|
|
|
|
|
No Implant, No Extraction
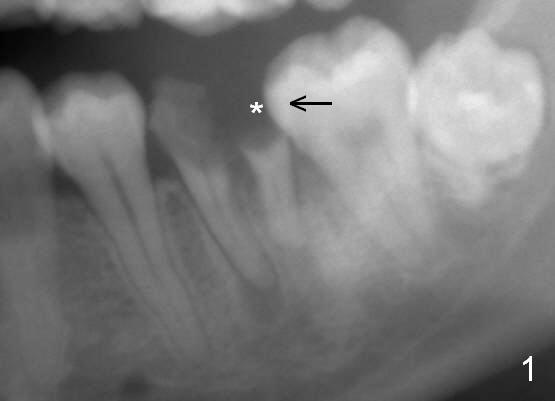
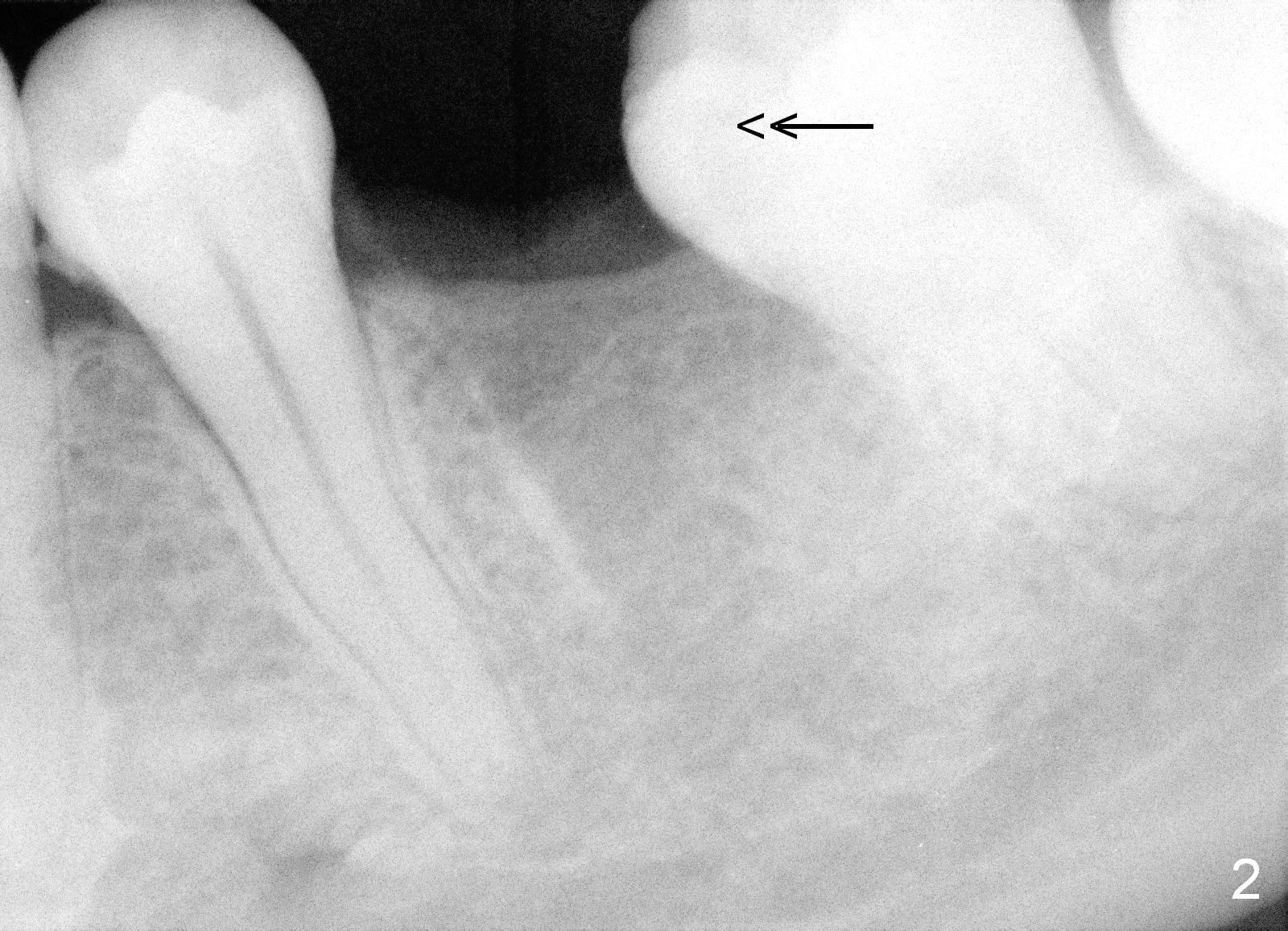
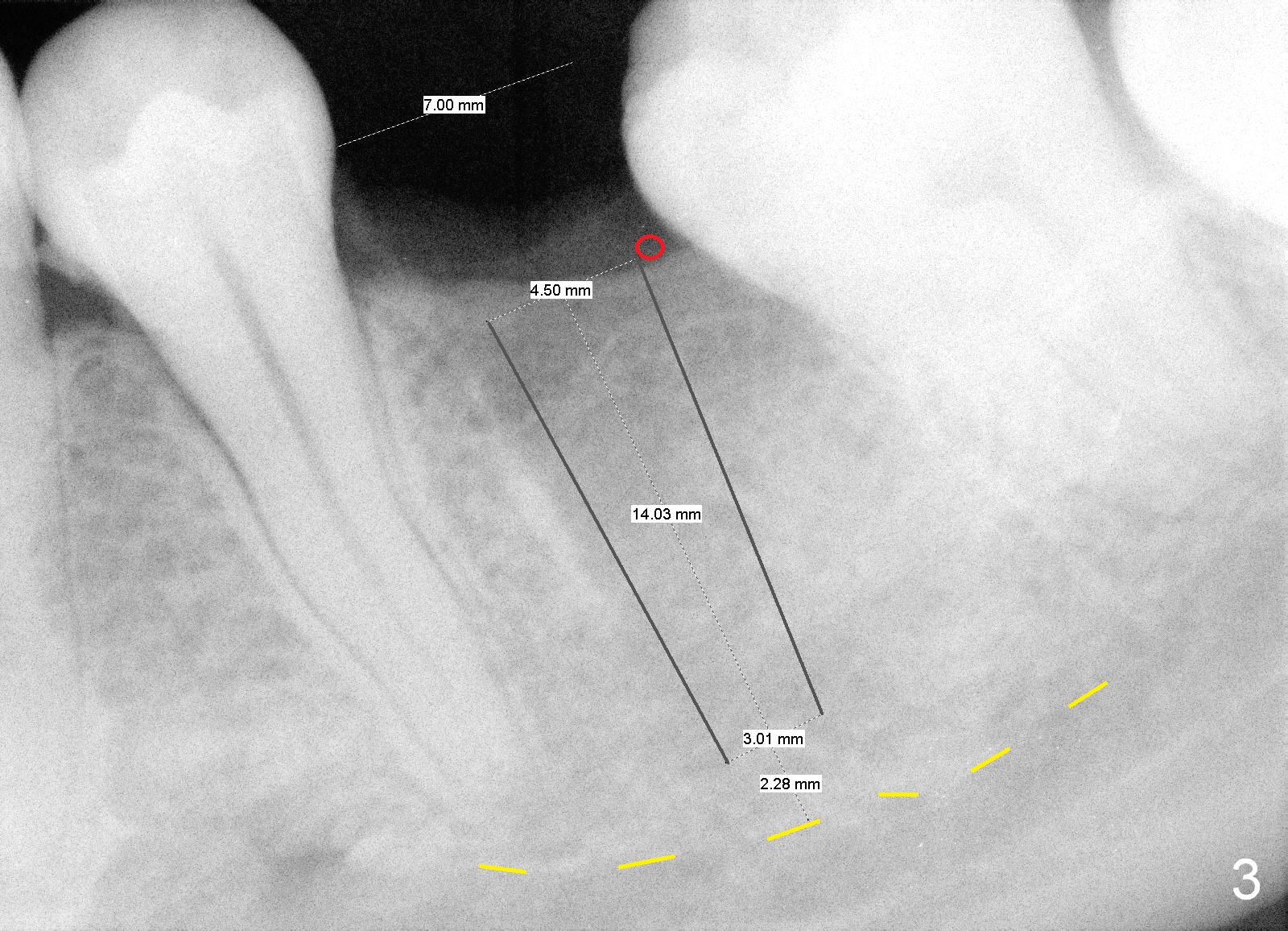
A 29-year-old man presented for #19 extraction a year ago (Fig.1). Probably due to long-termed loss of the distal portion of the crown of #19 (*), the tooth #18 has undergone mesial tilting (arrow). Now he returns requesting implant, but the tilting is worse (Fig.2 double arrows). What X-ray cannot show is severe atrophy buccolingually, increasing difficulty in implant placement. A much smaller implant can be placed (Fig.3), as compared to an immediate implant.
Reamers are used for osteotomy and saving the autogenous bone with control of depth. Bone graft is most likely placed buccodistally (Fig.3 red circle). To prepare the recipient site (decortication), surgical handpiece is needed. Long-termed resorption membrane is cut to cover the graft.
No implant, no extraction is our principle. Severity of the ridge atrophy is most striking when it is being handled.
Return to
Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 05/17/2015, last revision 12/09/2018