
|
|
|
|
|
|
|
|
|
|
|
Thin Septum
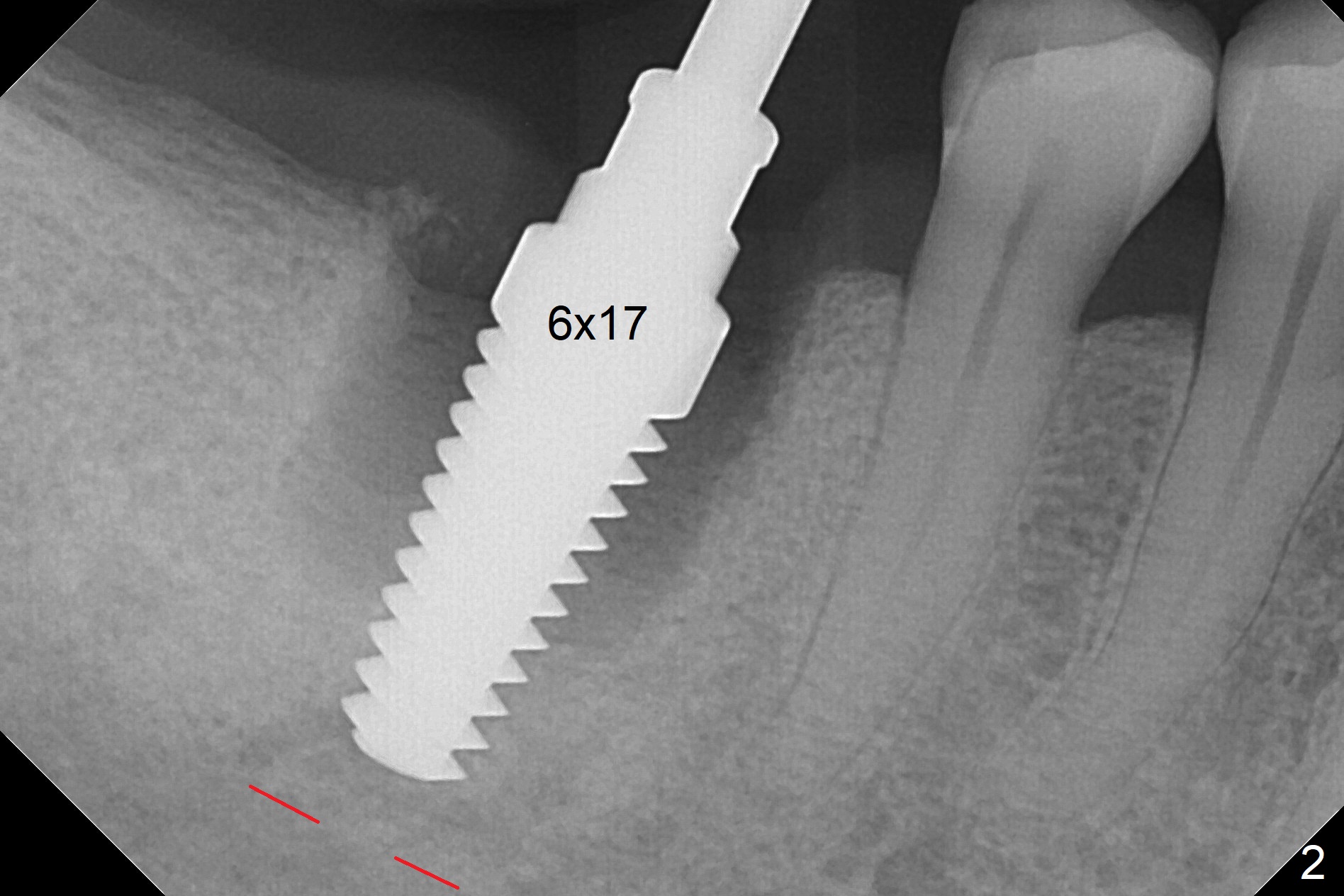
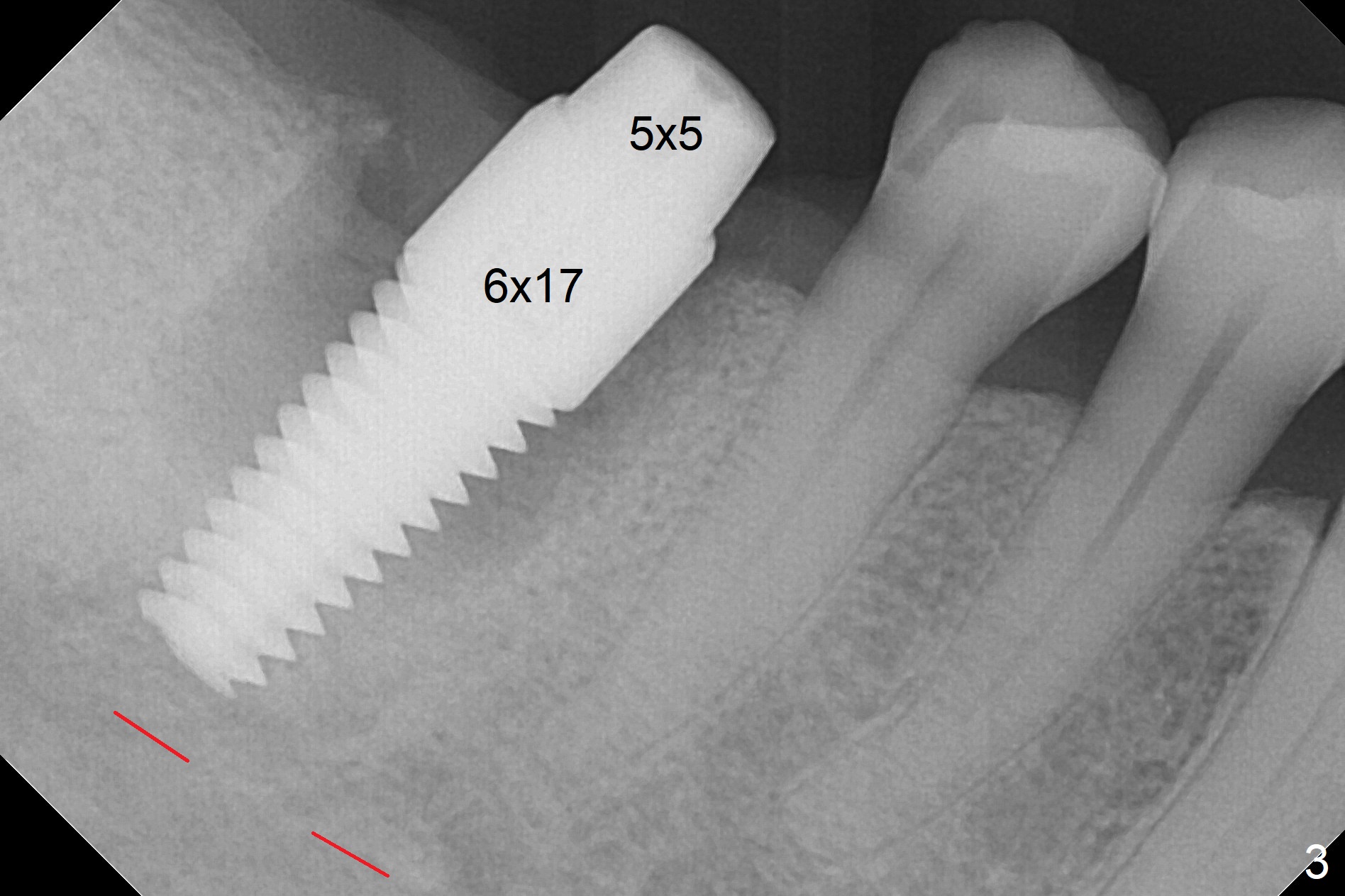
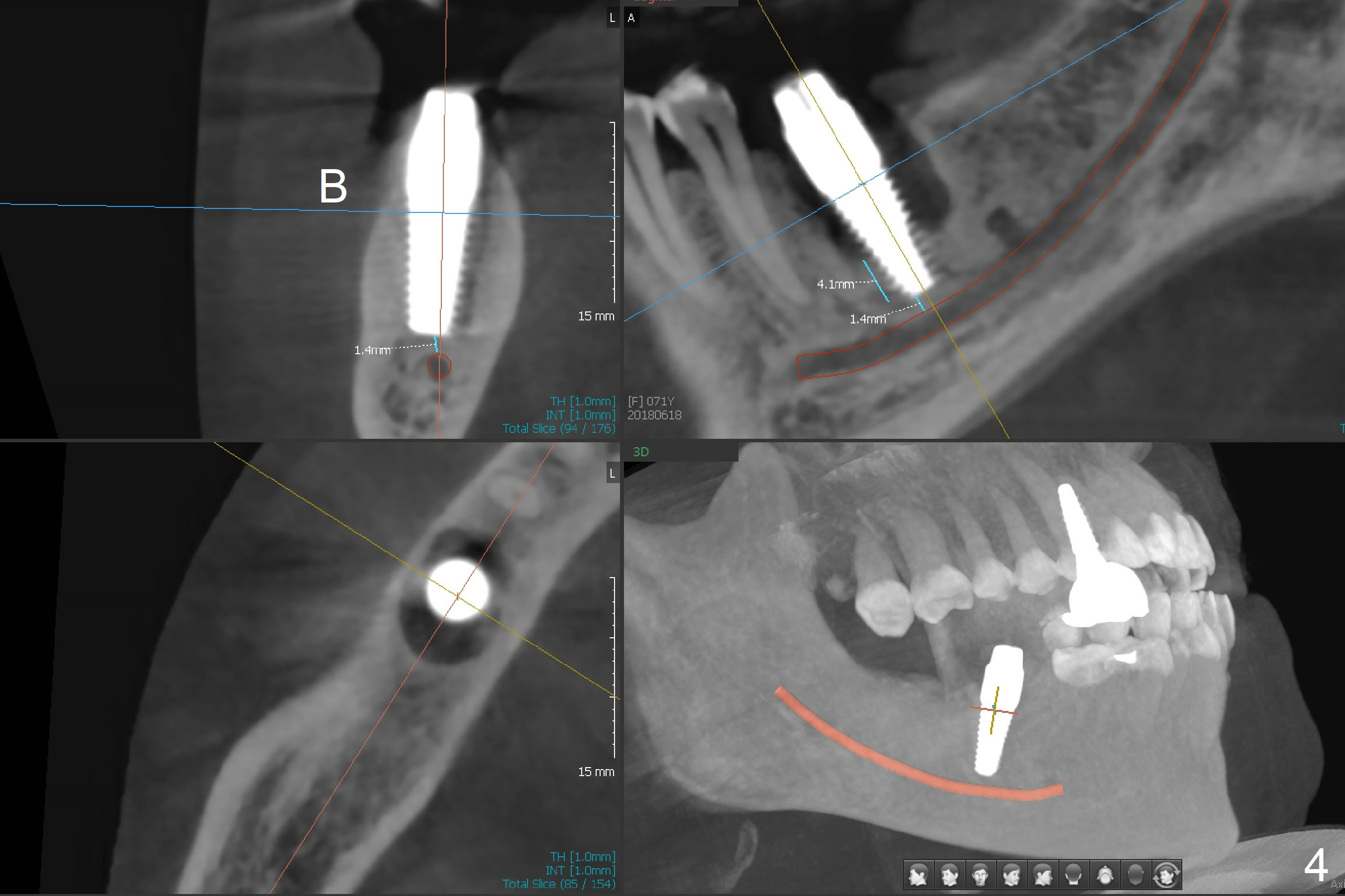
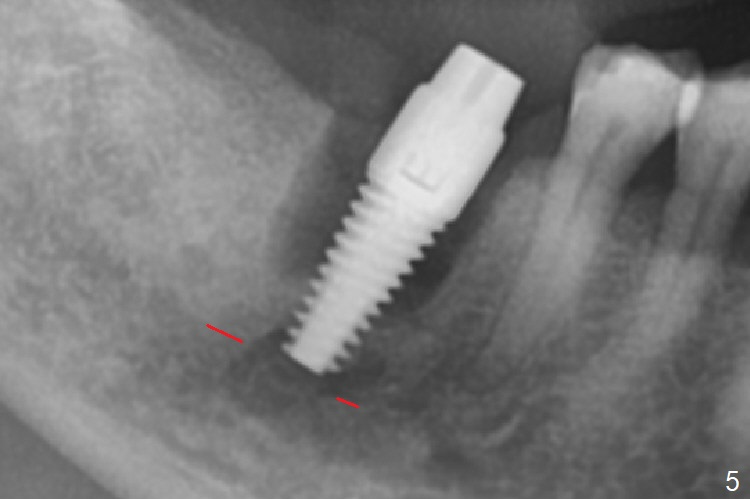
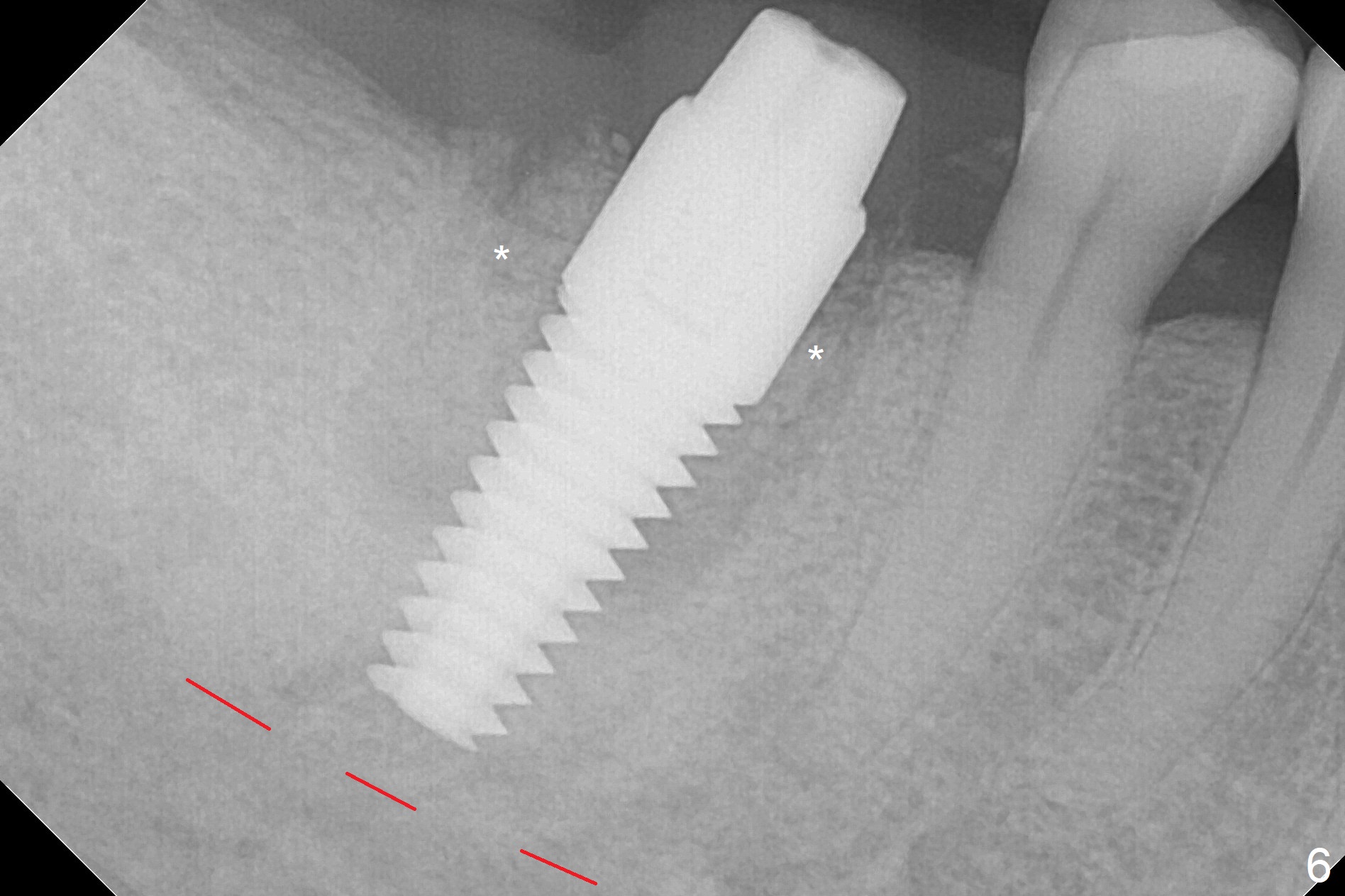
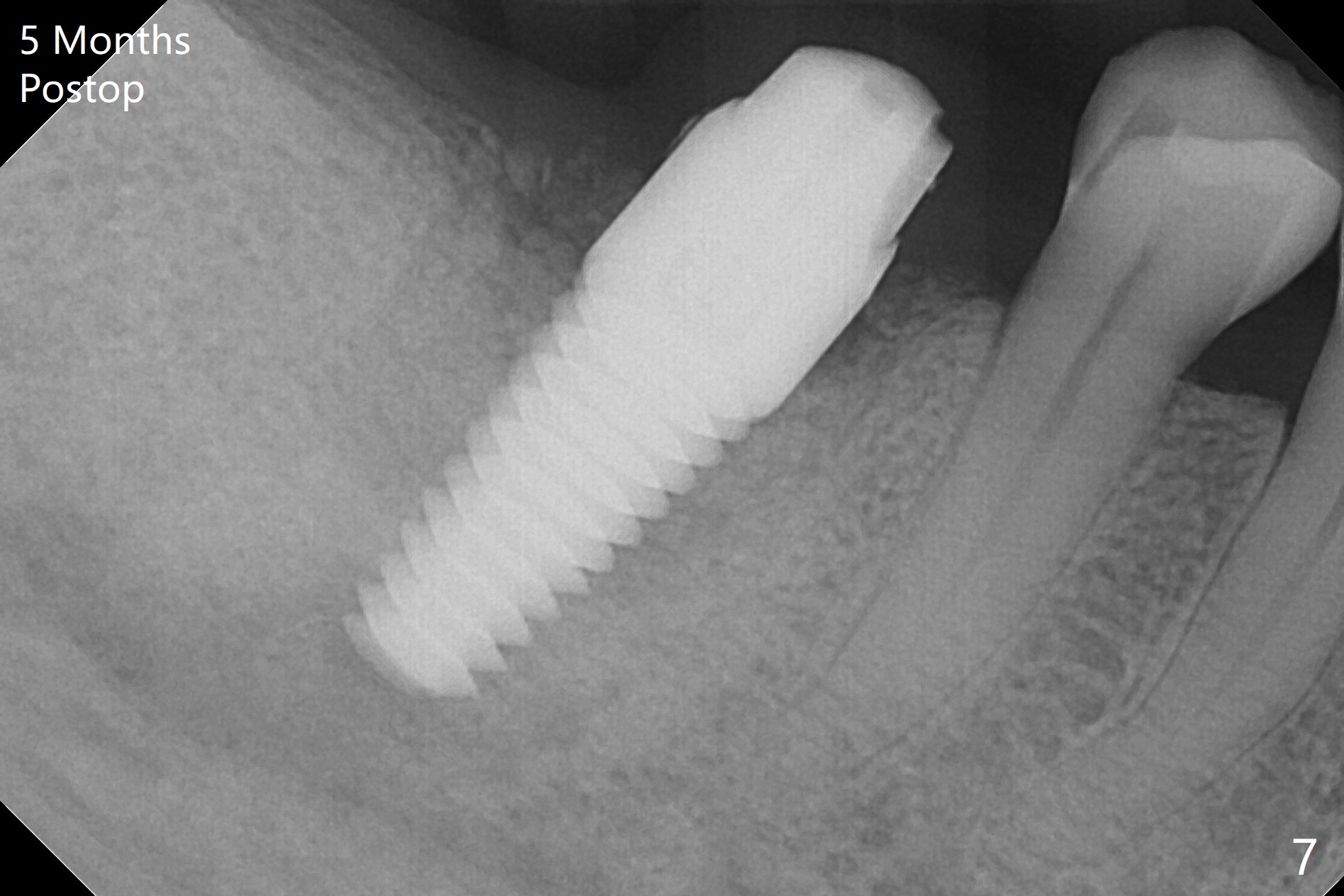
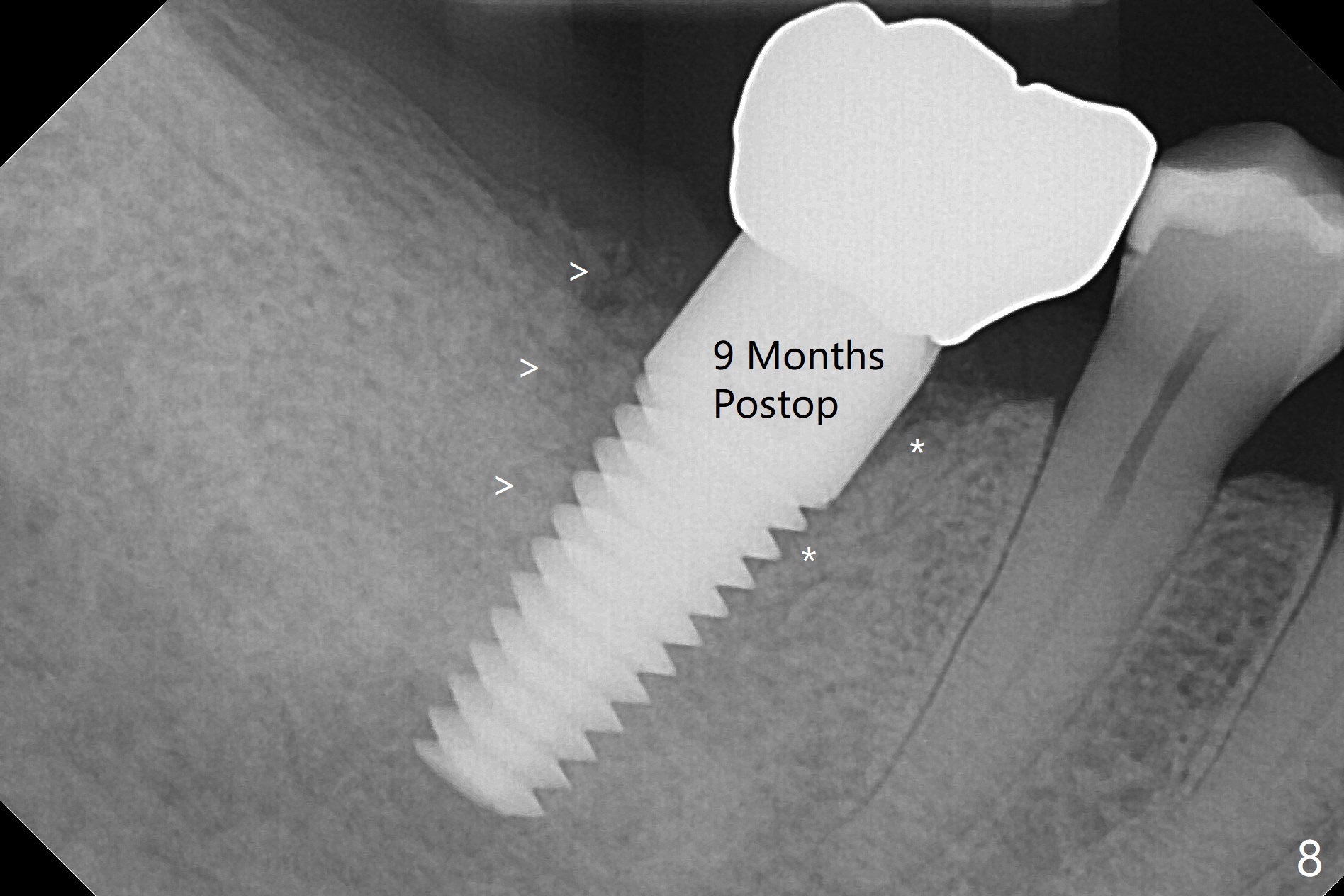
After extraction of the tooth #30 and curettage, the septum becomes so thin that the most coronal portion has to be removed with Rongeur and surgical fissure bur (bone height reduction). Initial osteotomy depth is ~ 4 mm from the flattened septum (Fig.1 (yellow dashed line: apical end of the osteotomy)). Following sequential osteotomy (with intact osteotomy wall), a 6x17 mm tap is placed with apparent clearance from the Inferior Alveolar Canal (Fig.2). When the same size implant is placed with 60 Ncm (Fig.3), the nervous patient feels that the implant is too long (causing pain). CT (Fig.4) and panoramic X-ray (Fig.5) show limited clearance (1.4 mm), but compression of the canal due to high torque could not be ruled out. Since limited amount of the native bone (4.1 mm) for primary stability, the implant is not backed up immediately. Vanilla graft is placed after fabrication of an immediate provisional (Fig.6 *). In brief, immediate implant should be avoided when the septum is thin or the native bone is less than 5 mm (3 mm for primary stability; 2 mm for clearance). In fact the implant has to be untorqued 4-5 times of turn to relieve pain nearly 1 month postop. The patient returns for impression 5 months postop (4 months post implant back up, Fig.7). When the abutment is changed to 5x5 mm and prepared, she reports earache (residual nerve damage?). The patient has had the similar complaint 9 months postop; it appears that there is radiolucency distally (Fig.8 >, as compared to radiopaque mesially (*)). The distal gingiva is tender. With a remade permanent crown, oral hygiene instruction is provided. If necessary, CBCT is taken with possible bone graft.
Return to Lower Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), Armaments 14 Xin Wei, DDS, PhD, MS 1st edition 06/18/2018, last revision 05/20/2019