|
|
|
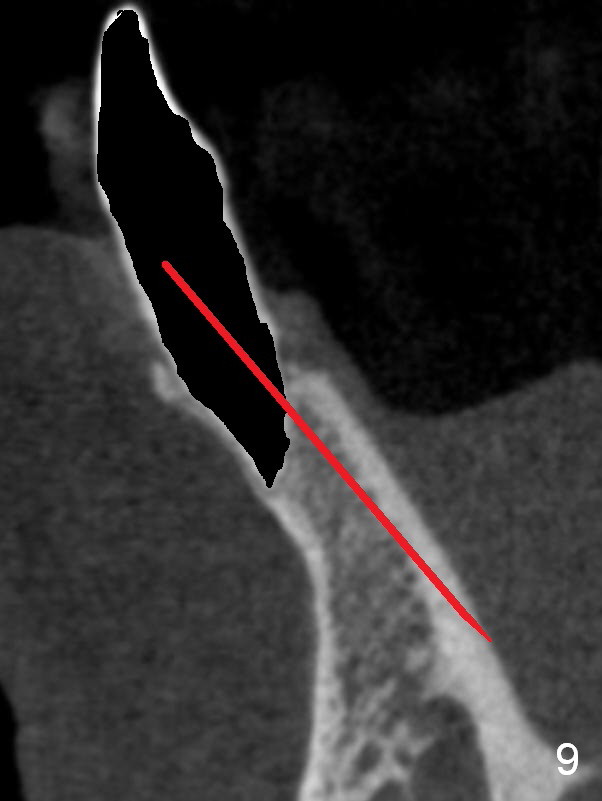
When the pilot drill extends to 20 mm, there is sudden empty feeling. The lingual plate has perforated (Fig.9).
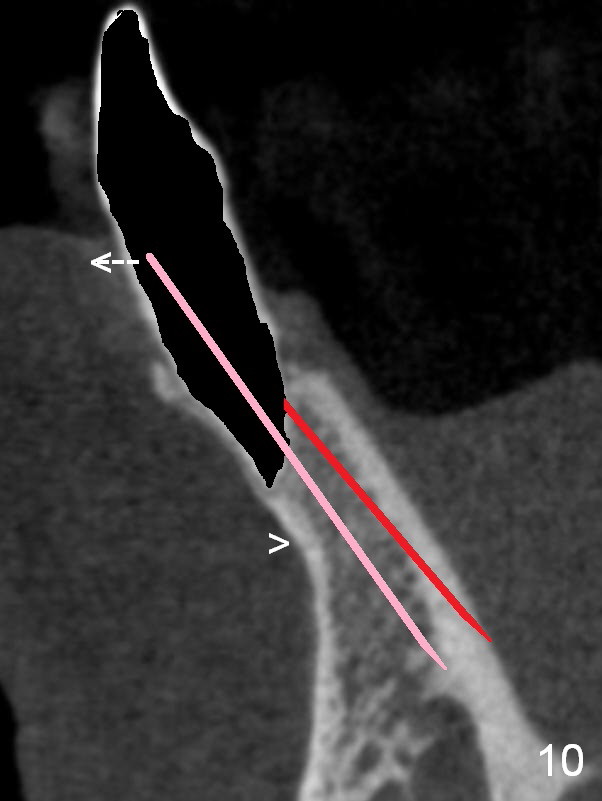
A new osteotomy is established buccally (Fig.10 pink). To avoid buccal plate perforation, especially in the buccal undercut area (>), the coronal end of the drill has to be tilted buccally (<--).
Retrospectively, a shorter implant (3x17 mm instead of 3x20 mm) should be ok with a better angulation for restoration. The apical lingual perforation should heal by itself. It should not interfere with implant stability.
More exactly, the initial osteotomy depth is controlled at 14 mm. If it is stable, extend another 3 mm after X-ray confirmation of trajectory mesiodistally.
Xin Wei, DDS, PhD, MS 1st edition 03/07/2015, last revision 01/19/2018