





|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Bone Density
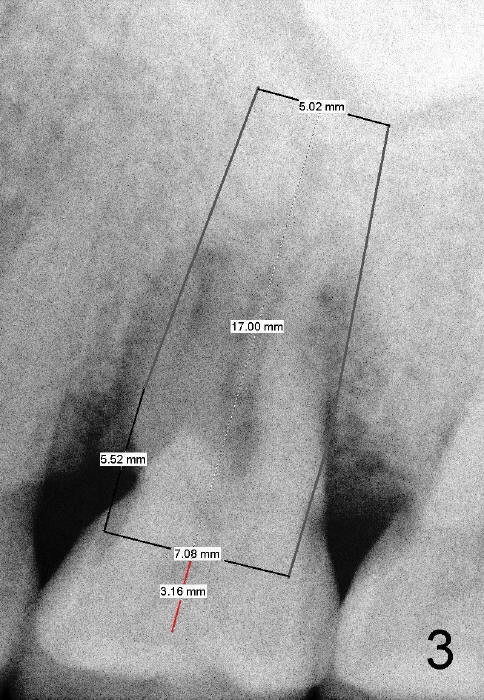
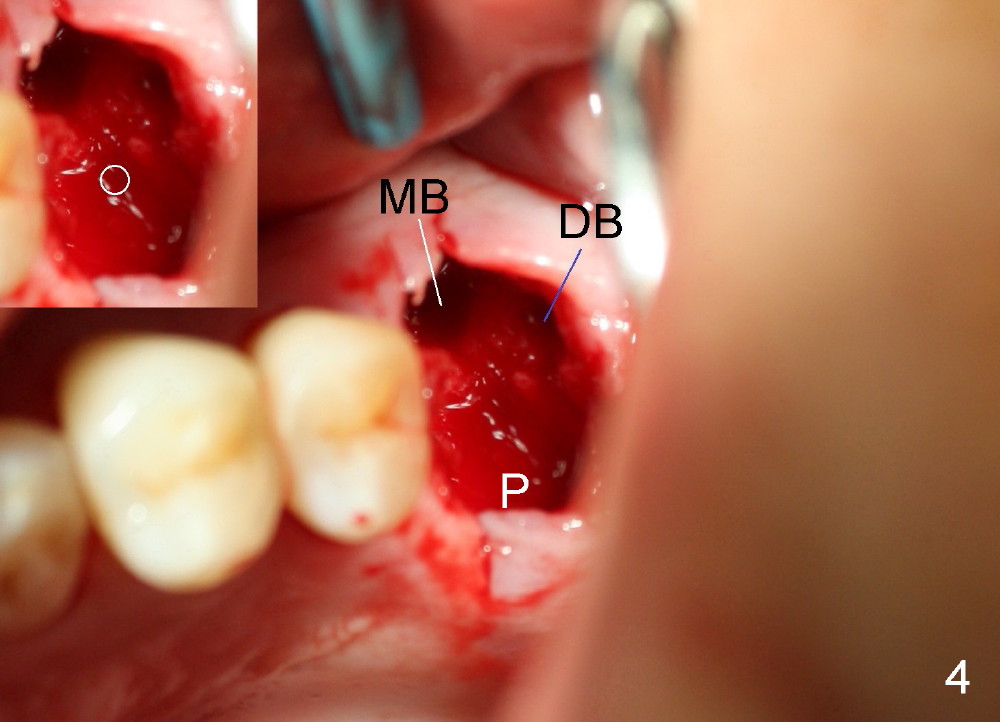
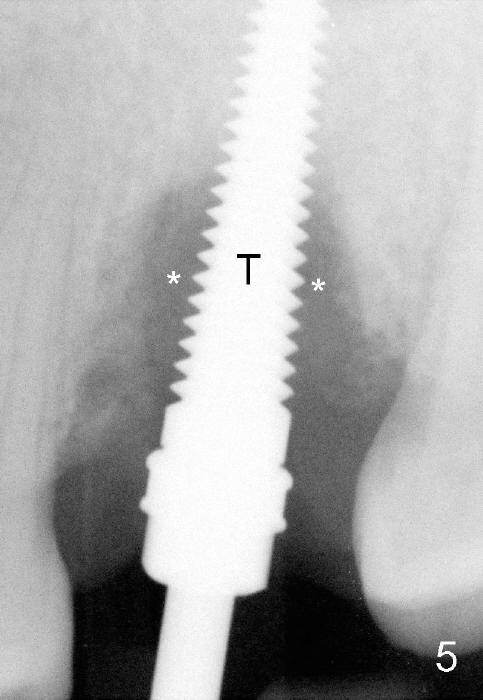
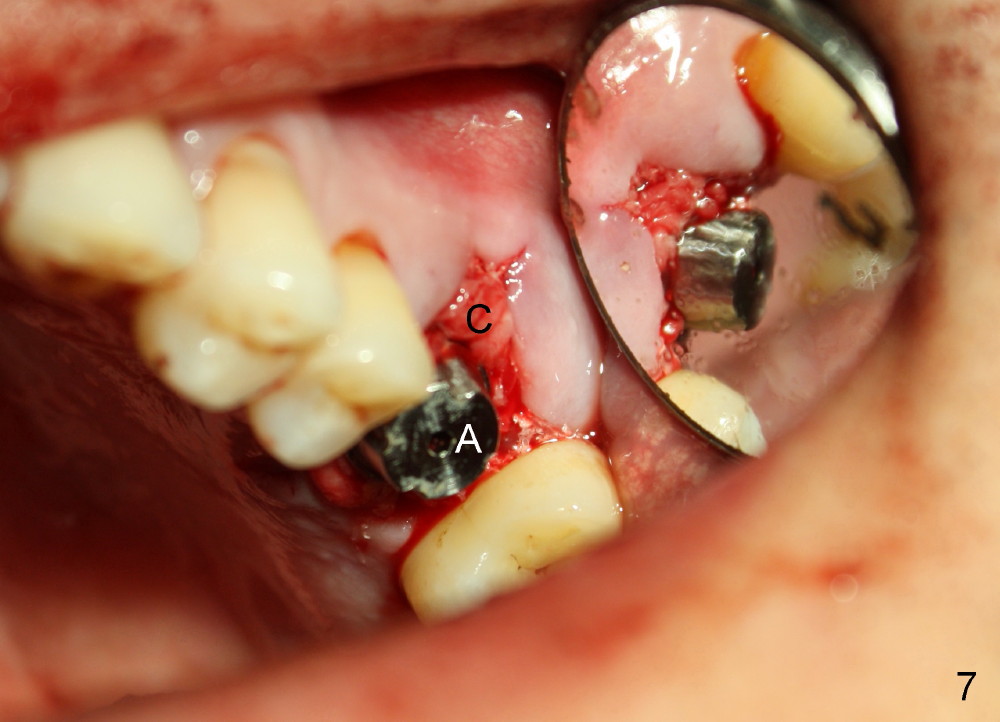
Bone density around the molars (including apical to #14) (Fig.1 black *) is higher than that around the premolar (white *). In fact the tooth has horizontal root fracture (Fig.2: <: CEJ), consistent with high bone density (strong mastication). An immediate implant is planned (Fig.3). After extraction, osteotomy starts at the buccal slope of the palatal (Fig.4 P) socket. Because of high bone density apical to the sockets, drills are required for osteotomy in the septum (type II bone) instead of osteotomes and primary stability is easily achievable (>60 Ncm). When a 7 mm implant (Fig.6 I)) is placed, the peri-implant gaps are much smaller (*) than that with a 4.5 mm tap (Fig.5 T). This helps bone grow faster toward implant. A long implant (17 mm) is necessary for this case to obtain primary stability in the apical one (double arrows in Fig.6). With reamers, a fair amount of autogenous bone is harvested during drilling, mixed with allograft and synthetic bone and placed in the remaining buccal (Fig.7) and palatal (Fig.8) sockets. The openings of the buccal and palatal sockets are covered with collagen dressing (C) and perio dressing. The latter is kept in place by a short abutment (Fig.6-8 A).
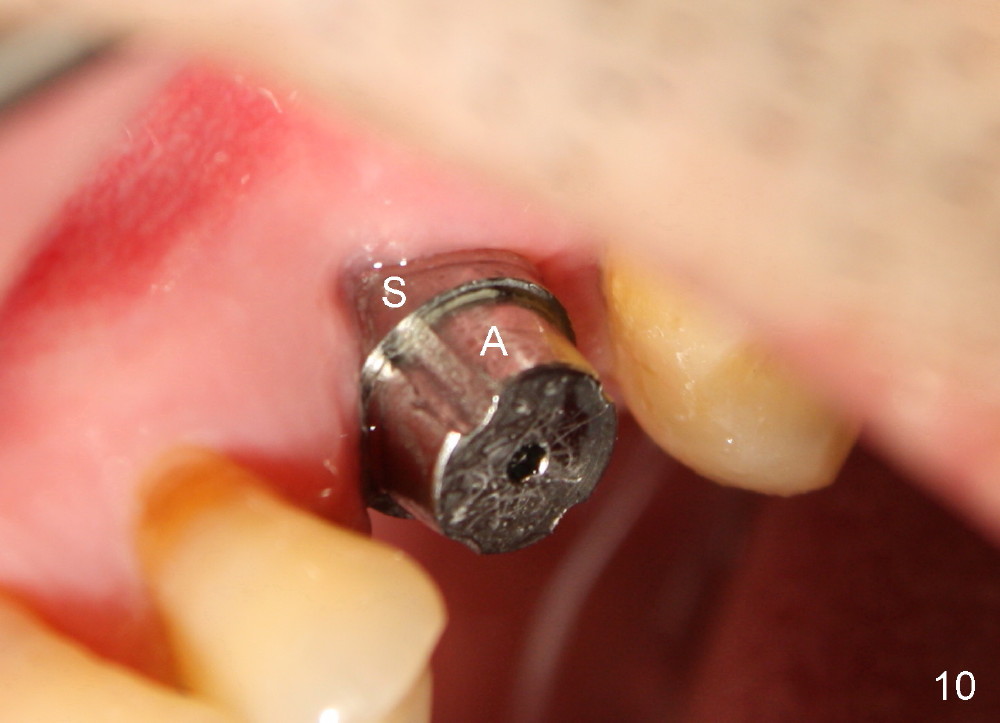
PA taken 3 months postop (Fig.9) shows bone graft in the mesial gap (*). Clinically the implant surface is less exposed buccally (Fig.10) than palatally (Fig.11 *).
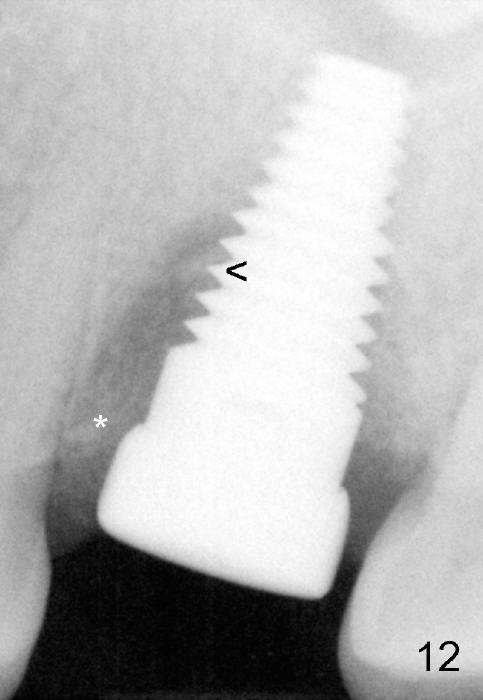
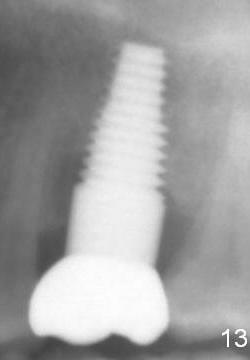
Bone appears to regenerate in the apical aspect of the mesial gap 5.5 months postop (Fig.12 <). The implant remains stable and is ready for restoration. The peri-implant radiolucency continues to reduce 1 year post cementation (Fig.13).
Return to Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 07/20/2014, last revision 01/19/2018