
|
|
|
|
|
|
Guided Bone Regeneration for Implant Thread Exposure
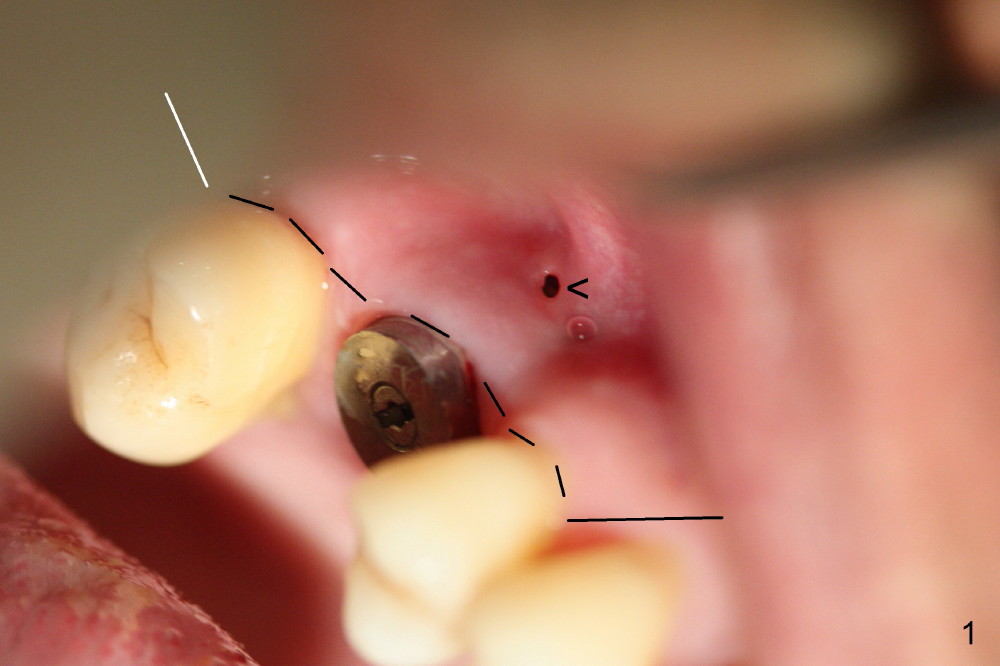
A fistula forms 3 months postop, buccal to the implant at the site of #3 (Fig.1 <). There are 2 possible reasons. First the implant was placed too buccally due to palatal root exposure before extraction. Second, the patient could not tolerate oral Amoxicillin. It is most likely that the buccal implant threads are not covered by the bone. Bone graft is required.
First, Clindamycin should be taken with Chlorhexidine mouth rinse 2 days prior to surgery. After incision (dashed line in Fig.1), the exposed threads are thoroughly irrigated, soaked with Clindamycin guaze 3 times, and treated with Perfogel and Endogain. Following allograft/Osteoten placement, Osteotape is used to cover the graft. Osteotape is a special collagen membrane with Osteogen already incorporated.
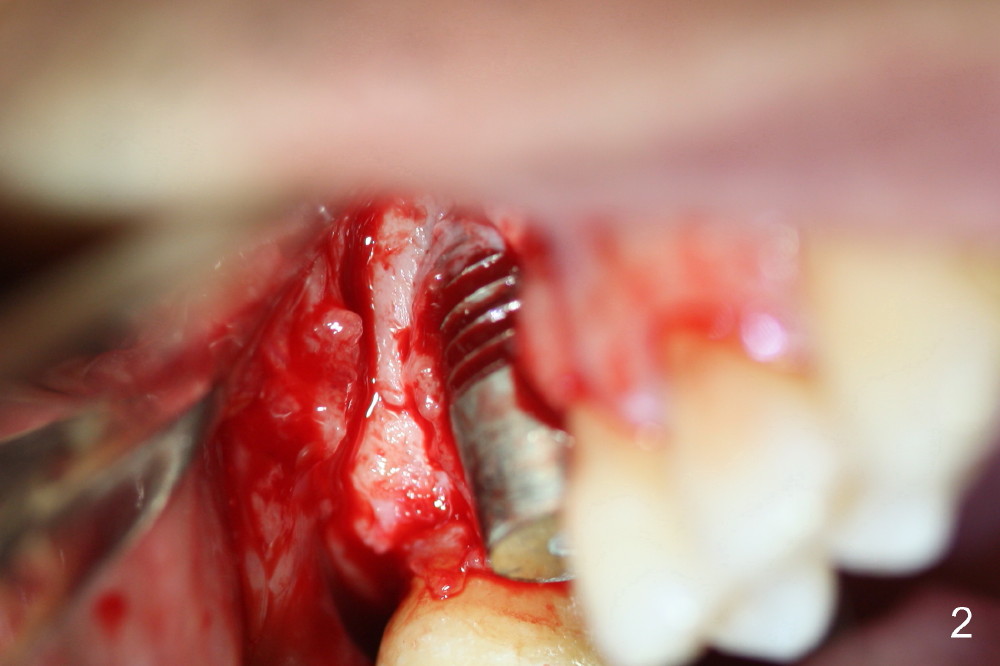
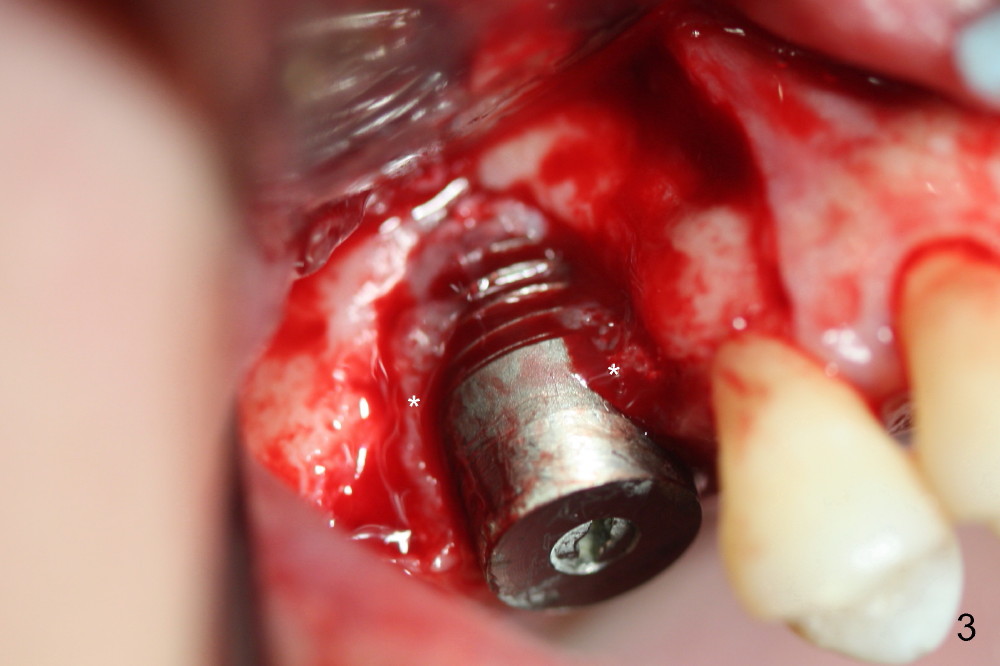
The surgery is finished as planned. Fig.2,3 (intraop photos) show thread exposure. The fistula is closed with perio glue. The defect appears to be a preexisting condition. Bone graft may be not enough or get infected. Or the implant is oversized, or placed too buccally (because of palatal defect).
The patient returns for follow up 2 and 4 weeks postop. Two weeks postop, the fistula closes after removal of perio dressing. Mesial to the healing fistula is a small wound opening, from which bone graft granule are exposed. The Osteotape is partially exposed from the gingival margin. Four weeks postop, the osteotape is not visible from the recessed gingival margin (Fig.4). The fistula remains close (single arrowhead: <)), whereas the small wound opening mentioned above has closed (double arrowheads: <<). Gingival graft should have been done with GBR to decrease the chance of gingival recession. A second GBR appears necessary.
Return to Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 12/25/2014, last revision 04/12/2015