



|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
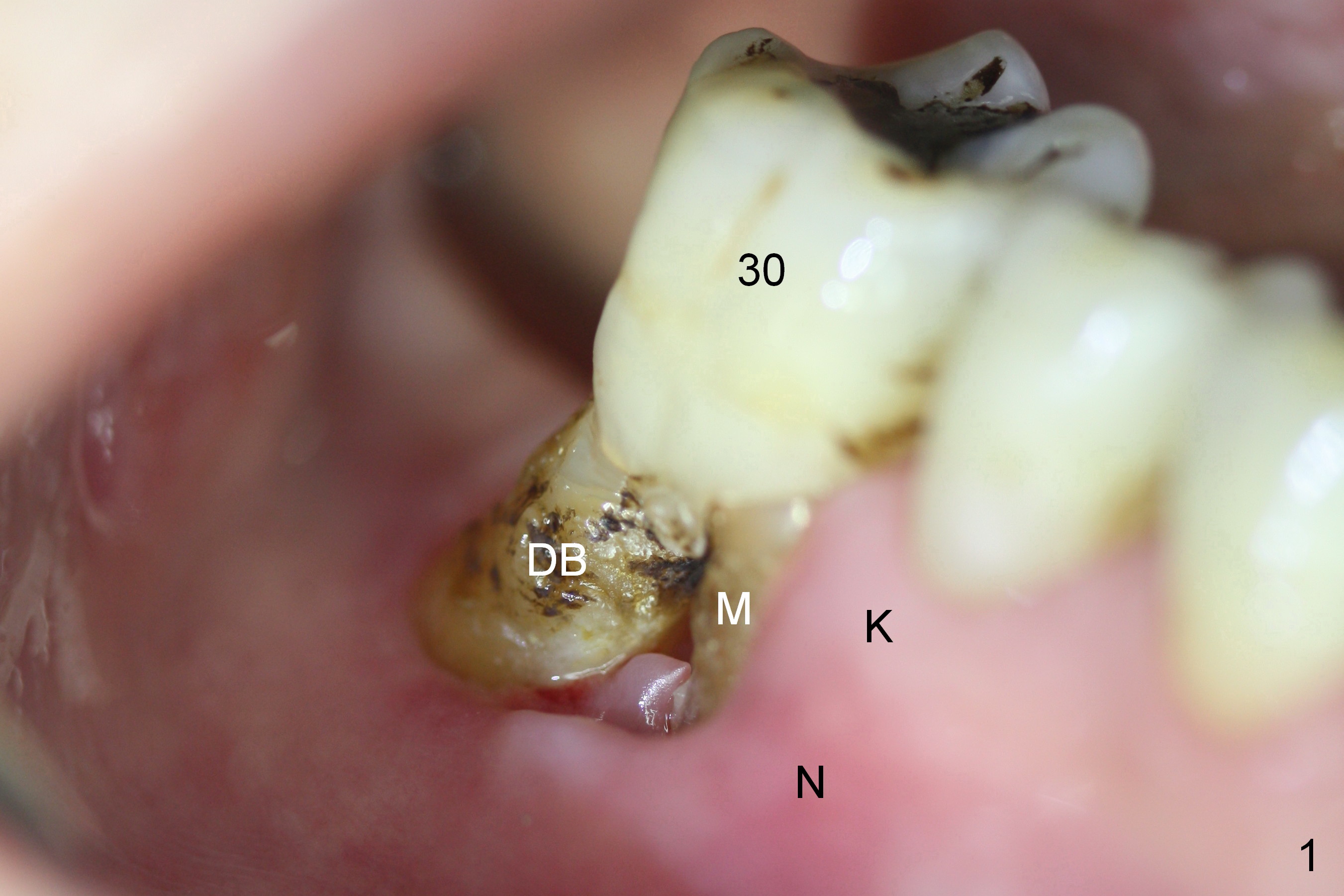
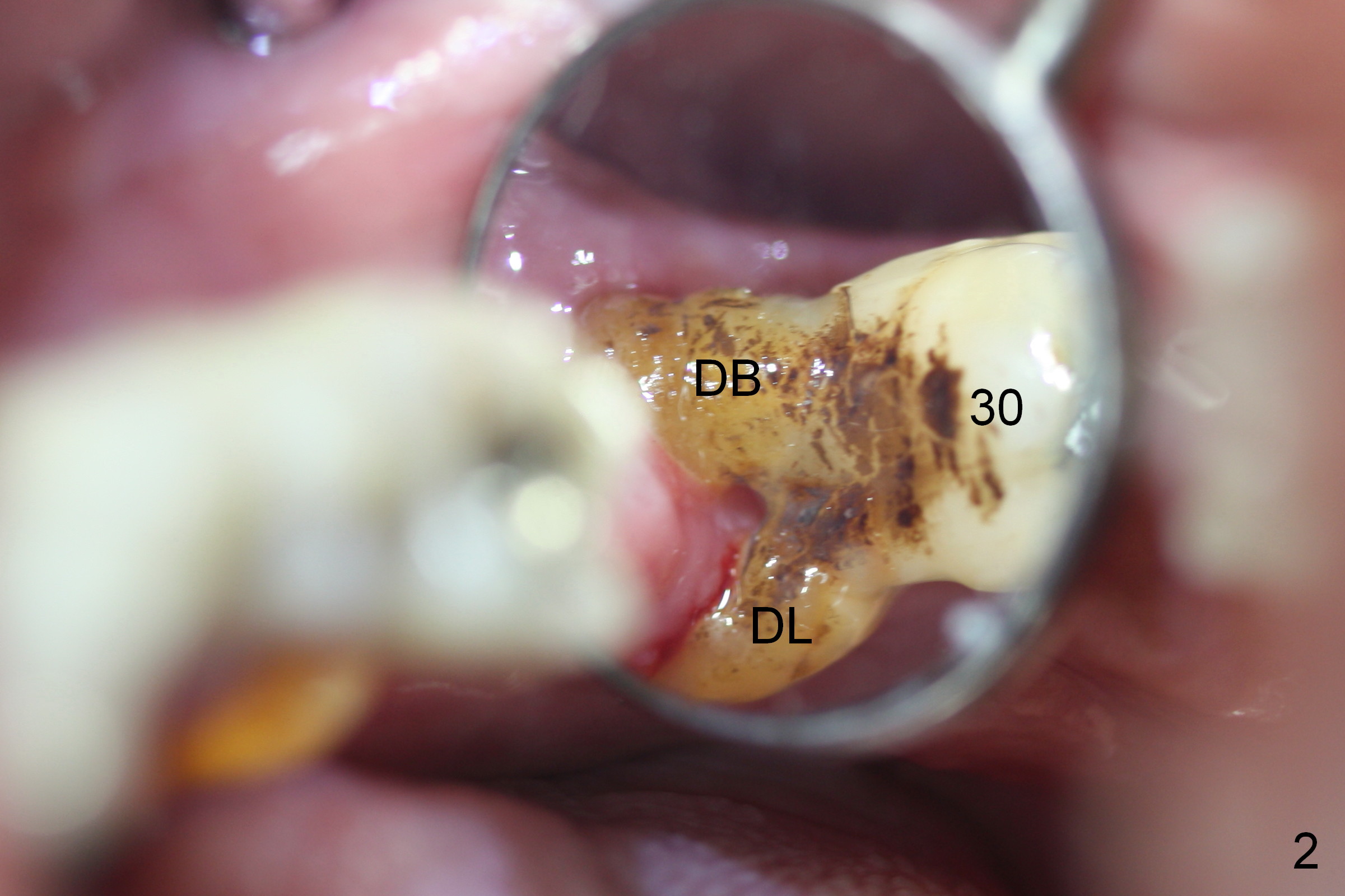
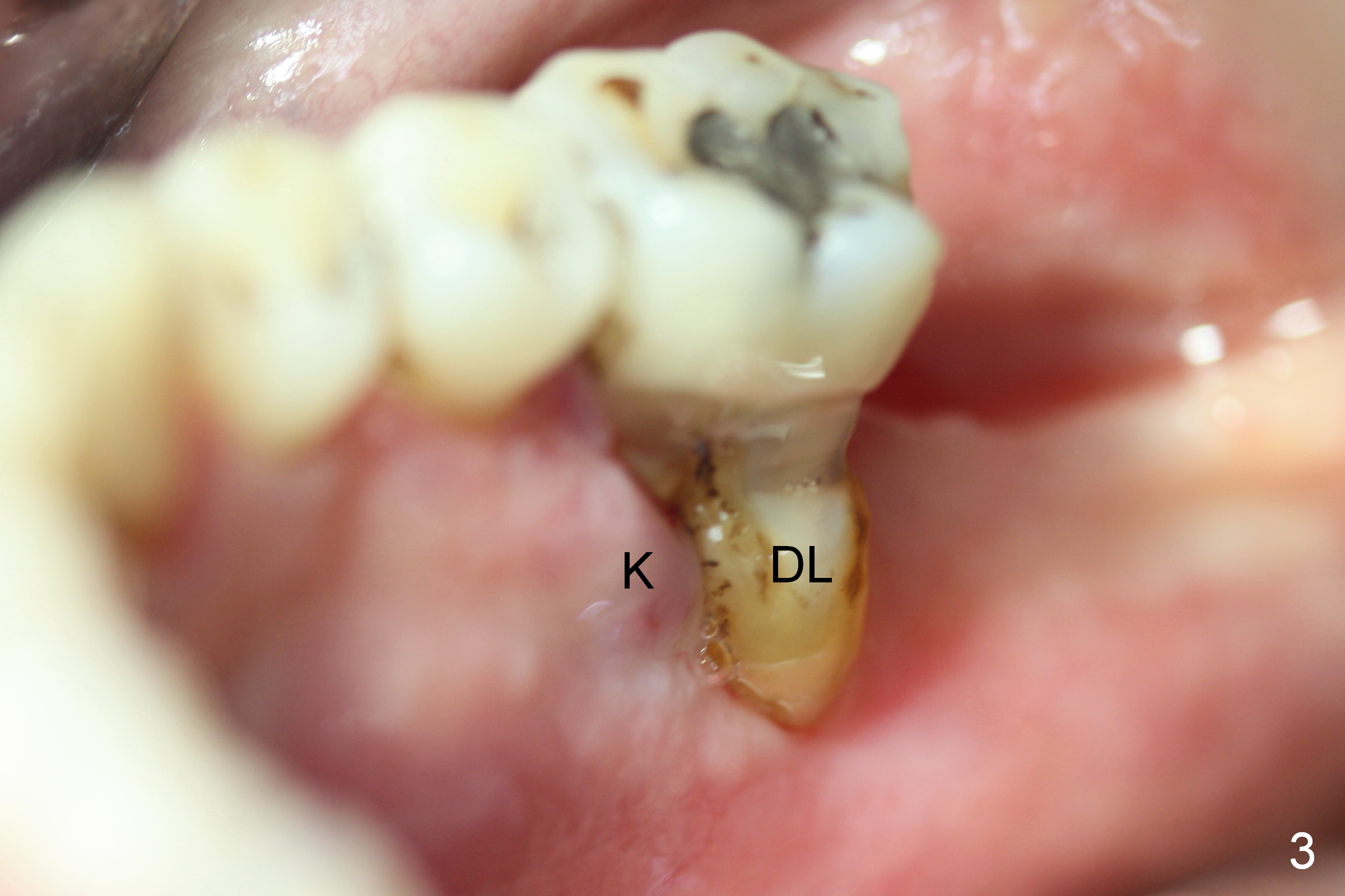
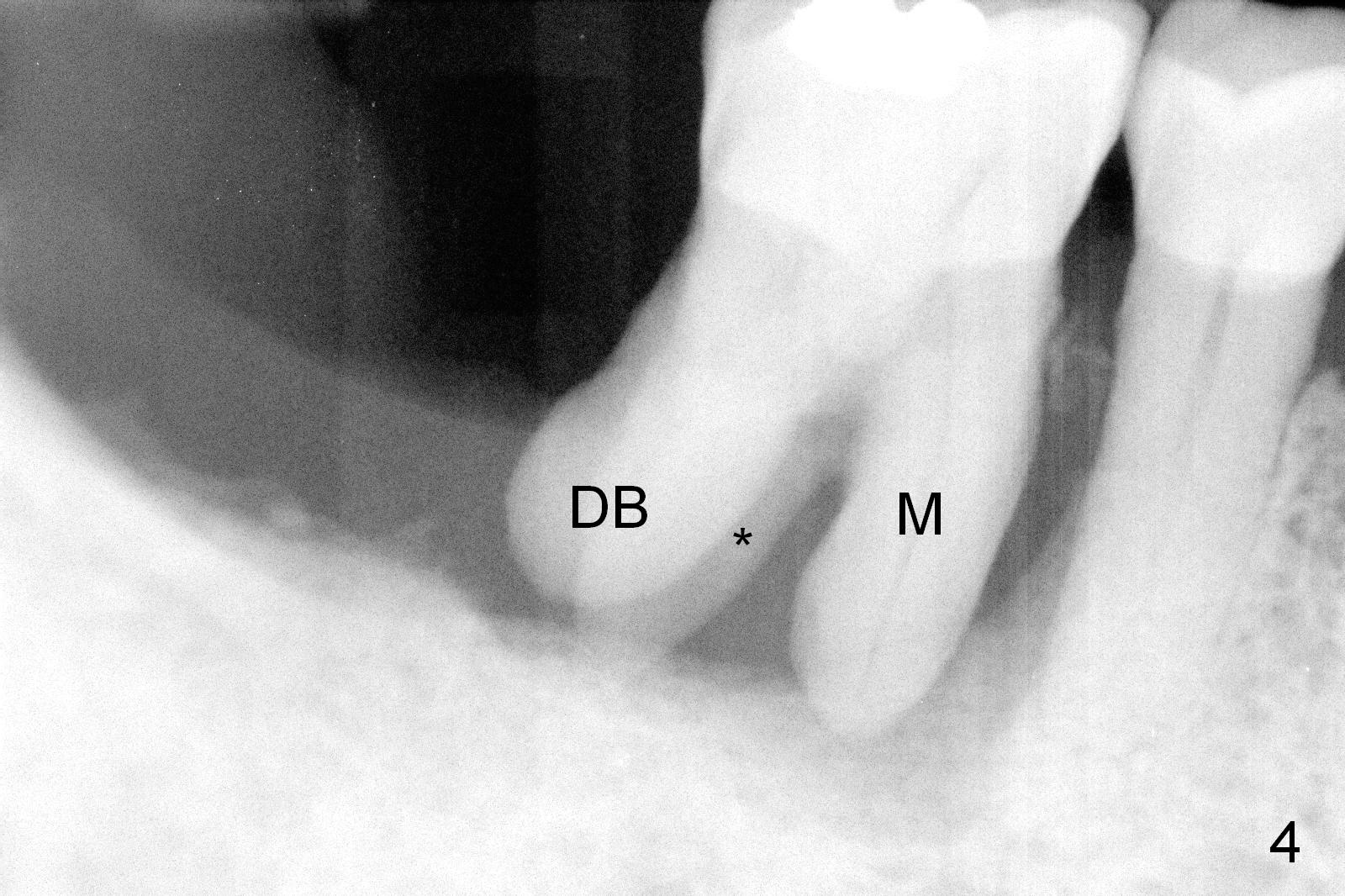
Use of Non-Resorbable Membrane to Repair Gingival Defect
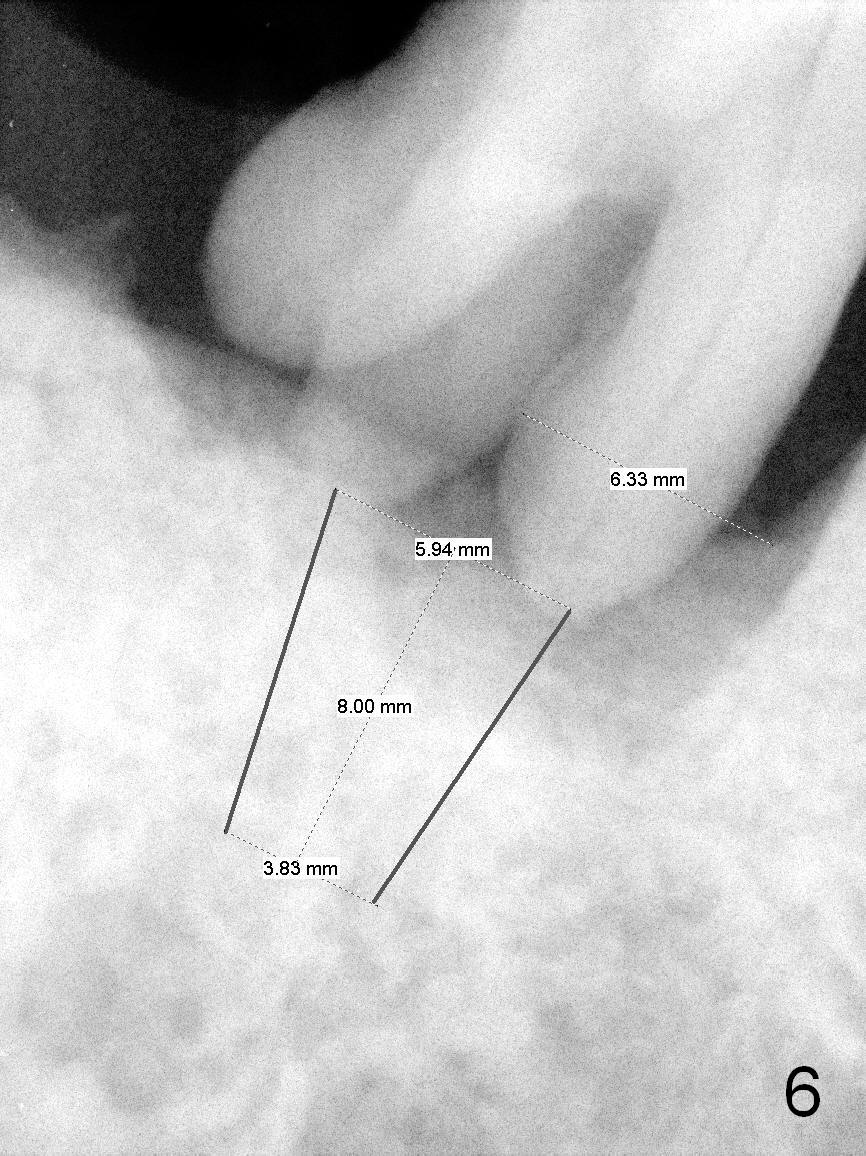
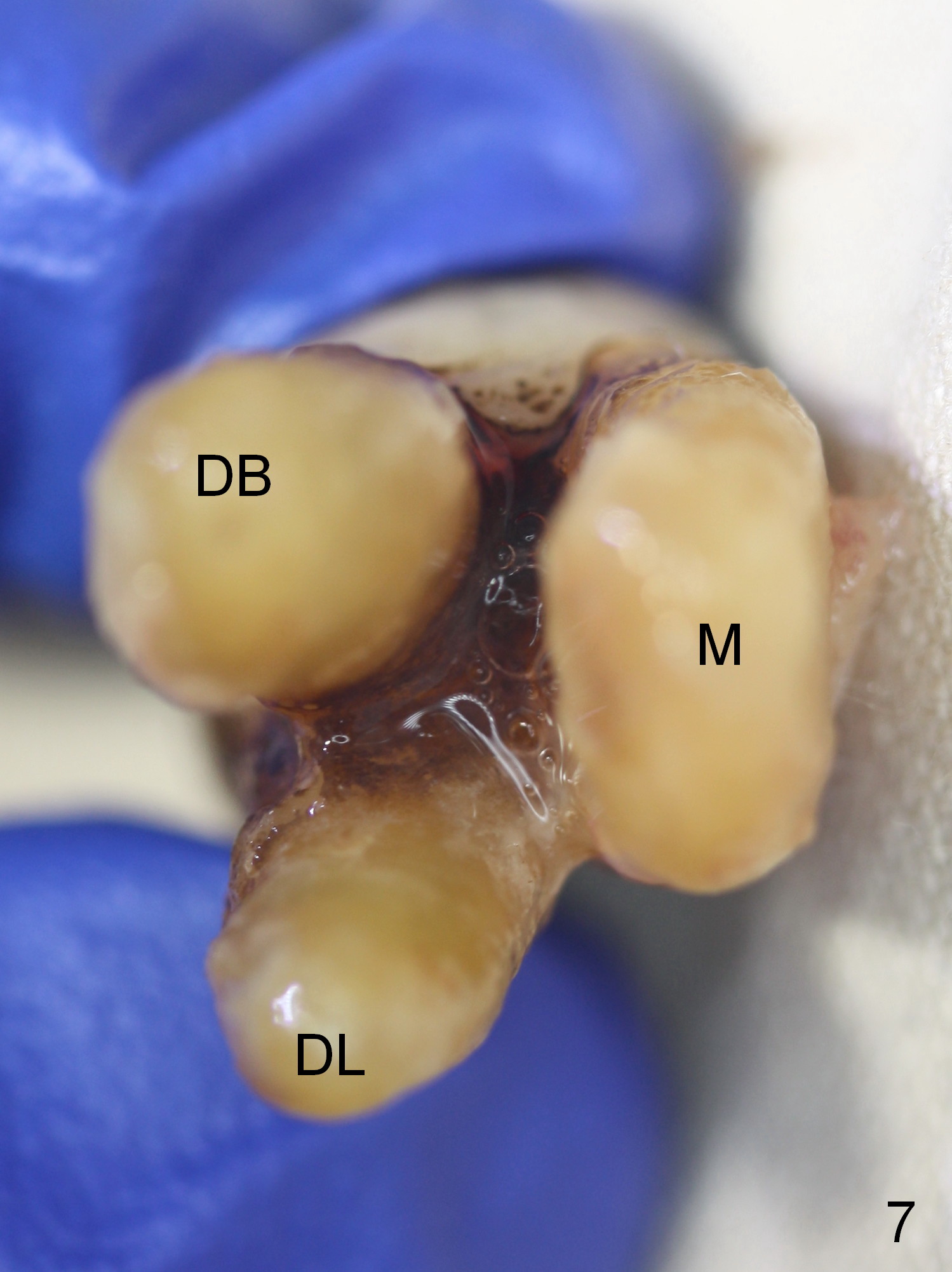
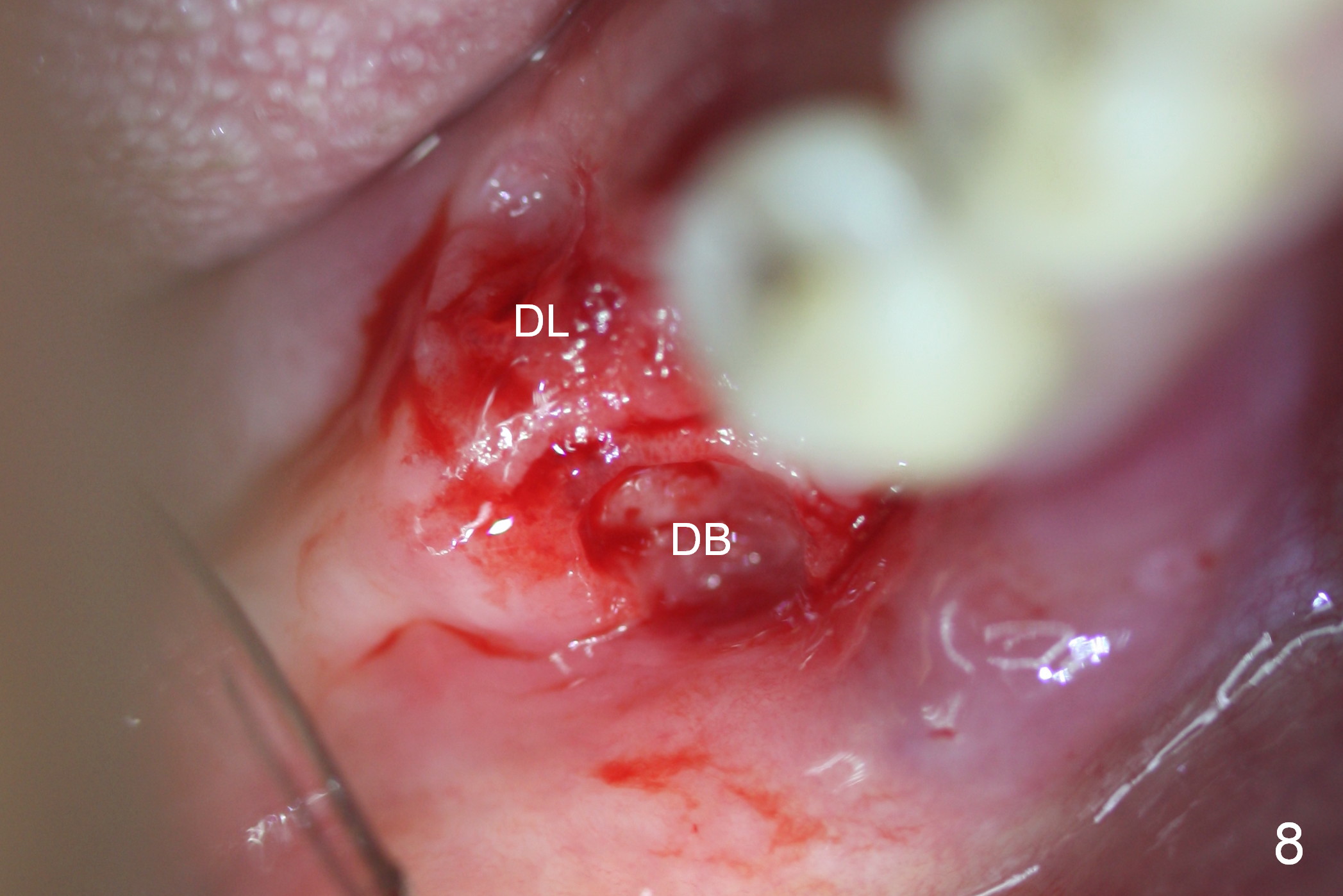
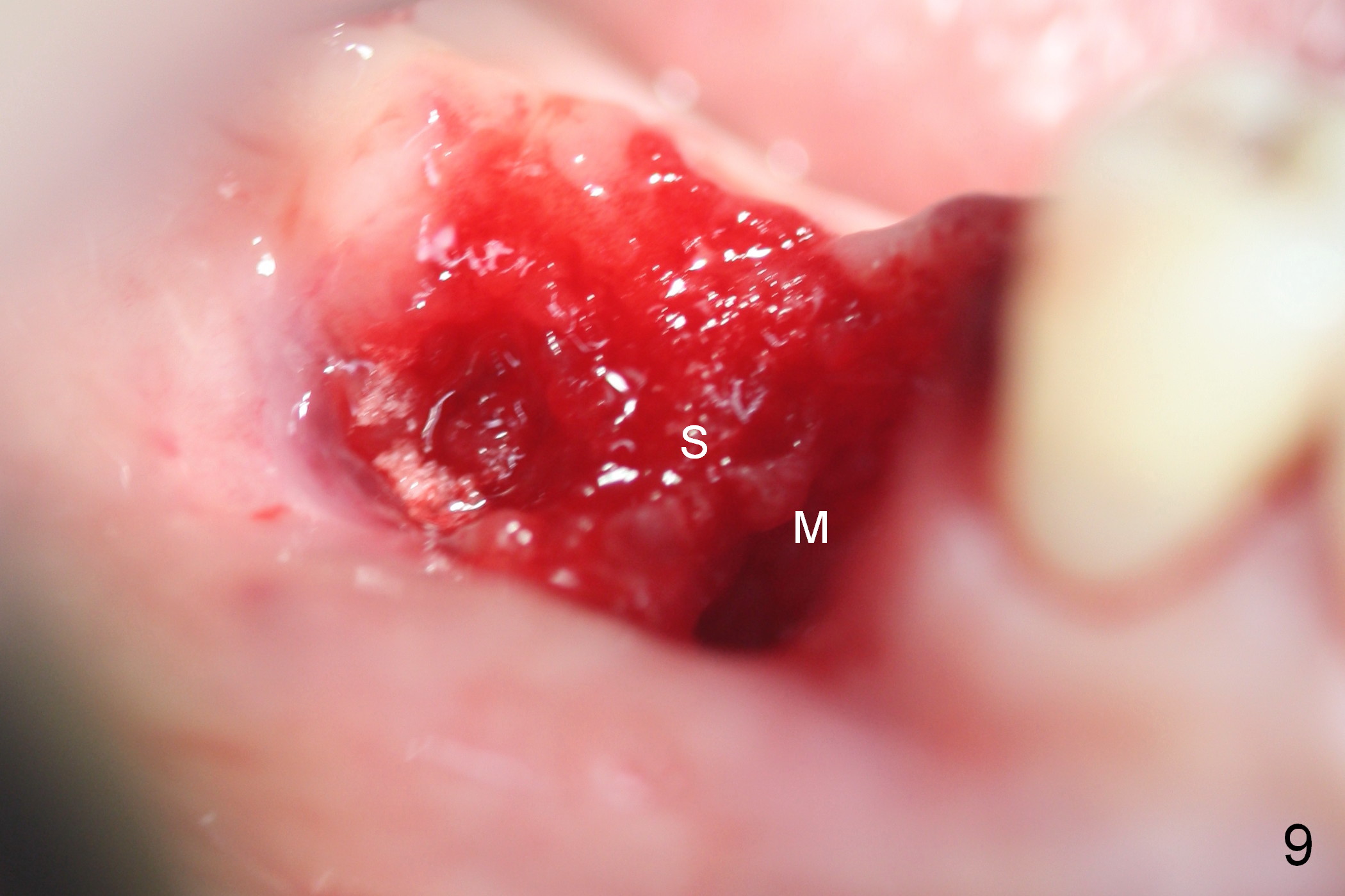
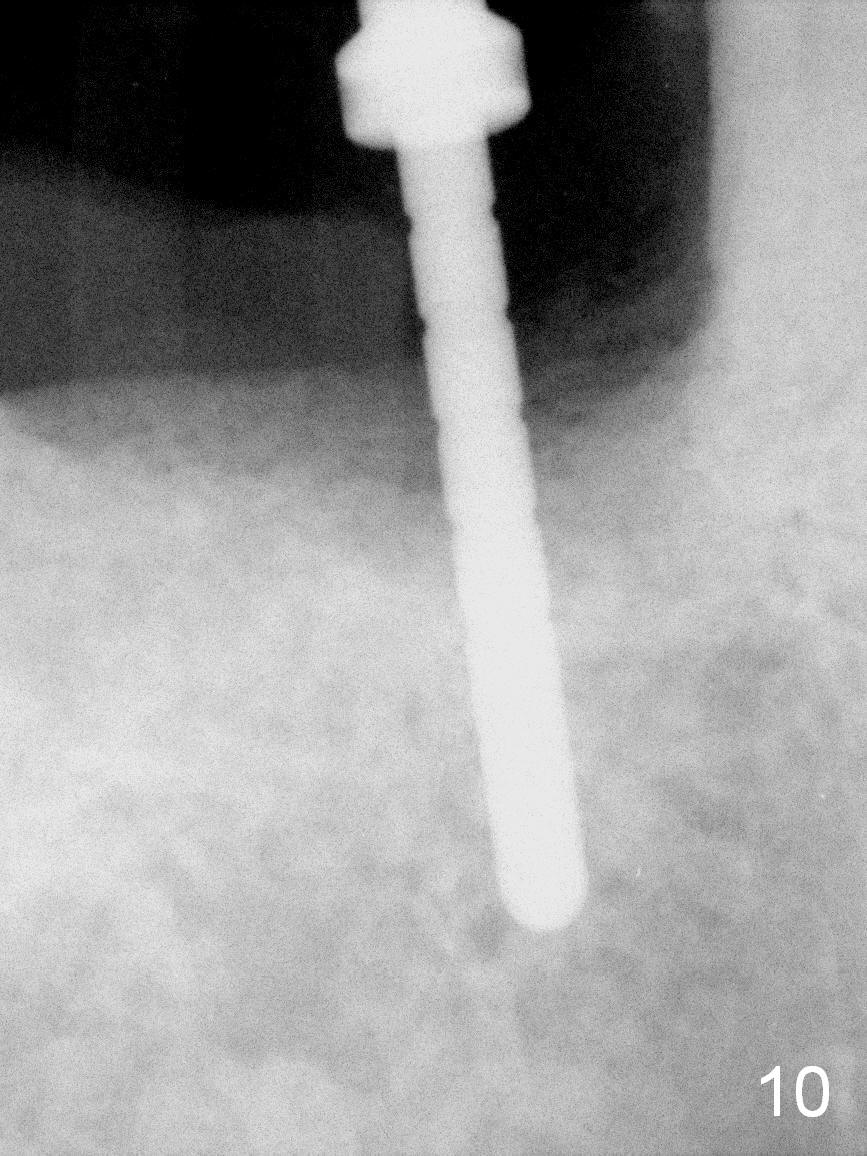
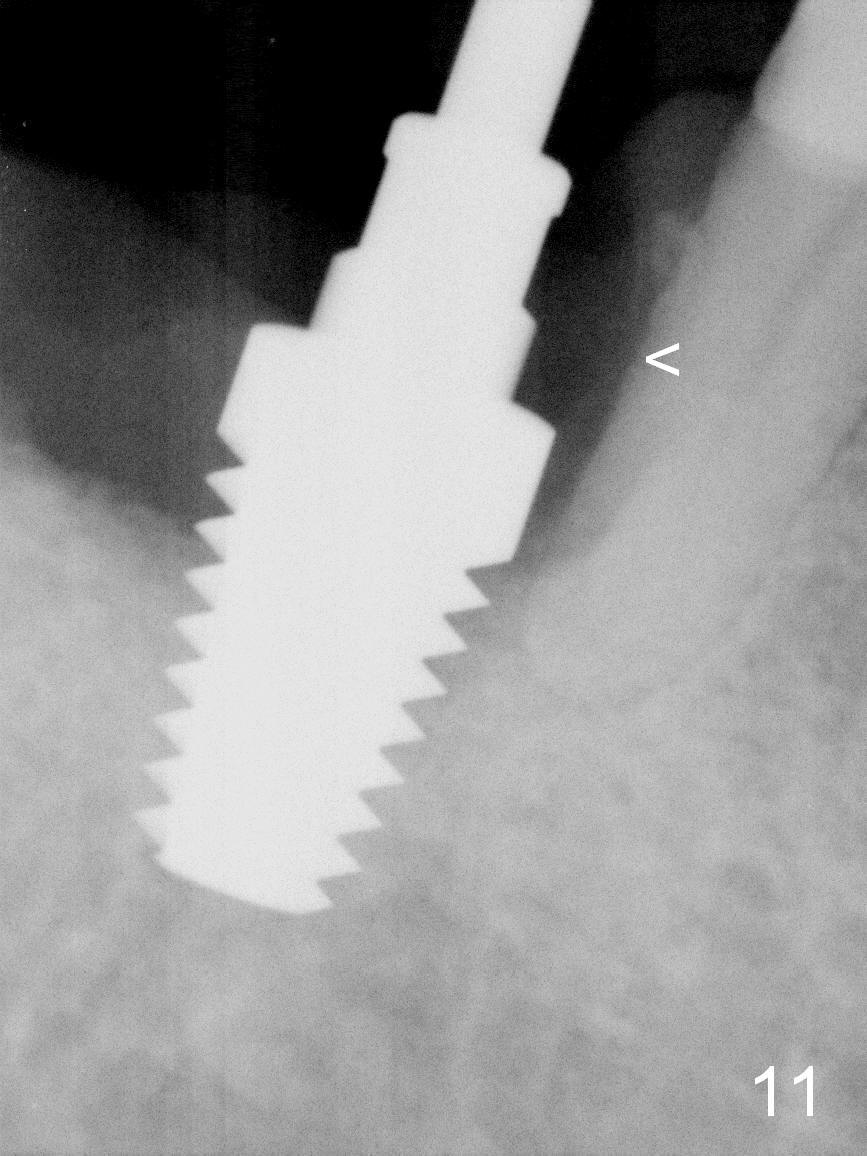
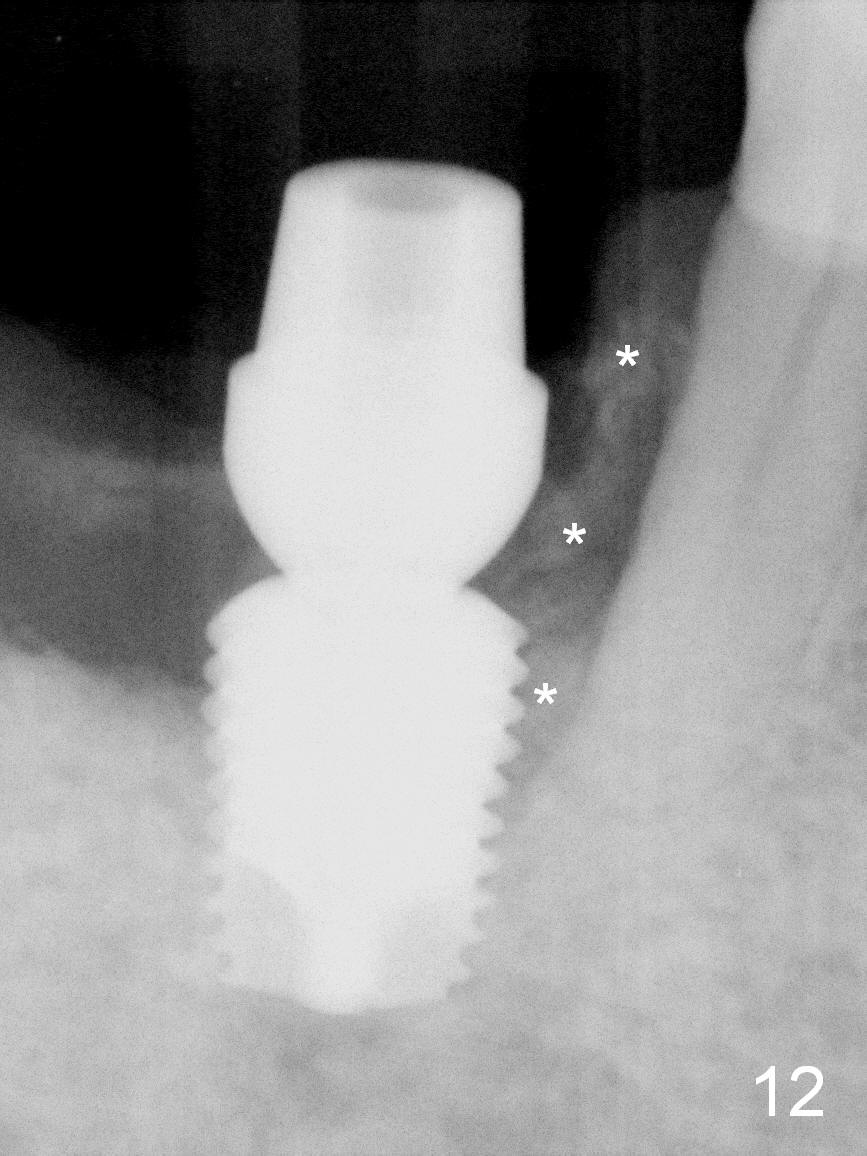
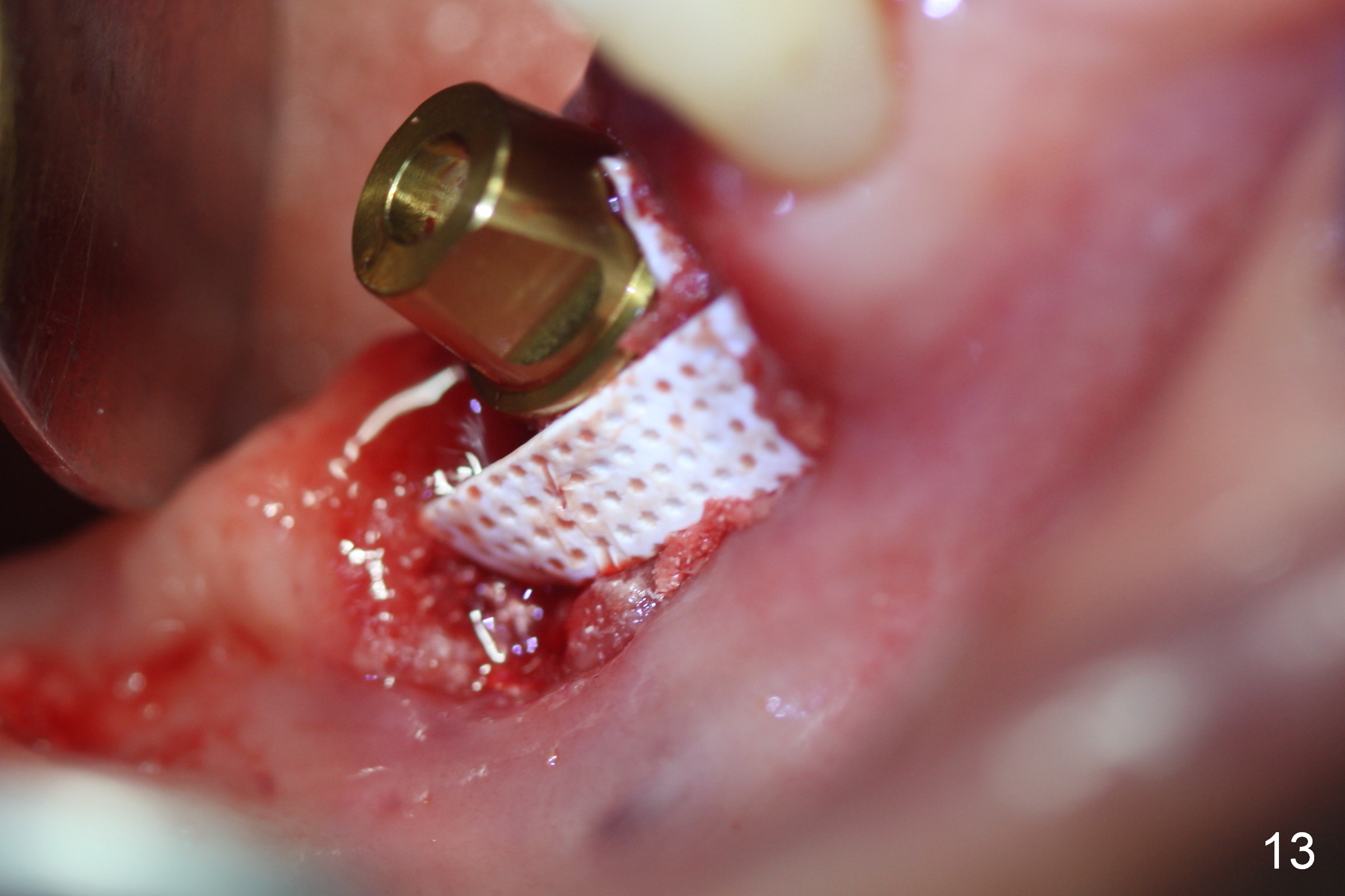
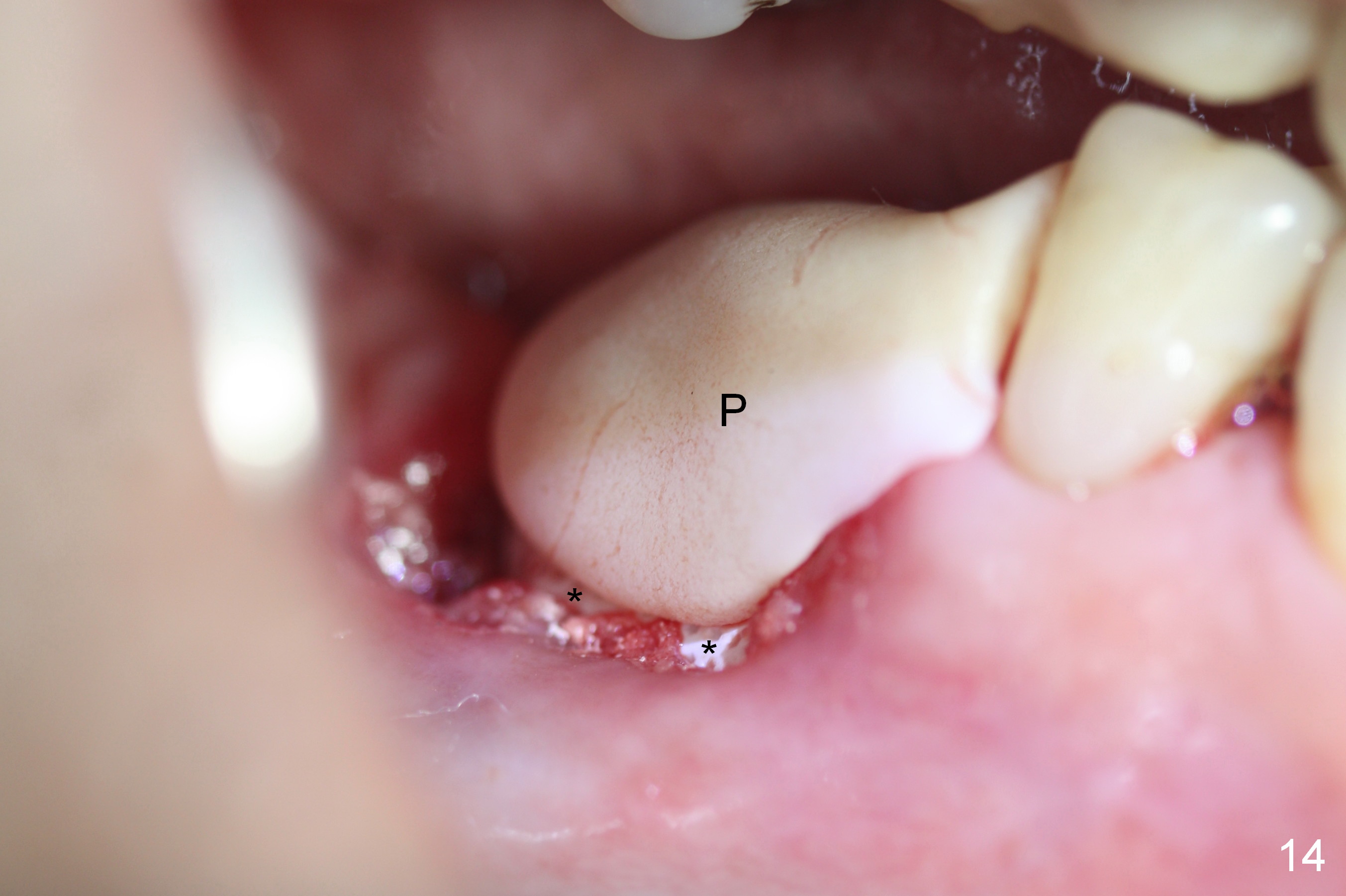
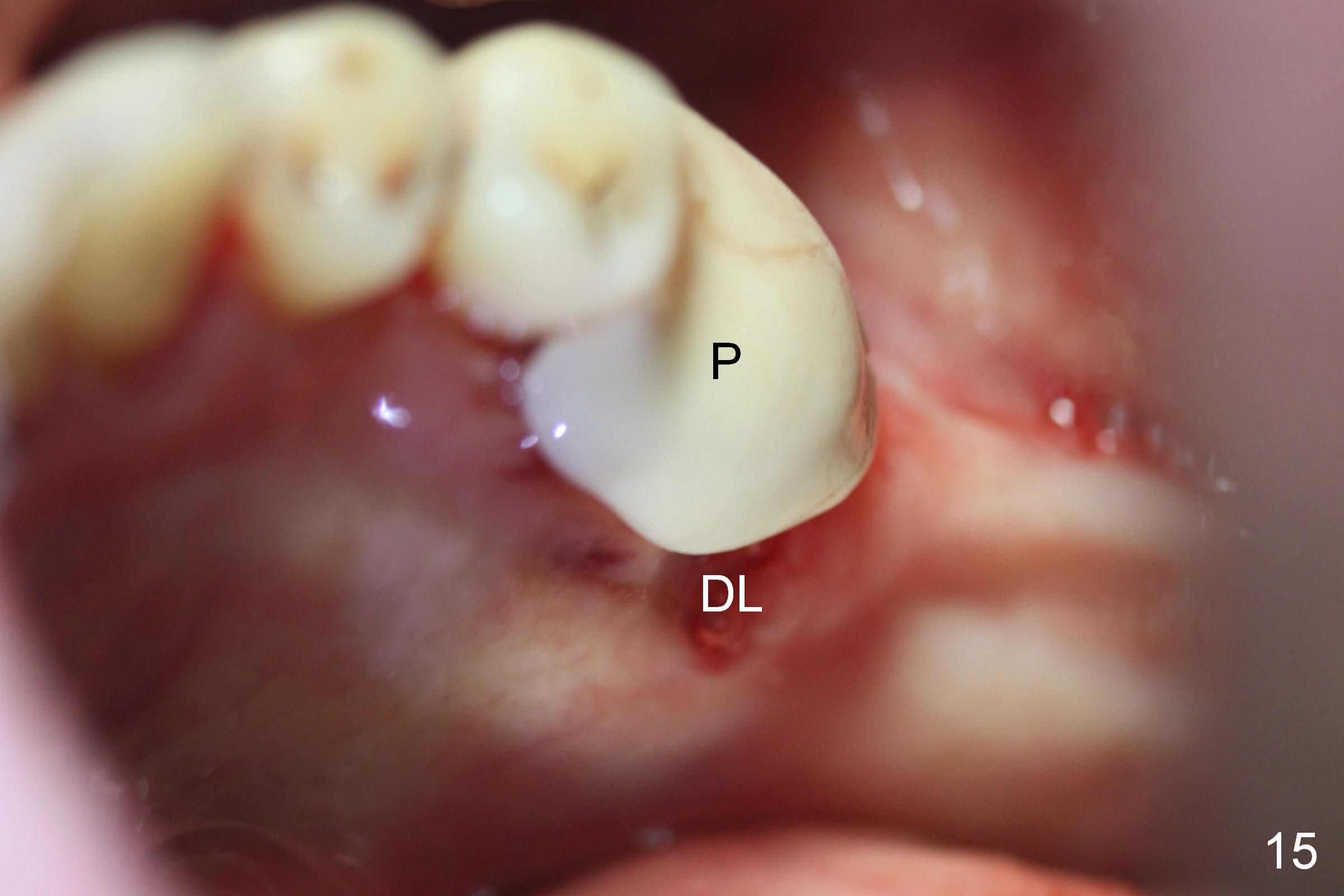
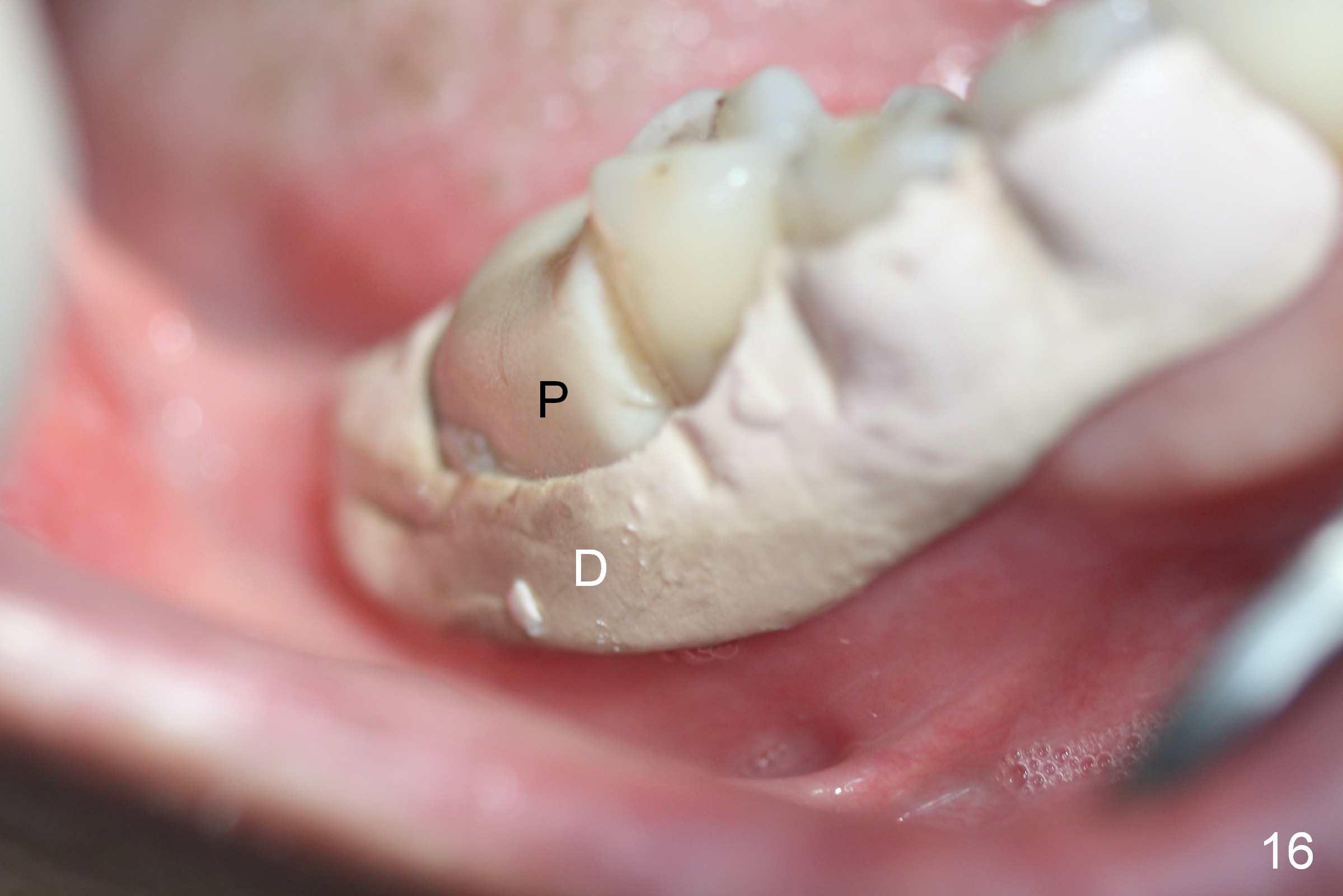
The tooth #30 has severe gingival recession (Fig.1,2): the mesial (M), distobuccal (DB) and distolingual (DL) roots having been exposed, especially the last one (Fig.3). It appears that the mesial socket (lingually) is the best site for implant. Two preop PAs do not show the Inferior Alveolar Canal (Fig.4,5). It appears to be safe to place a 8 mm long implant (Fig.6). Extraction (Fig.7) confirms that the mesial socket, as compared to the distobuccal and distolingual ones, seems to be the most appropriate site for implant (Fig.8,9). The osteotomy starts in the distolingual aspect of the mesial socket (Fig.10 (parallel pin after 2 mm pilot drill). As the osteotomy increases (using drills at 50 RPM) and is expanded (taps), the soft and hard tissue of the septum (Fig.9 S) is being pushed distally. Since the bone density is low, a 7x14 mm tap is used to obtain stability (Fig.11). A 6.9x8 mm implant is placed with insertion torque > 55 Ncm (Fig.12). In fact the buccal and lingual plates are present, near and at the level of the top of implant. The plates are too thin to be shown in X-ray. A 6.8x4(4.5) mm abutment is placed immediately (Fig.12). Cytoplast (a non-resorbable membrane) covers the bone graft (Fig.13). The membrane (Fig.14 *) is fixed in place by an immediate provisional (P). The remaining wound (Fig.14.15) will be covered by perio dressing. In spite of no show of the Inferior Alveolar Canal by X-ray, there is no paresthesia postop. Seven days postop, the patient remains asymptomatic; the provisional (Fig.16 P) and perio dressing (D) stay in place. The latter is planned to be removed another 1-2 weeks later.
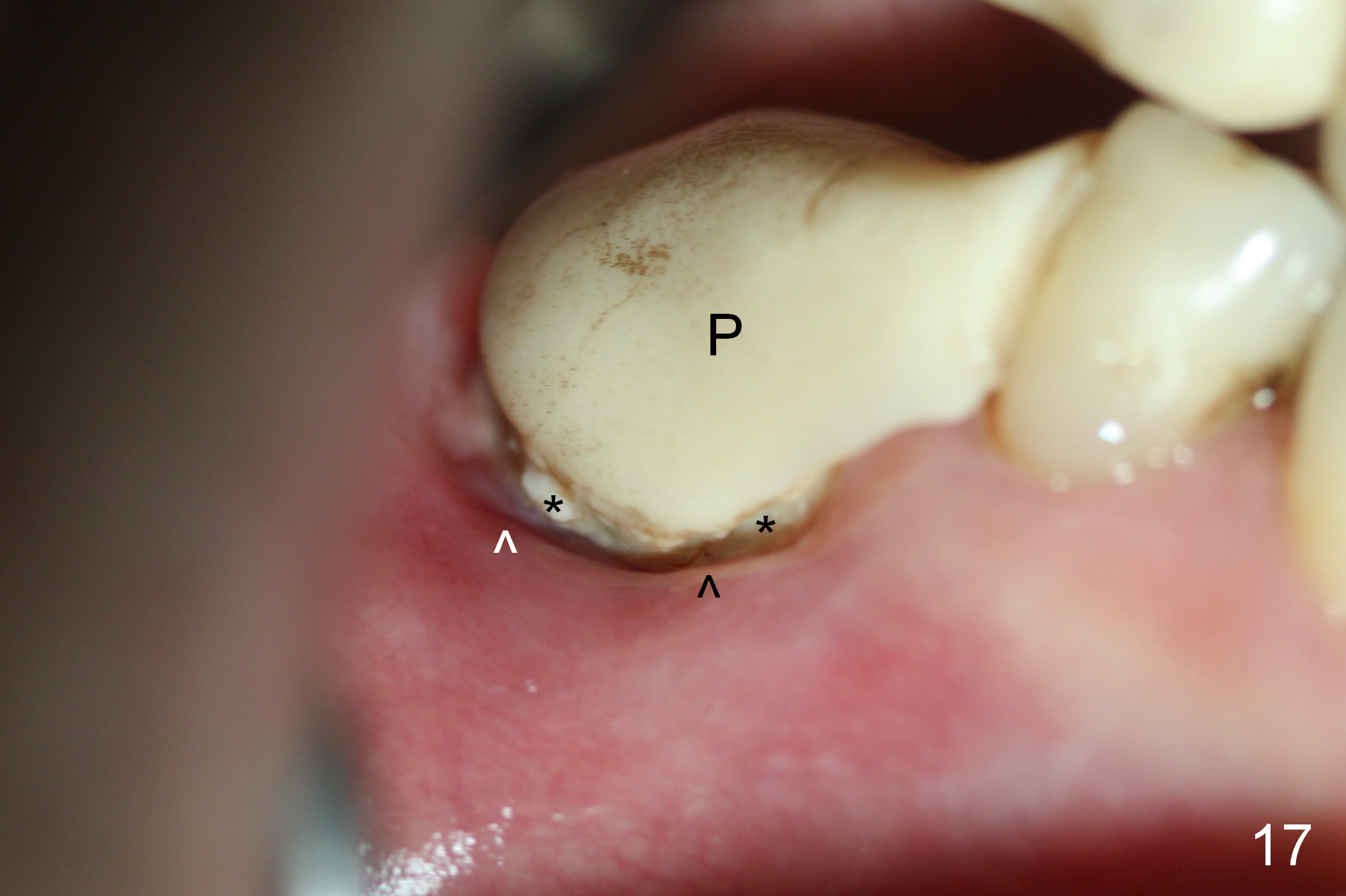
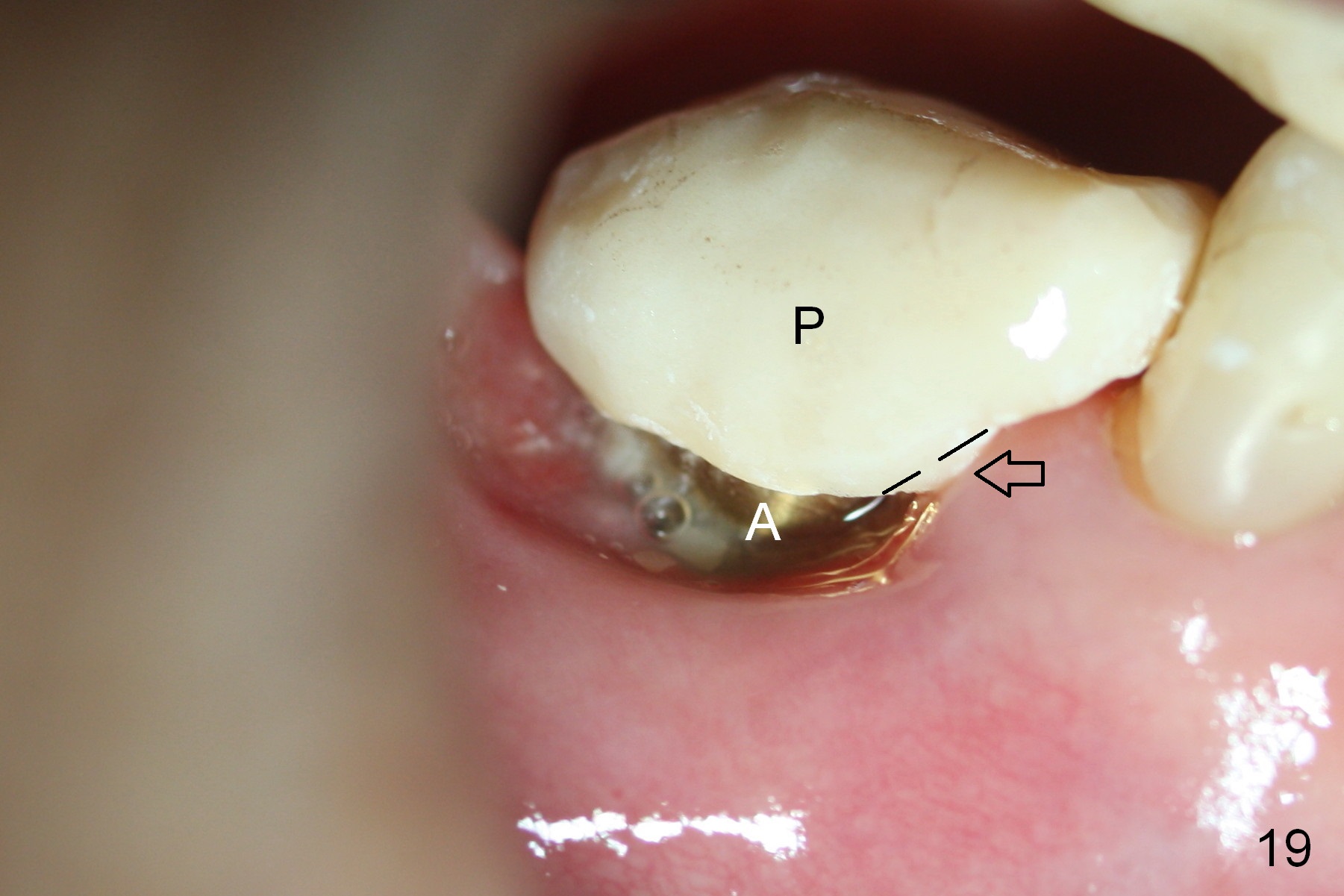
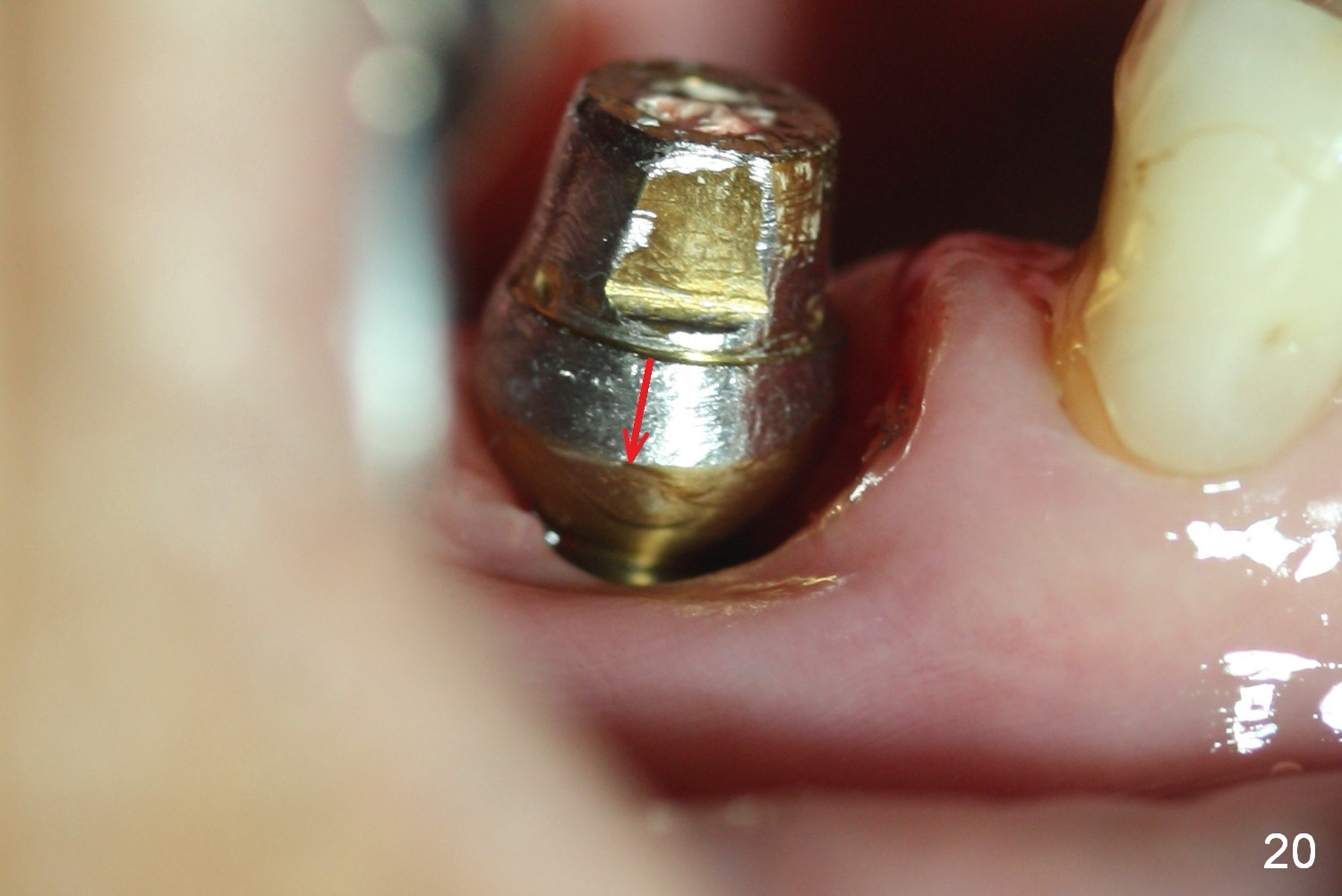
Six to 7 weeks postop, the provisional (Fig.17 P) and Cytoplast (*) remain in place, while the gingival margin appears to grow more superiorly and toward the provisional (^, as compared to Fig.14). When the formers are removed, loose bone graft (Fig.18 *) adheres to the surface of the inferior portion of the abutment (A). After the margin of the provisional (Fig.19 P) is trimmed, the provisional is recemented. It is expected that the gingiva will gradually cover the inferior portion of the abutment (A). Next visit, the mesial margin of the provisional (black dashed line) will be trimmed so that the keratinized gingiva can grow toward the abutment (arrow). Eighteen days later, the abutment margin is lowered (Fig.20 arrow) before provisional modification as mentioned above. The coronal end of the implant is not covered (Fig.21 *), but without sign or symptom of infection. Retrospectively, the gingival recession should have been repaired with tissue graft.
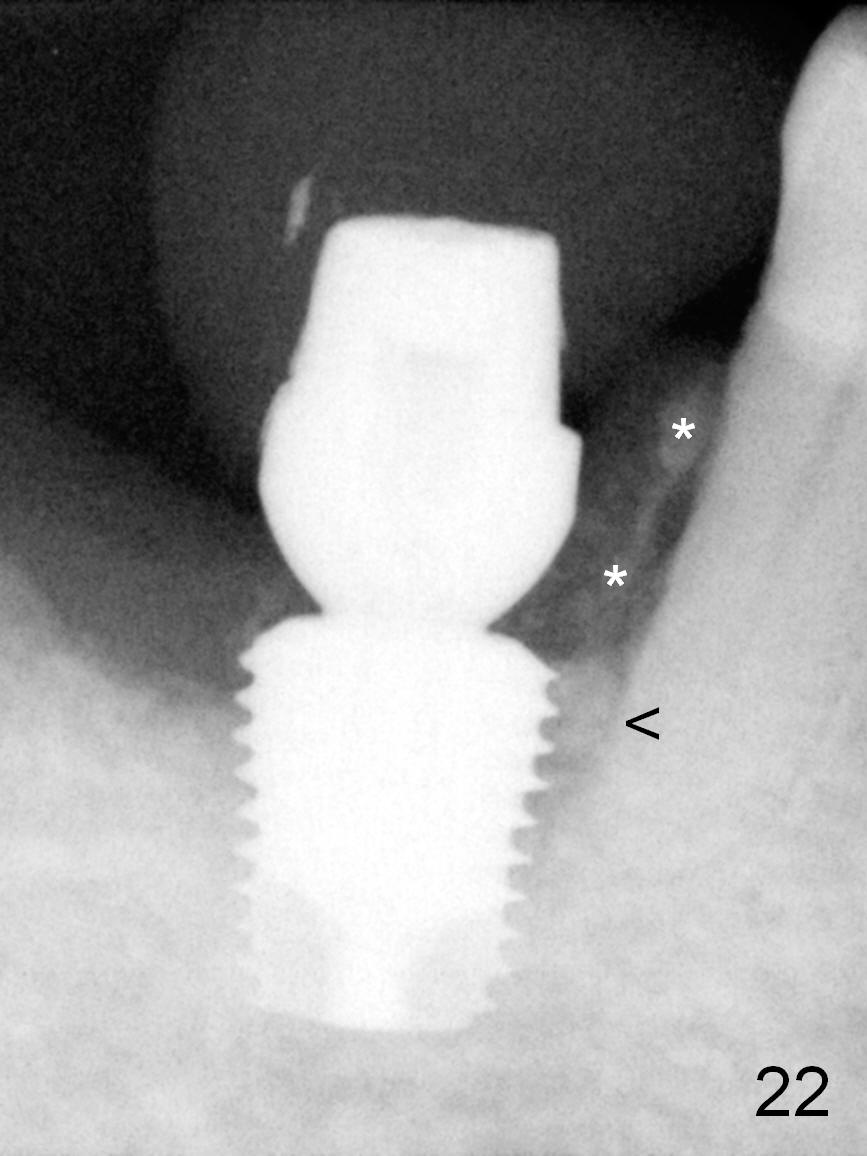
The patient returns for impression of final restoration 3.5 months postop (1/2 half since last visit). Bone graft is continuously visible along the root of the neighboring tooth (Fig.22 *) and between the implant and the root (<).
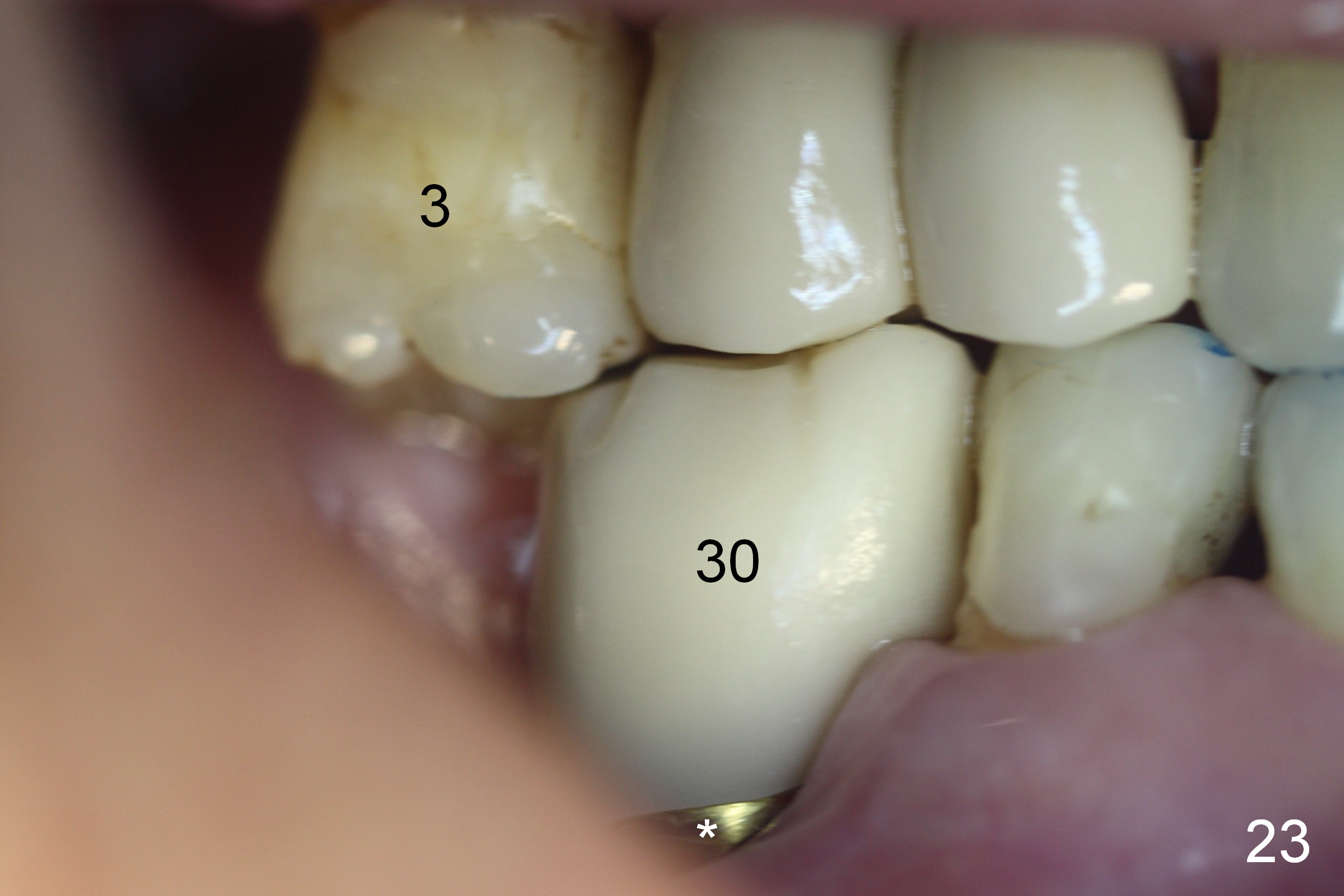
When the crown is cemented (nearly 5 months postop), the gingiva surrounding the abutment (Fig.23 *) remains healthy. It appears that an implant at #31 is needed for maximal intercuspidation.
There is no bone resorption 8 months post cementation (Fig.24). The large diameter implant compensates for unfavorable crown/implant ratio. In fact there is no gingival recession, in contrast to Fig.23.
Return to Lower Molar Immediate Implant,
Posterior Immediate Provisional
Xin Wei, DDS, PhD, MS 1st edition 08/20/2015, last revision 08/14/2016