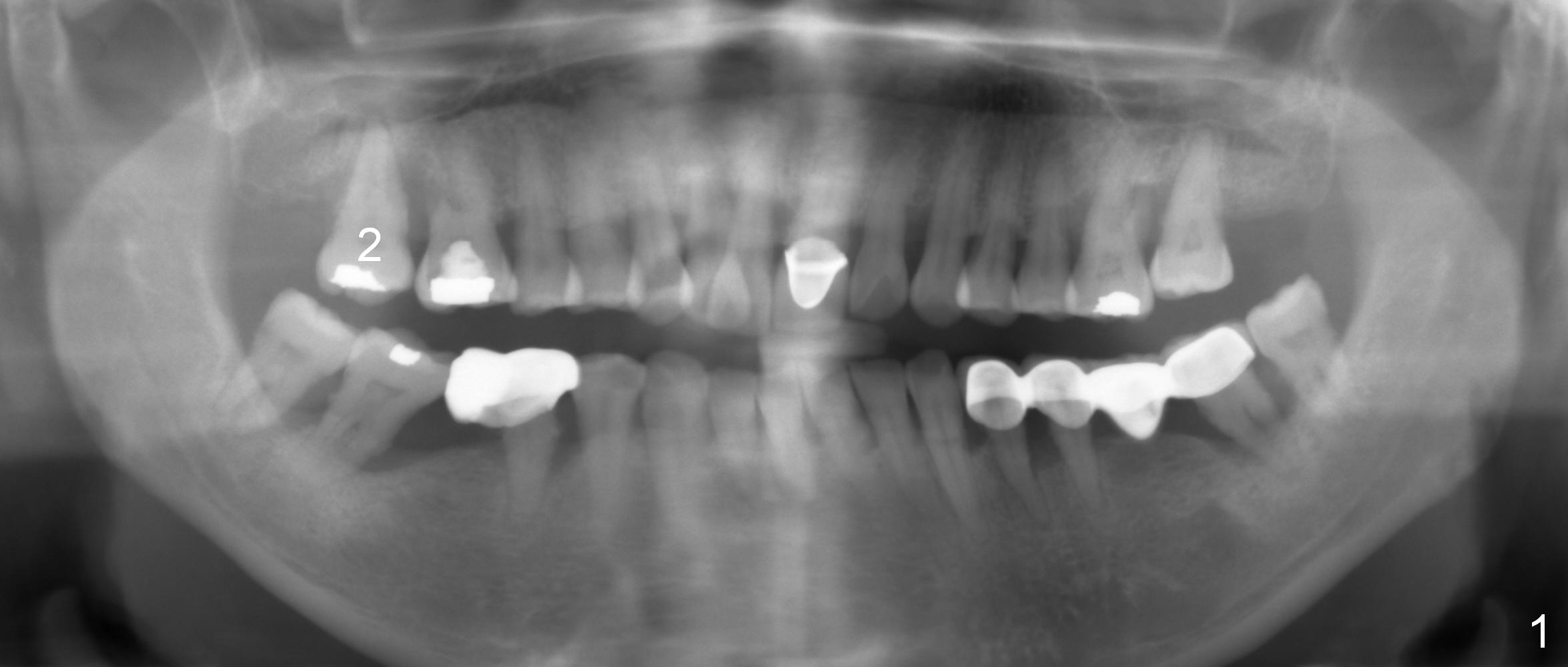
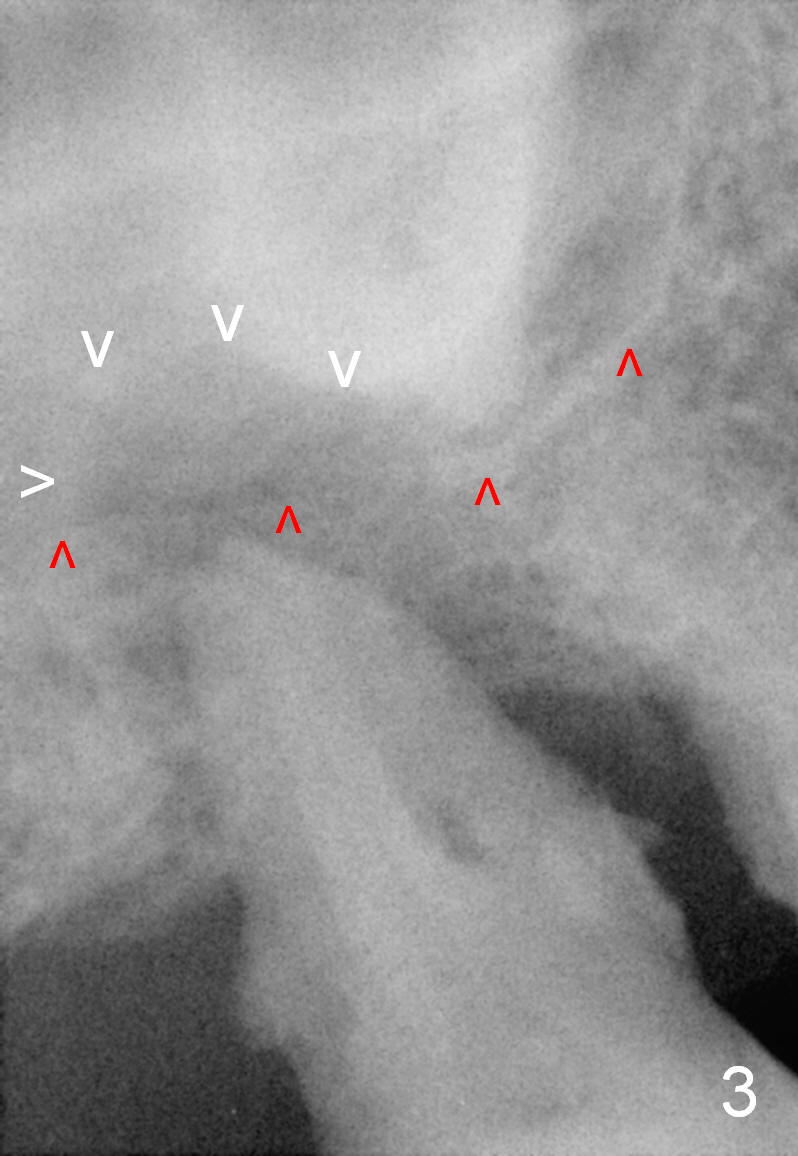
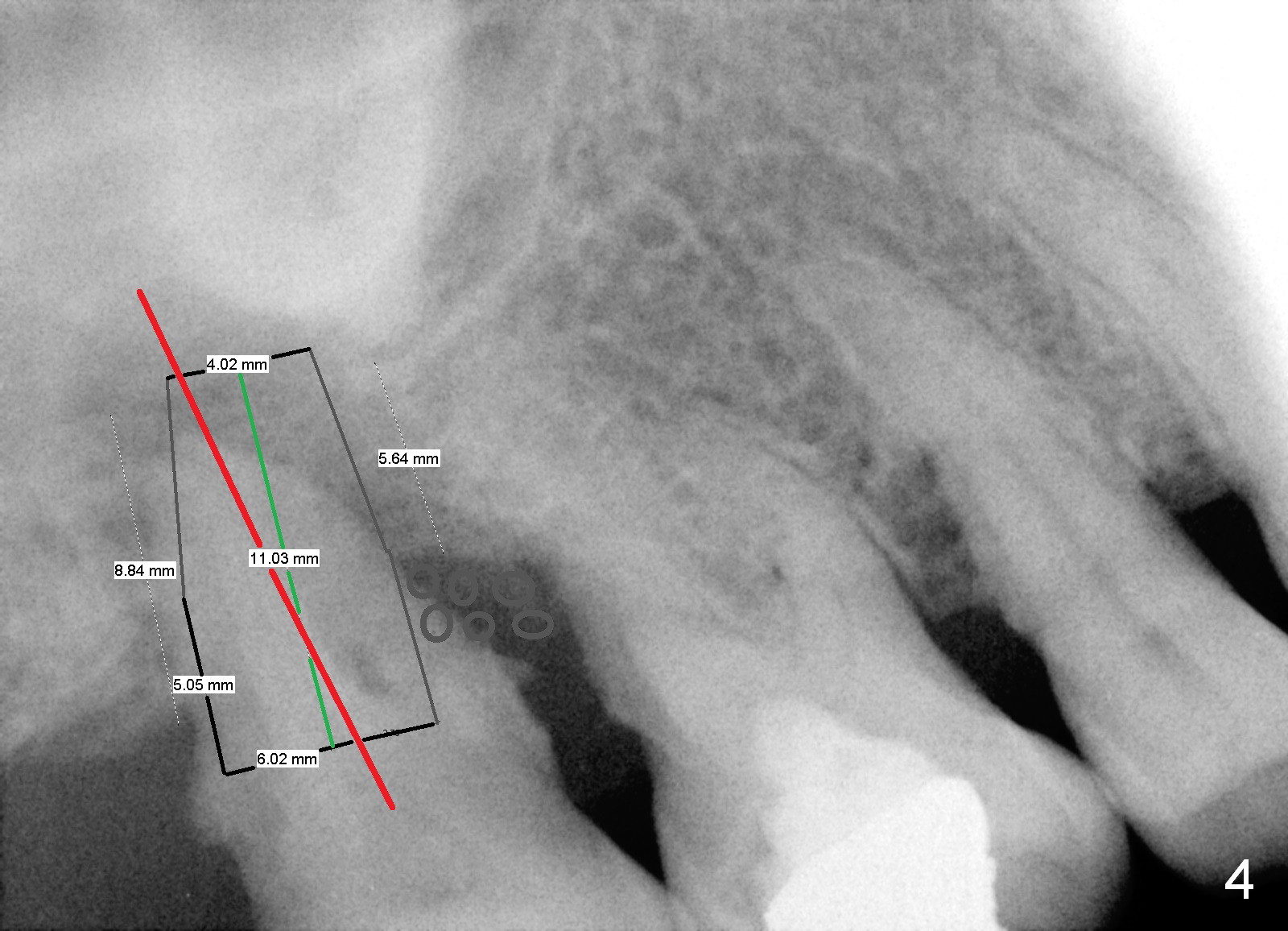
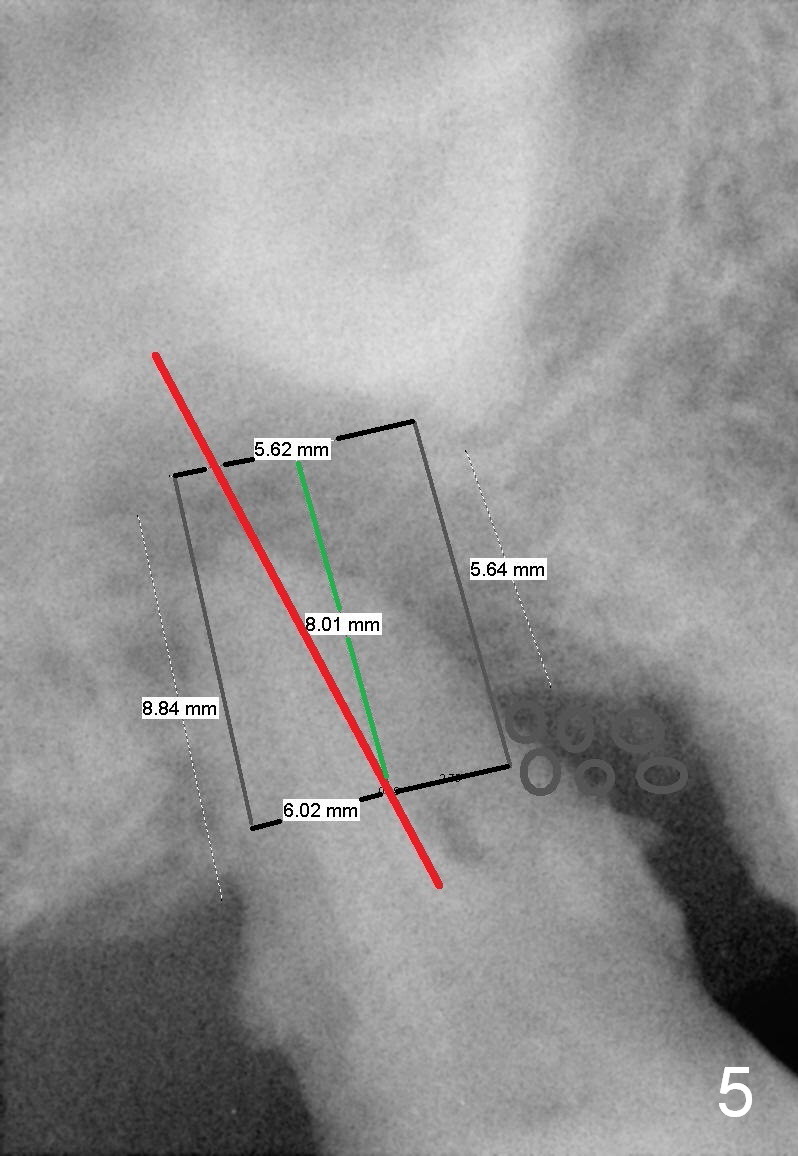
A 49-year-old lady (ZY, dental phobic) has had poor dentition (Fig.1). Finally the tooth #2 is non-salvageable with mobility and bone loss (Fig.2). The periapical radiolucency (Fig.3 white arrowheads) is higher than the sinus floor, suggesting presence of bone beyond the sinus floor. The designed tissue-level implant (Fig.4: 6x11 mm) could be longer e.g. 6x14 mm); bone-level implant could be as long as 12 mm (Fig.5).
After the socket is treated with Clindamycin, osteotomes or taps will be used form osteotomy. Attention should be paid to the long axis of the osteotomy, which should be parallel to those of the neighboring teeth (Fig.4,5 red line). In this way, the coronal end of the implant will be even with the mesial and distal crests. No excessive bone graft will be placed around the mesial crest (Fig.4,5: black circles). The long axis of the designed implant is represented by green line in Fig.4,5.
Return to Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 09/13/2015, last revision 12/27/2015