




|
|
|
|
|
|
|
|
|
|
Atypical Trigeminal Neuralgia or TMD
A 56-year-old lady has a peculiar history of pain. At first an upper left molar has pain. After unsuccessful root canal therapy, the tooth is extracted. The pain does not go away. It persists after socket debridement. When she presents to our clinic, a med for trigeminal neuralgia is prescribed. It reduces pain. When it is not taken, the pain returns. Brain surgery is indicated if the diagnosis is correct.
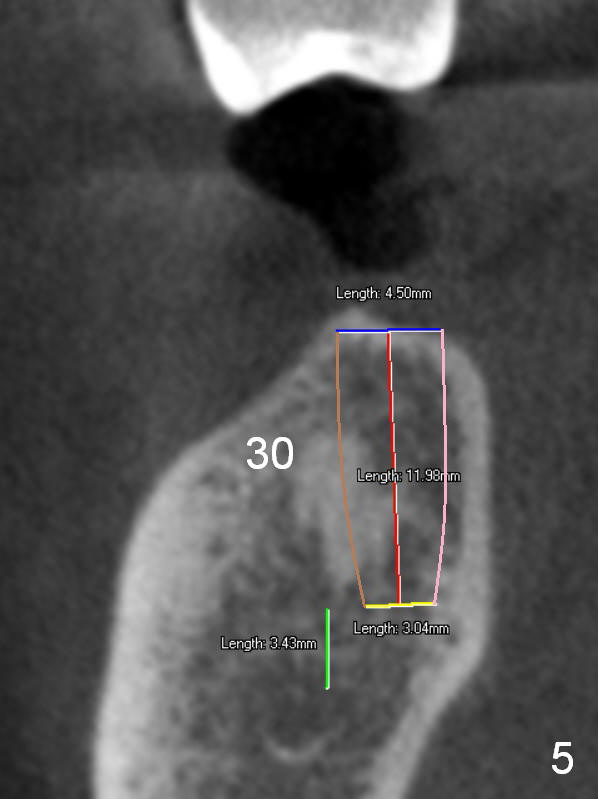
On the other hand, her occlusion is out of order. The teeth #2,14,15,30 and 31 are missing with #3 supraeruption and deep anterior overbite and overjet (Fig.1,2). This may lead to TMD. Alginate impression will be taken for fabrication of night guard or occlusal guard to raise vertical height. If this helps, implants are placed (Fig.3-6), followed by limited or comprehensive ortho to intrude #3, to permanently change her occlusion.
In fact she has a night guard, which is not used. Before restoring the missing teeth, the tooth #7 develops pain due to caries underneath crown. After root canal therapy, the tooth fractures.
Return to Upper Arch Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 01/20/2016, last revision 01/19/2018