










|
|
|
|
|
||
|
|
|
|
|||
|
|
|
|
|||
|
|
|
|
|||
|
|
|
|
|
||
Where to Use the Longest One-Piece Implant?
Most of patients do not like removable dentures. A clumsy flipper for a small lower incisor does not sound a good idea. They also want a treatement with quick turnaround.
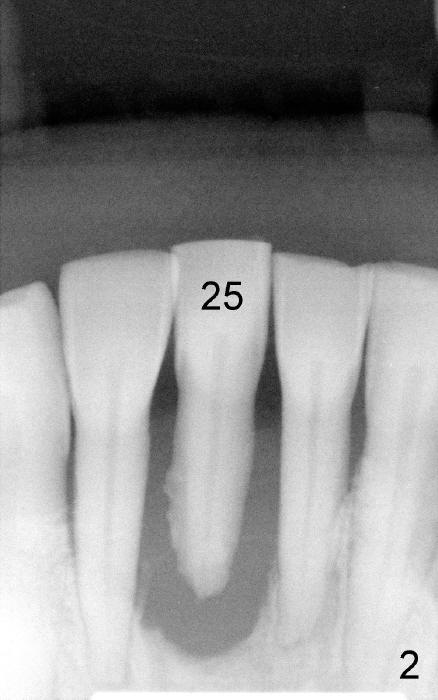
A 50-year-old female amateur dancer has a mobile lower right central incisor (Fig.1,2). She is pleased to learn that we can give her a stable tooth immediately after extraction. Treatment plan is accepted easily.
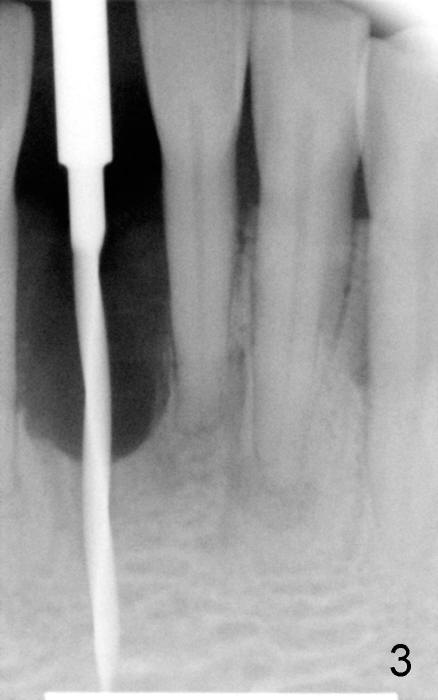
Severe bone loss around this incisor dictates use of a long one piece implant (3 x 23 mm; Fig.4 after using 1.5 mm pilot drill (Fig.3)), followed by bone graft (Fig.5 demineralized cortical human allograft, Impladent). The longest implant available is 23 mm. The long implant is the basis for high insertion torque, 55/60 Ncm. An immediate provisional is provided (Fig.6,7). There is hemorrhage during osteotomy, probably due to penetration of the Incisive vessels. Hemostasis is achieved when the implant is placed.
Special to the placement of the long implant is that it is difficult to provide sound anesthesia with infiltration. Inferior alveolar nerve block is required for profound anesthesia, possibly because of innervation from the incisal nerve.
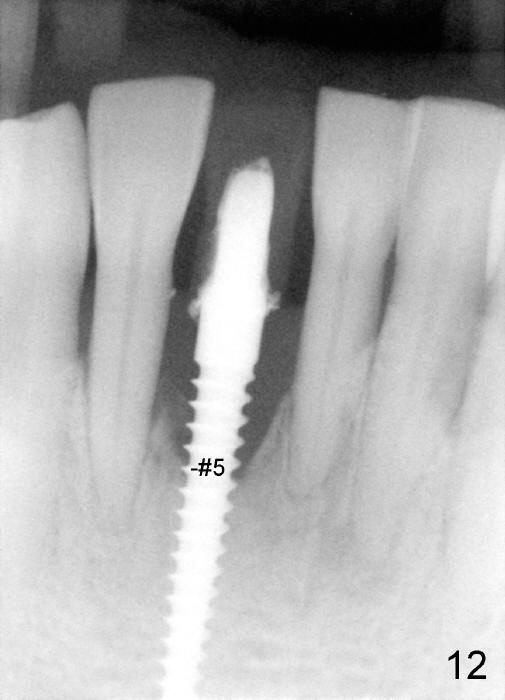
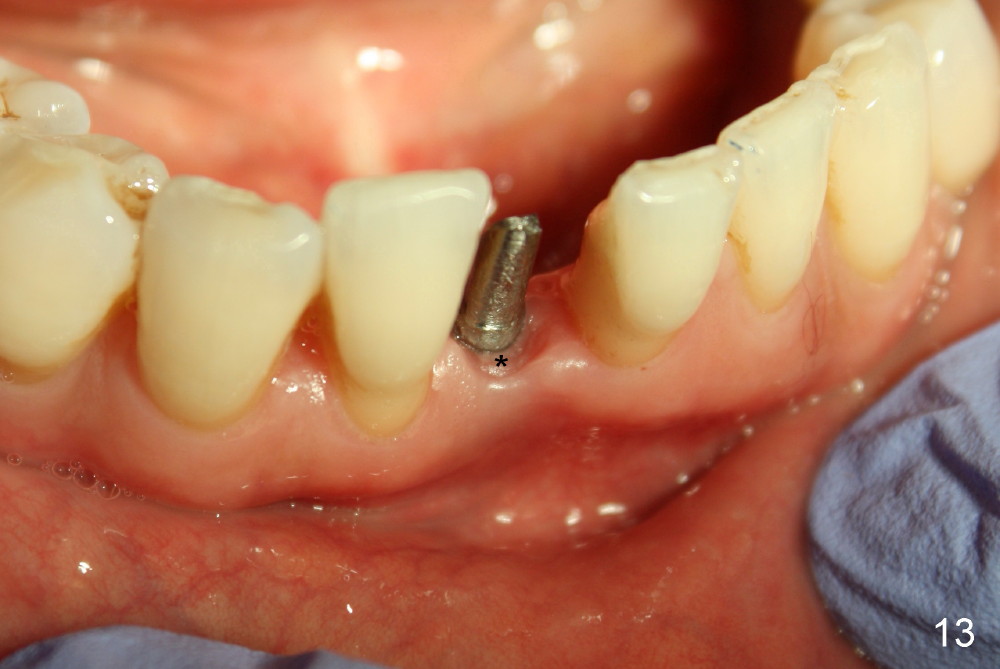
The patient returns for follow-up 9 days postop. She is doing well except that the tongue is irritated by the rough surface of the provisional. After adjustment of the margin of the provisional, the patient leaves in a hurry for her performance rehearsal (Fig.8,9). As compared to immediately postop (Fig.6,7), gingival inflammation (*) disappears in a fast fashion. The patient returns for provisional recementation 14 days postop (Fig.10) and crown impression 6.5 months postop (Fig.11, 12). Note the wound healing and bone growth. When the patient returns for crown cementation 7 months postop, the provisional is loose. The temporary cement has been dissolved; the gingival tissue surrounding the implant looks fresh and healthy, seemingly having good seal (Fig.13 *). The definitive crown (Fig.14 C) looks harmonious with the gingiva. It is expected that the papillae will partially fill in the gingival embrasures (Fig.15 ^) in the near future, considering improved oral hygiene and normal hard and soft tissue growth.
In brief, immediate implant/provisional offers practical and reliable service.
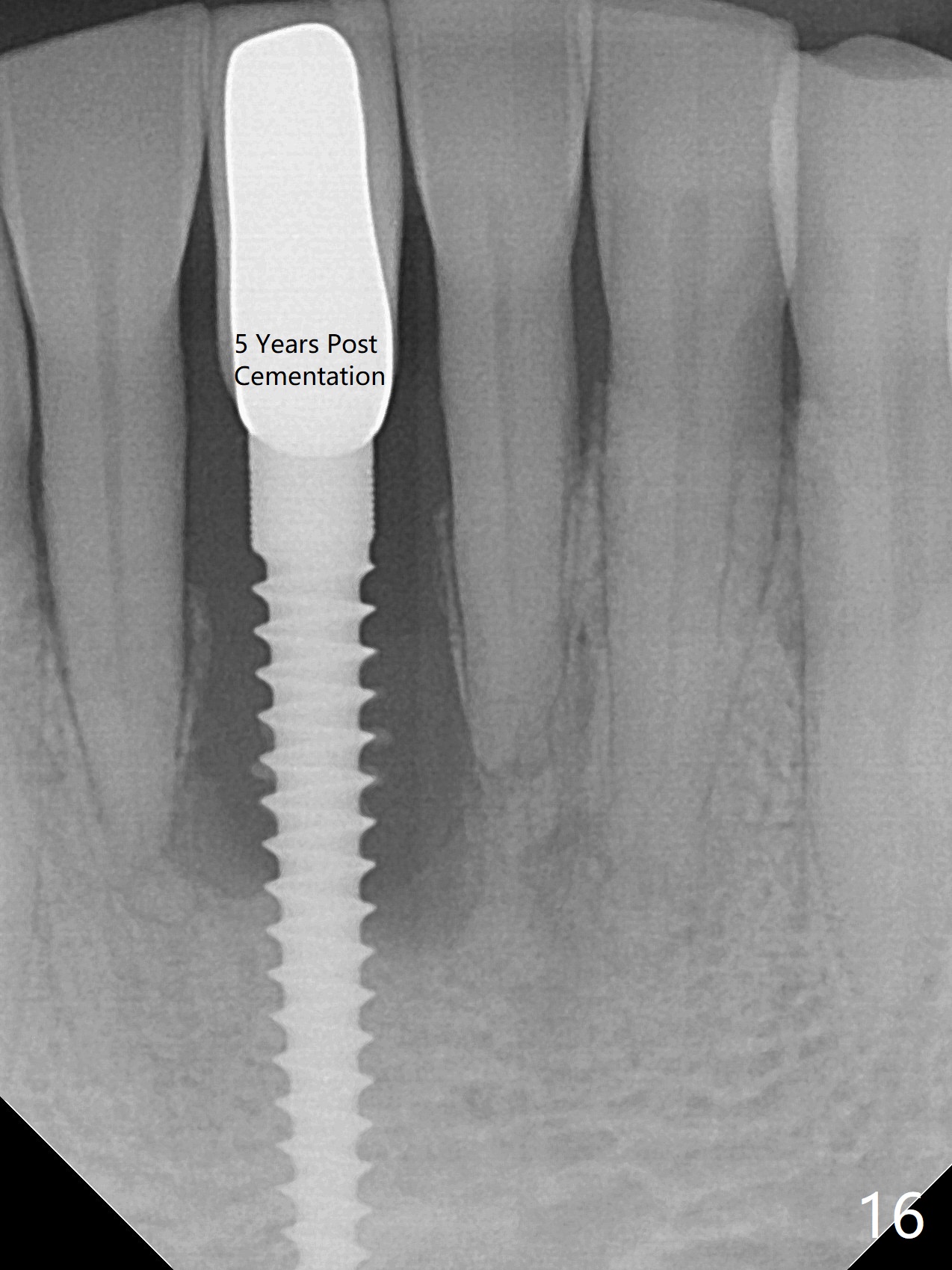
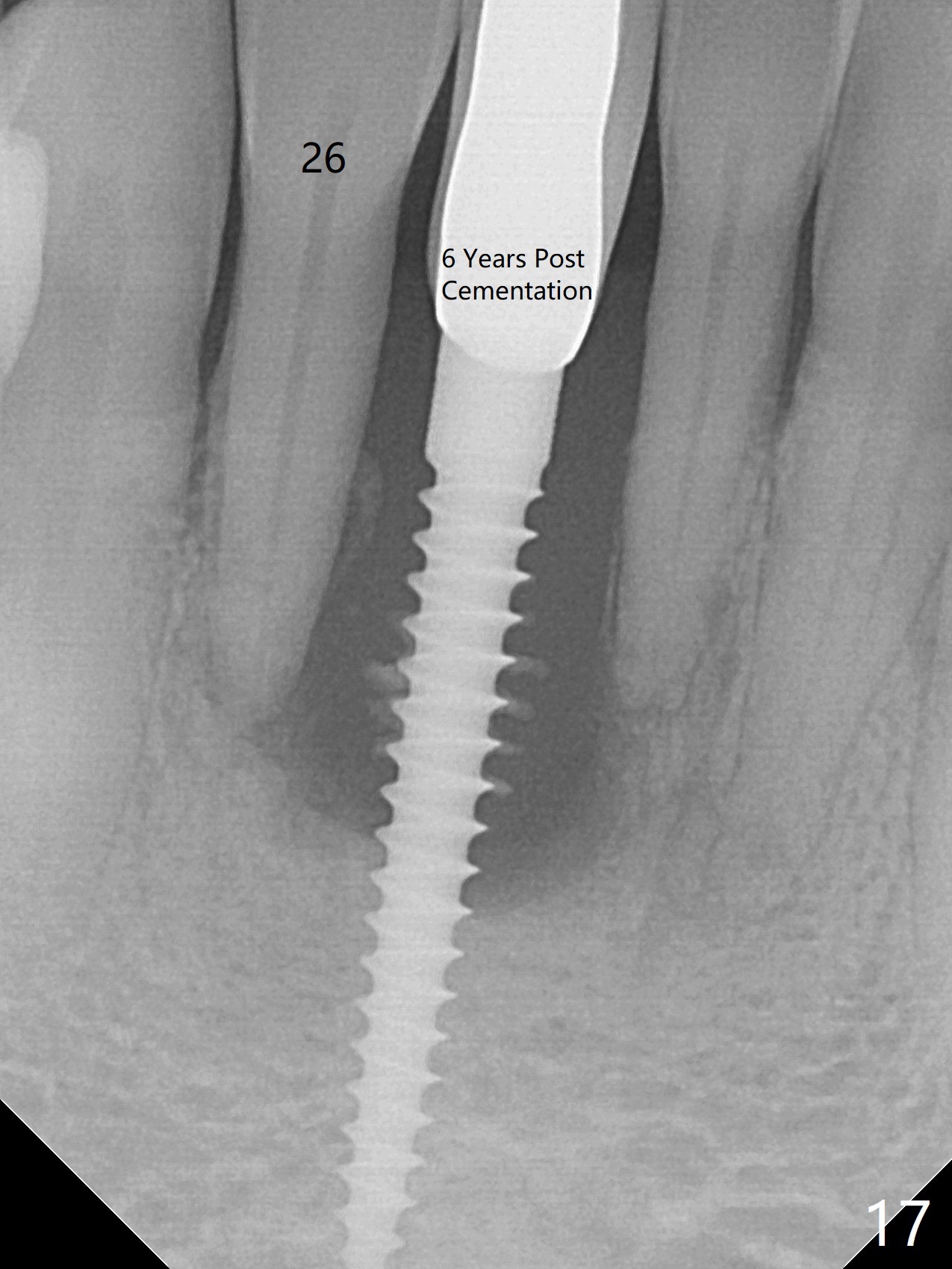
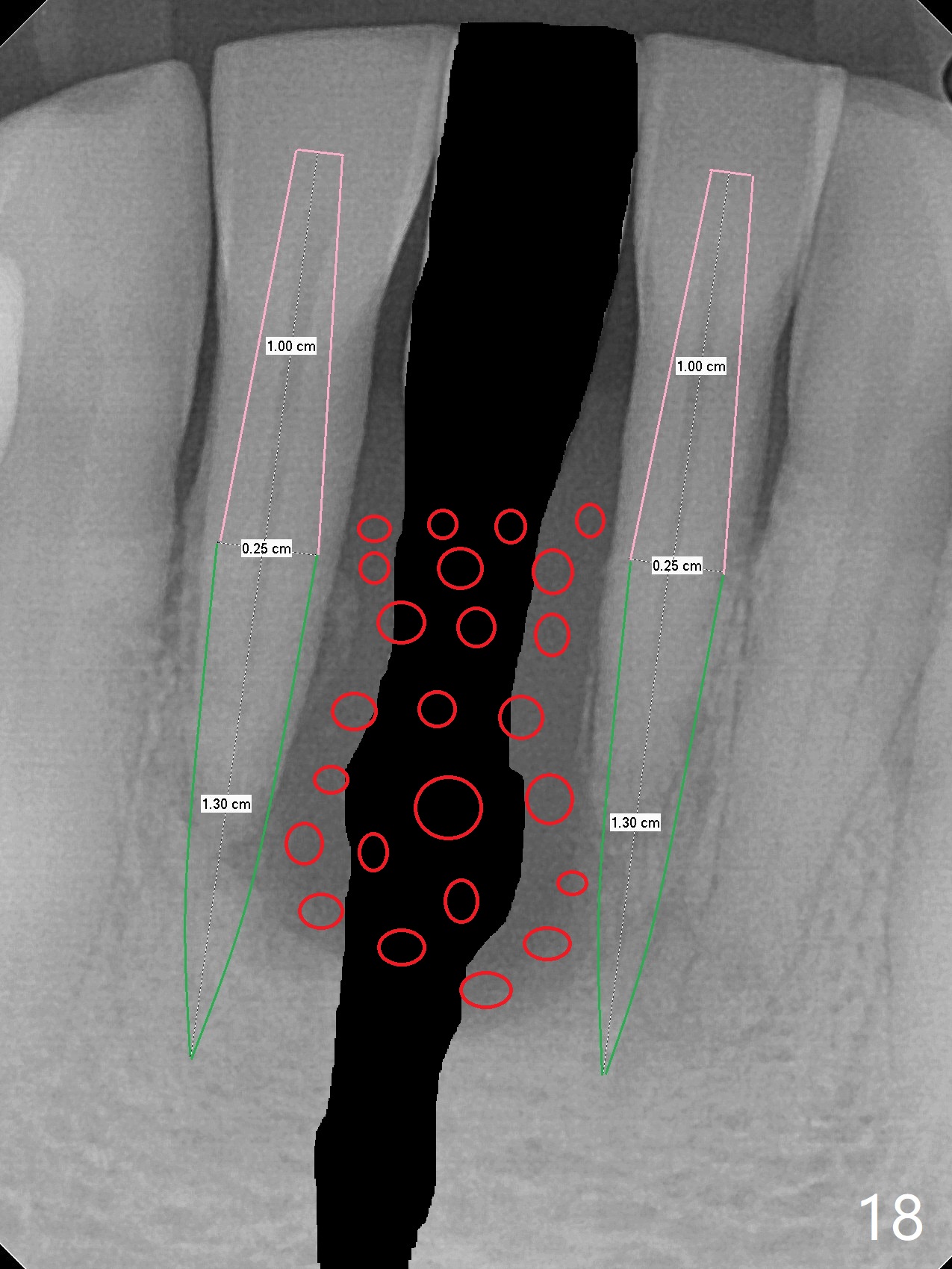
There is no improvement of bone loos at #25 implant 5,6 years post cementation (Fig.16,17). The tooth #26 is mobile. It appears that the implant should be removed or truncated, while IS 1-piece 2.5 mm implants are to be placed at #24 and 26 with plenty of bone graft in between (red circles).
Xin Wei, DDS, PhD, MS 1st edition 01/18/2014, last revision 09/03/2020