|
|
|
|
|
|
|
|
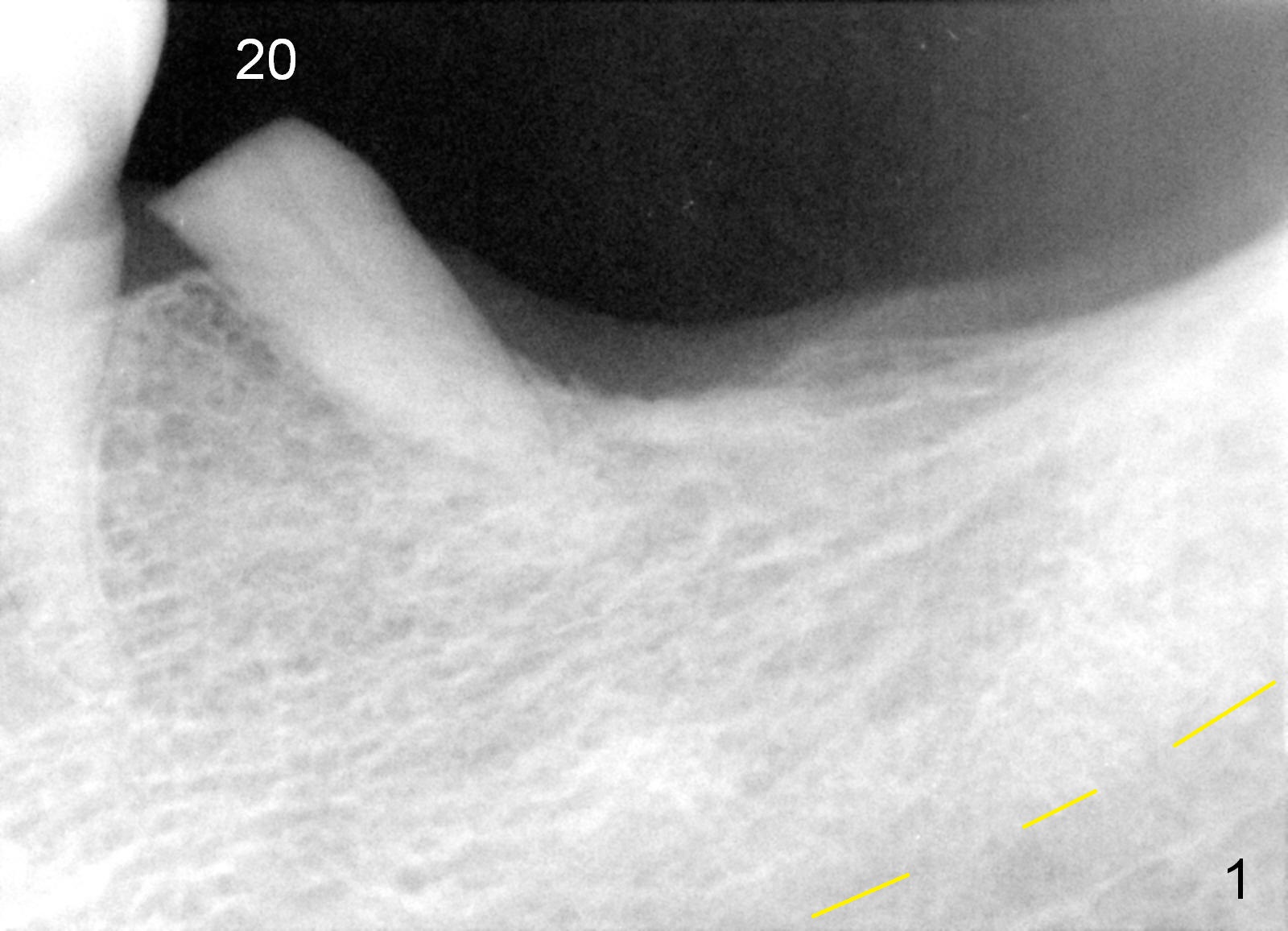
Change in Long Axis While Immediate Implanting
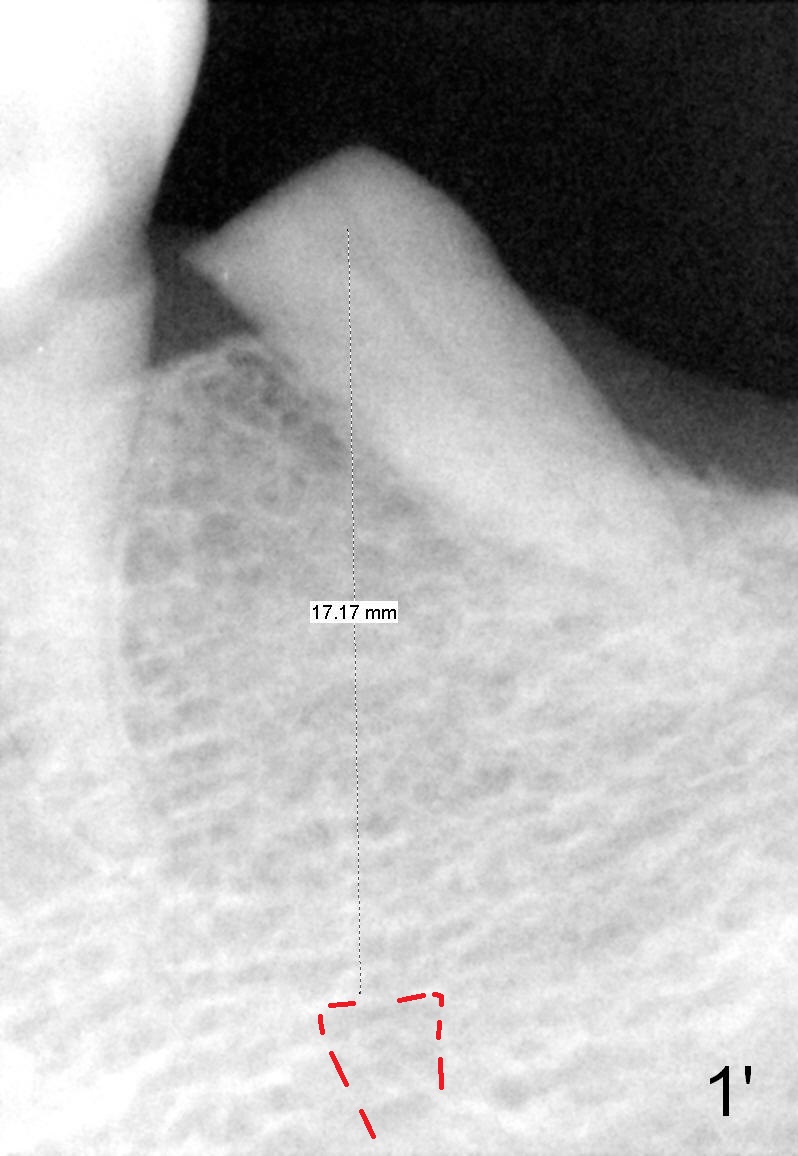
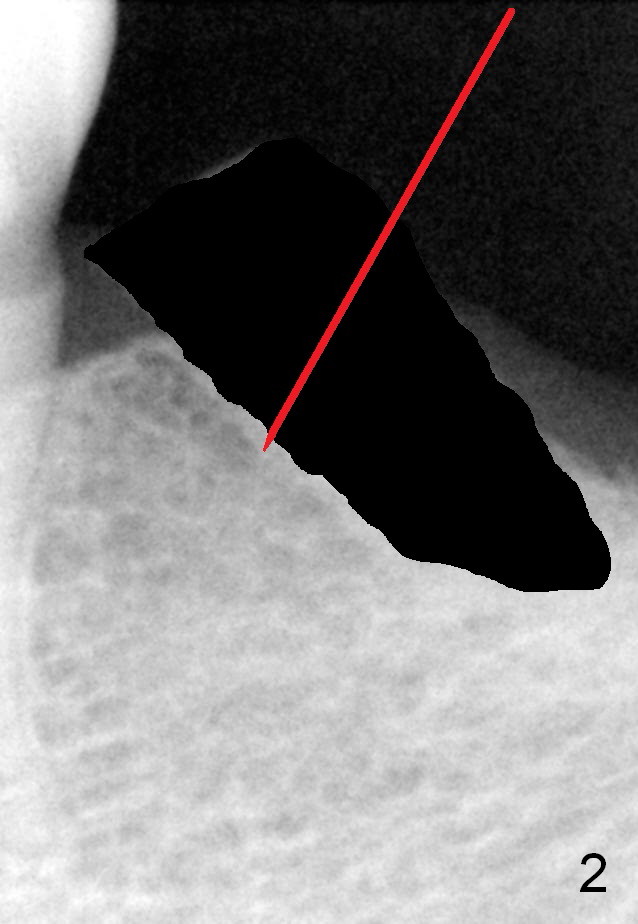
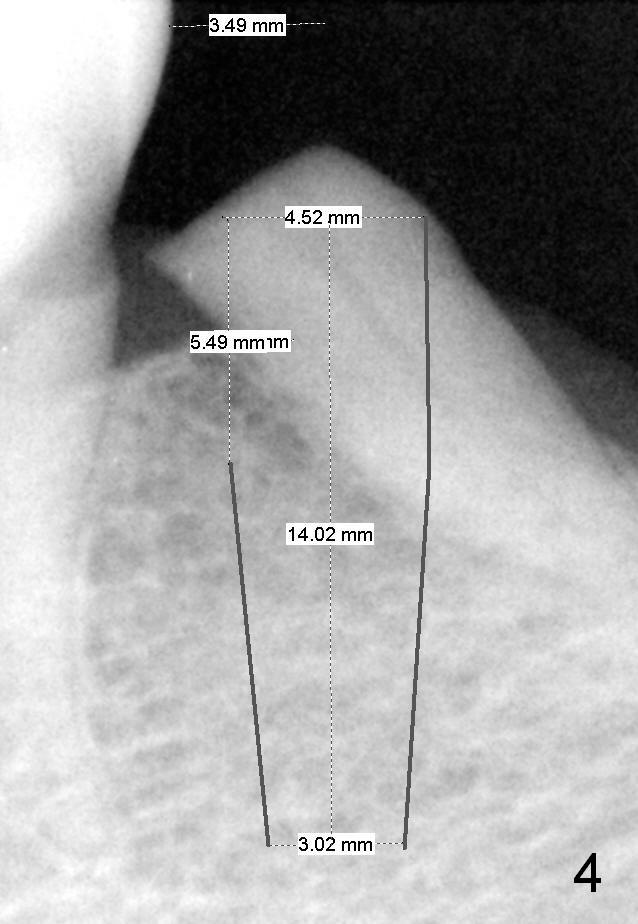
A 78-year-old lady is scared of dentistry, but she has no problem having a 2nd immediate implant (#20 in Fig.1) once the 1st one turns out to be without pain. The challenge associated with #20 is its long axis. After extraction, the osteotomy is initiated in the mesial socket wall at the junction of the upper and middle 1/3 obliquely (Fig.2, slightly lingually). Once the entry is obtained, the axis of the pilot drill is changed to be parallel to the neighboring tooth (Fig.3); an implant spacer of 2.5 mm is used to check (against the 2 mm pilot drill) so that the center of the osteotomy is 3.5 mm from the neighboring tooth (Fig.4). The implant will be 4.5x14 mm. The depth is not longer than that of the neighboring tooth so that it should be quite safe relative to the Mental Loop and the Inferior Alveolar Canal (yellow dashed line in Fig.1). The apical socket is packed with collagen dressing while the coronal one with bone graft. An immediate provisional will be fabricated to keep the graft in place. The osteotomy should be as lingual as possible to avoid the Mental Loop (Fig.1' red dashed line).
Return to
Lower Bicuspid
Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 04/26/2015, last revision 12/26/2018