
|
|
|
|
|
|
Implant and Intrusion
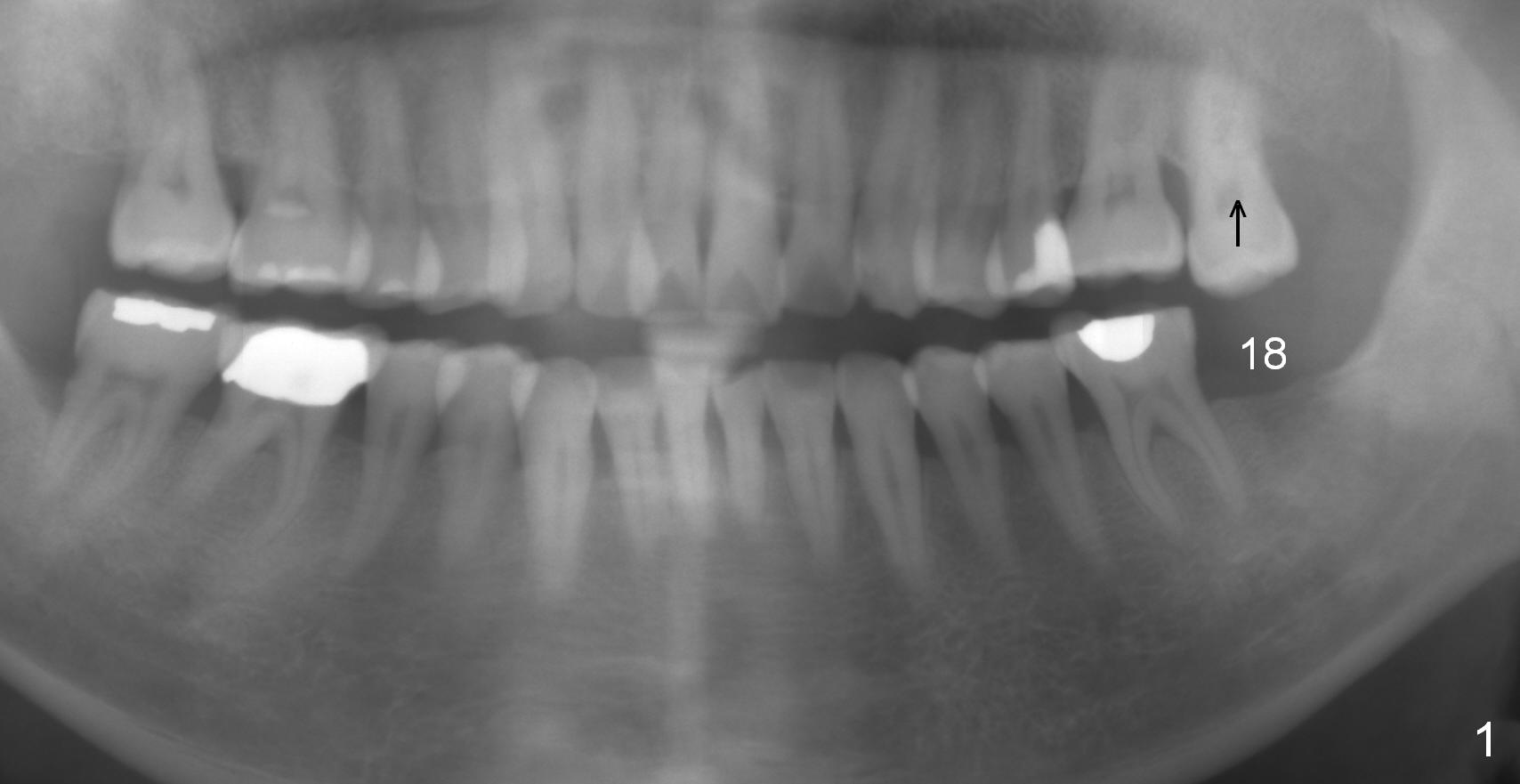
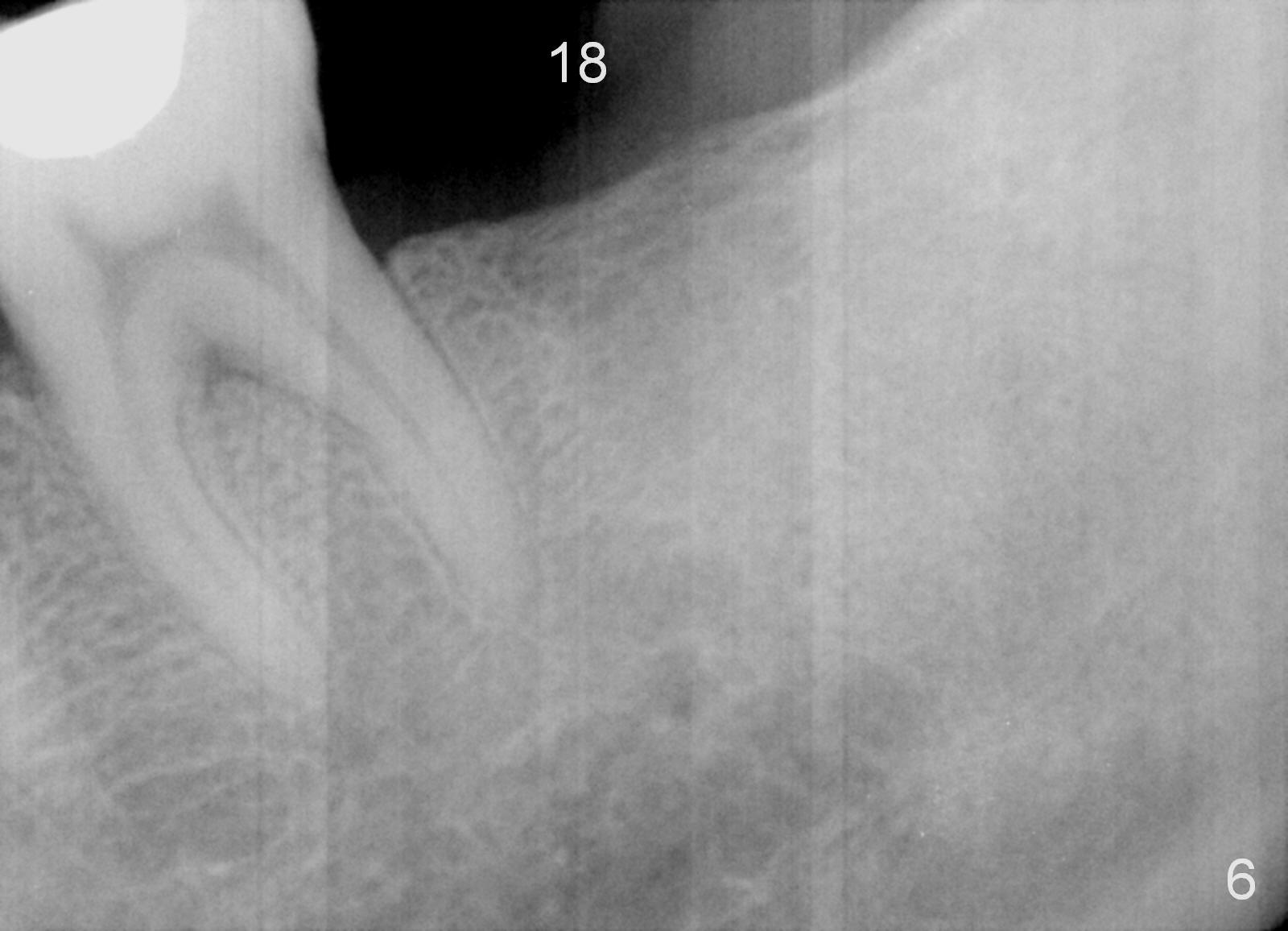
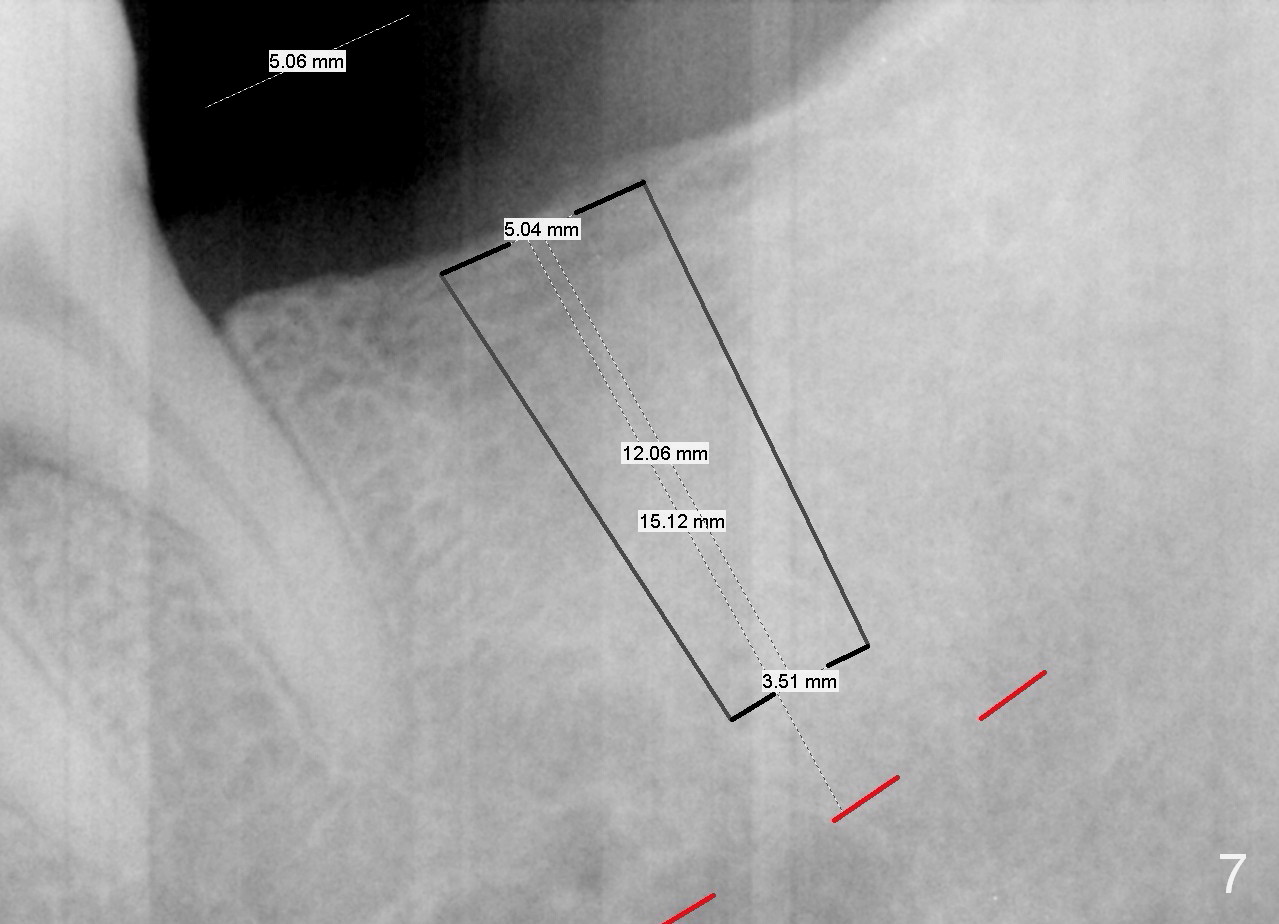
A 51-year-old man has lost #18 for more than 10 years (Fig.1,6). There appears to be sufficient bone height for implant (15 mm (Fig.7 (red dashed line: the superior border of the Inferior Alveolar Canal))). Prepare 4 mm implant spacer and SM starter drill and 2 mm pilot drill at 12 mm. Take PA. Palpation reveals that the edentulous ridge is wide. Place an implant in the middle of the ridge (buccolingually).
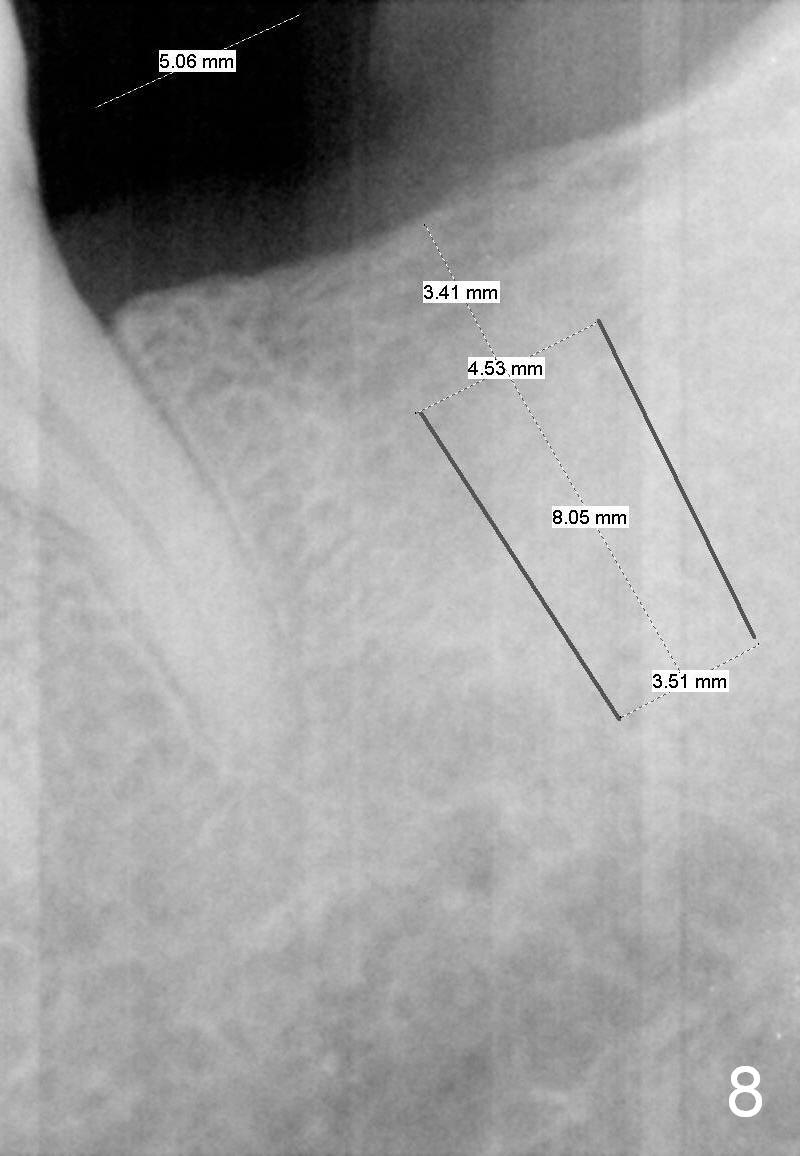
On second thought, Bicon implant is to be placed, either 4.5x8 or 5x6 mm (Fig.8).
Next appointment, place 2 of mini-implants for #15 intrusion (Fig.1 arrow): one in MB (latch driver) and the other in DL (hand instrument).
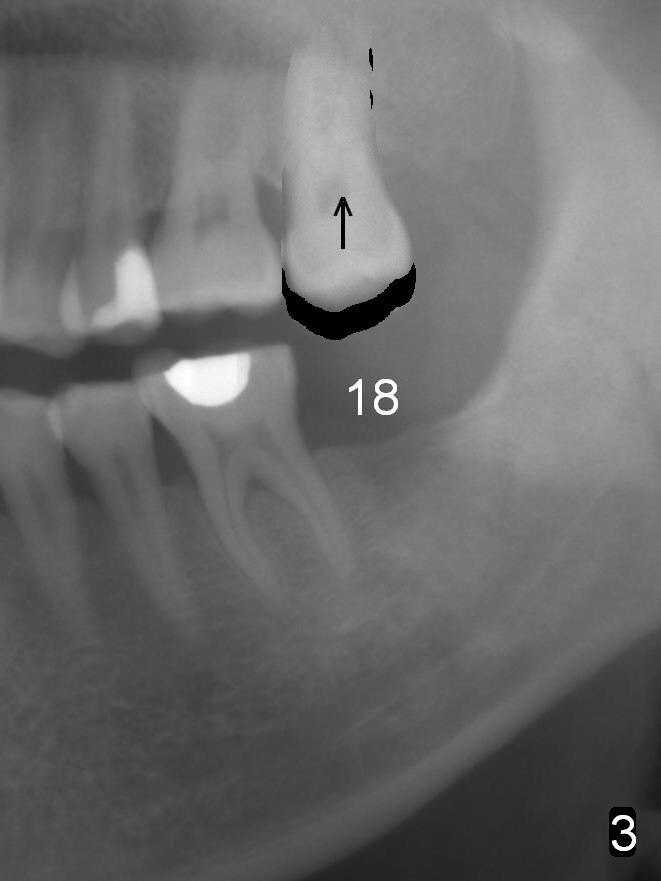
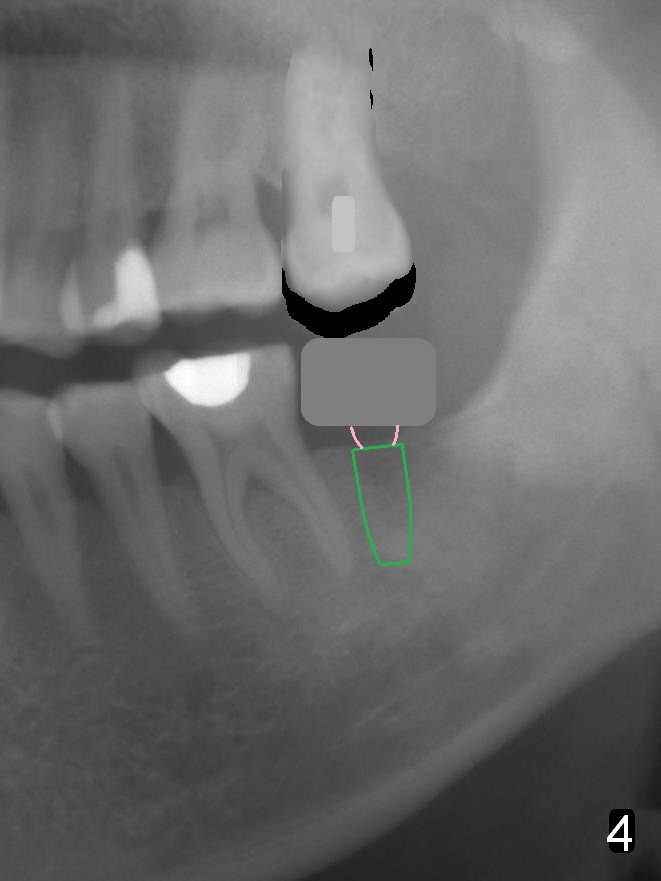
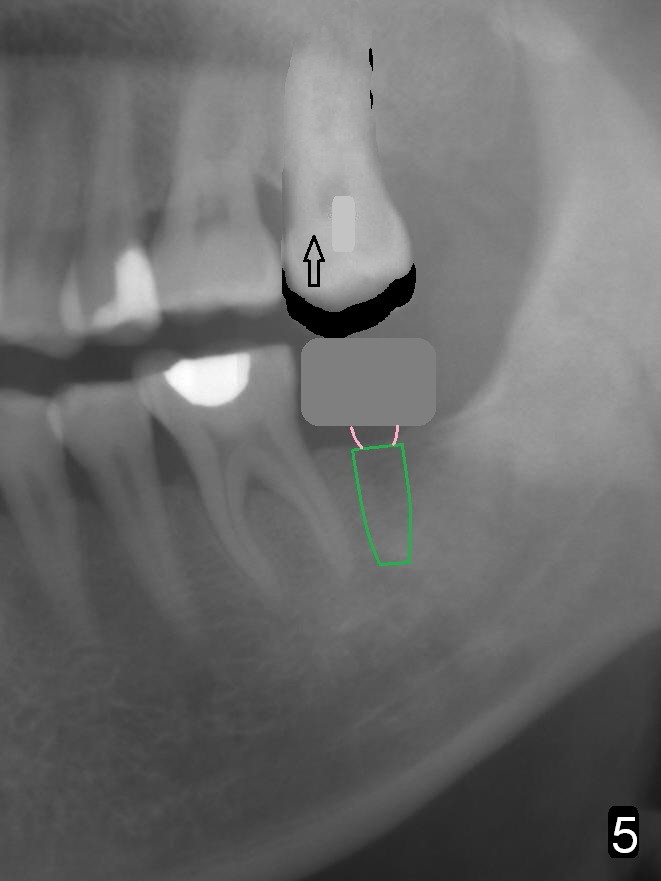
In fact, the tooth 15 had basically no extrusion 6 years earlier (Fig.2) with even occlusal plane. When the tooth is intruded orthodontically, the occlusal plane may be not even (Fig.3). When the implant at #18 osteointegrates (Fig.4 green), fabricate a provisional (grey rectangle) with higher mesial occlusal surface. For certain period of time, the tooth #15 may change its axis so that the mesial portion of the tooth may be intruded more (Fig.5 arrow).
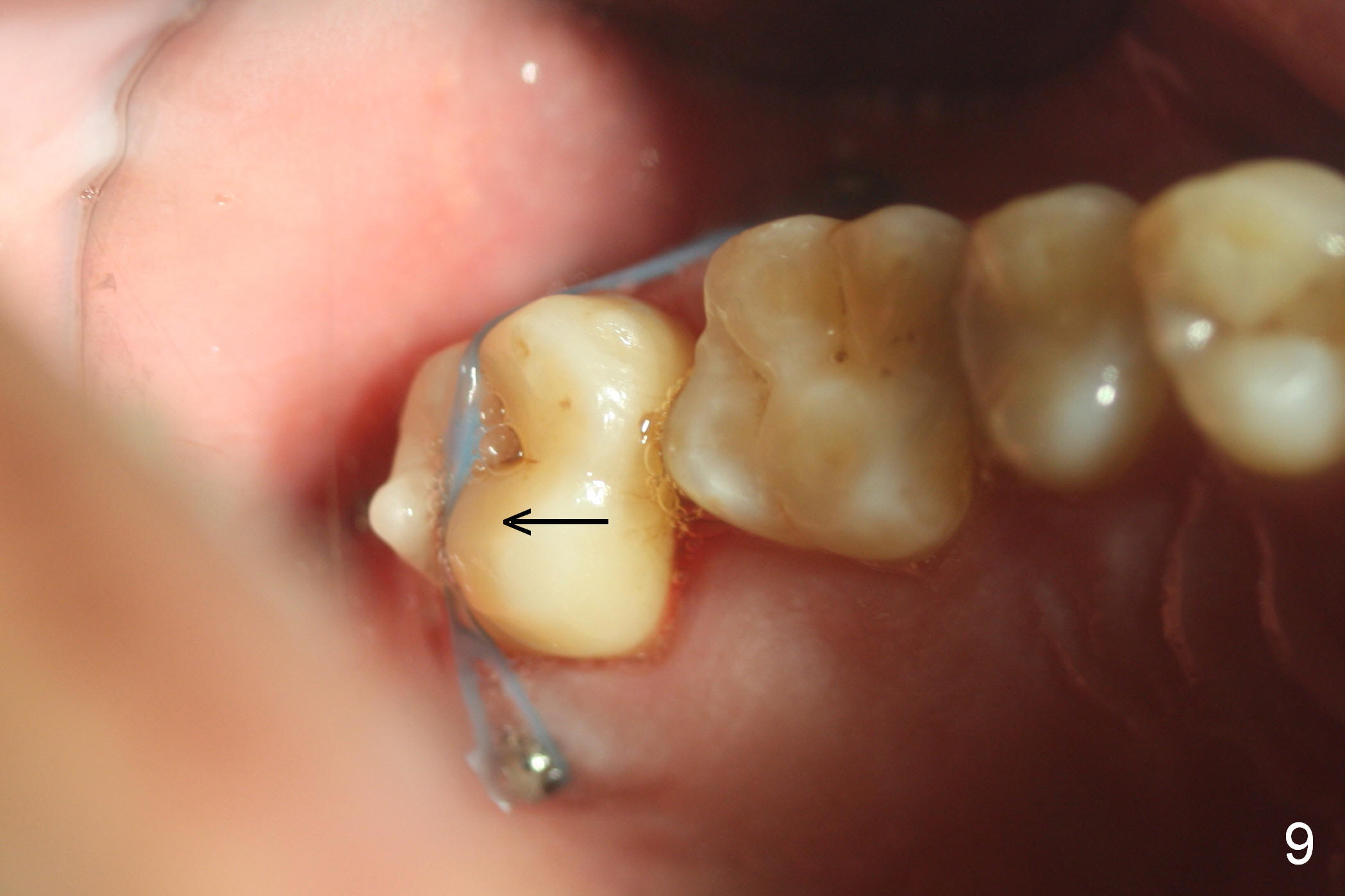
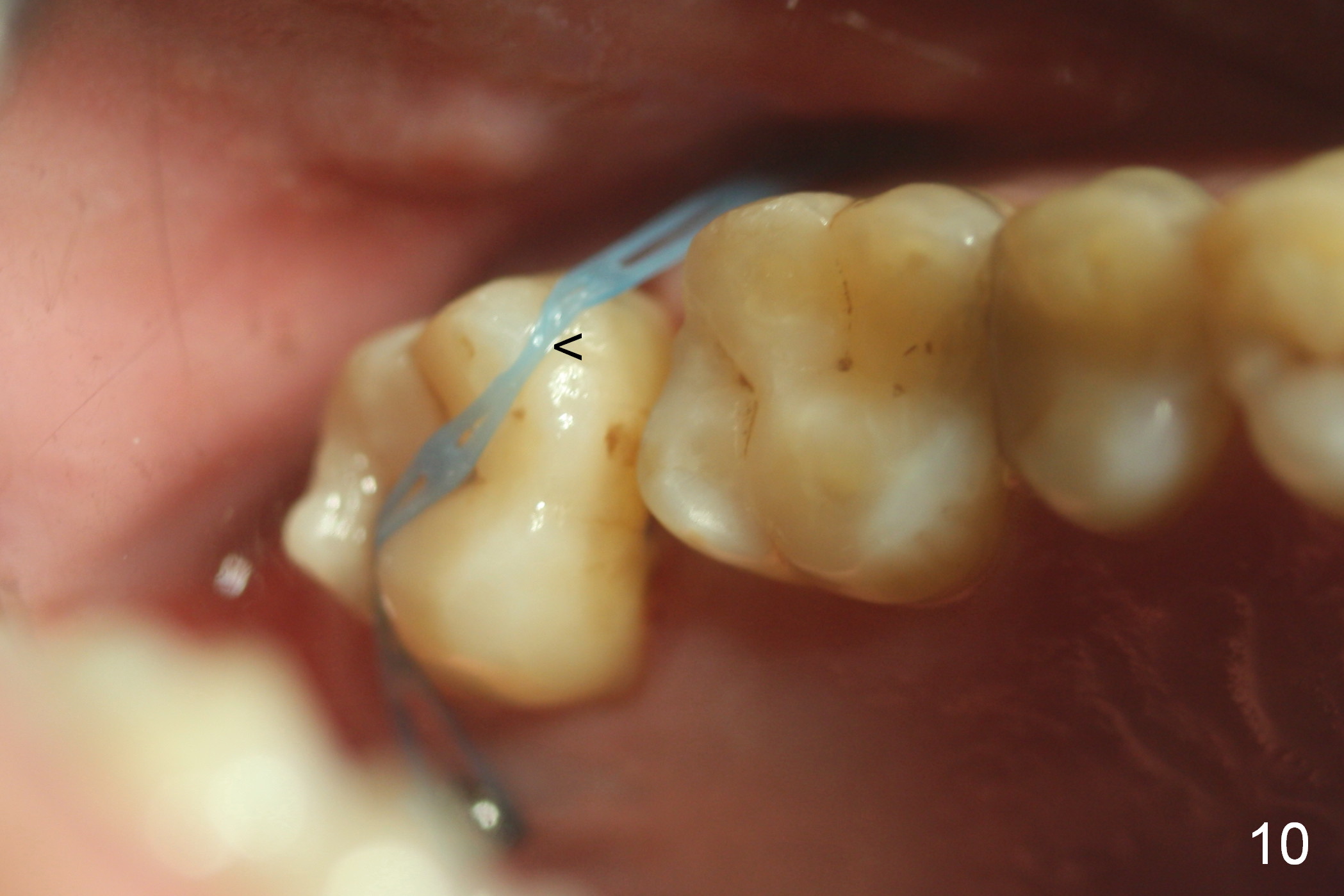
Four months post intrusion, the tooth #15 is distalized instead (Fig.9 arrow). To facilitate mesialization, the power chain is engaged into the mesiobuccal slot (Fig.10 <). It is 1 month after the change in position of the power chain. Has the tooth mesialized? Regional orthodontic devices are placed, but the patient is not cooperative, refusing any intrusion treatment. Prosthetic intrusion will be tried once the implant at #18 osteointegrates.
Return to Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 11/21/2015, last revision 01/19/2018