
.jpg)
,%206x9,%206x4(4).jpg)



|
|
|
|
|
|
|
|
|
|
|
|
Implant Placed in Distal Socket of 2nd Lower Molar
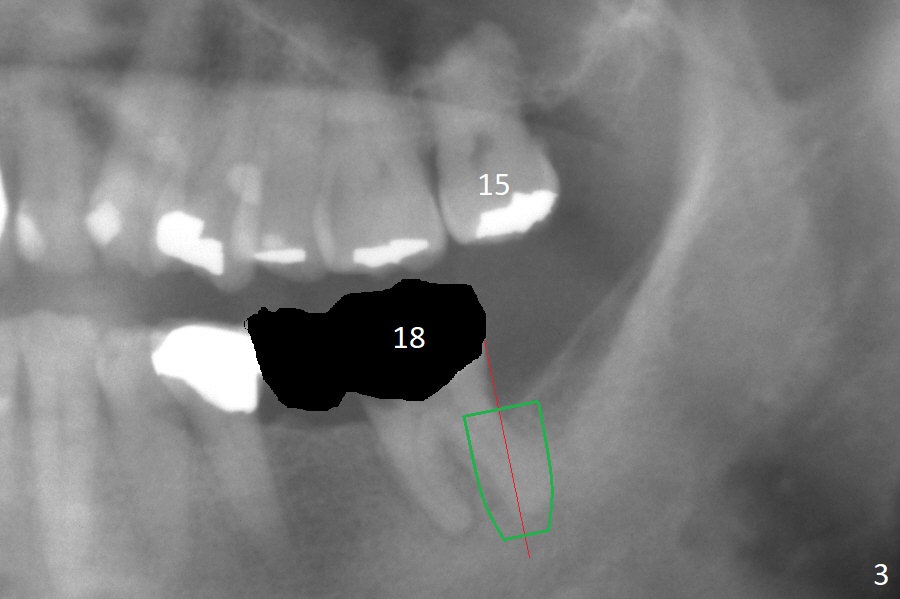
After extraction of the residual root at #18 (Fig.1), the septum is narrow, while the distal socket seems to be the most appropriate site for implant placement (Fig.2 (M: mesial)). In fact the implant needs to tilt slightly distally (relative to the original trajectory of the distal socket, Fig.3 green) to occlude with the opposing tooth. The implant at #19 could be placed more mesially (Fig.4 (*: Vera Graft)).
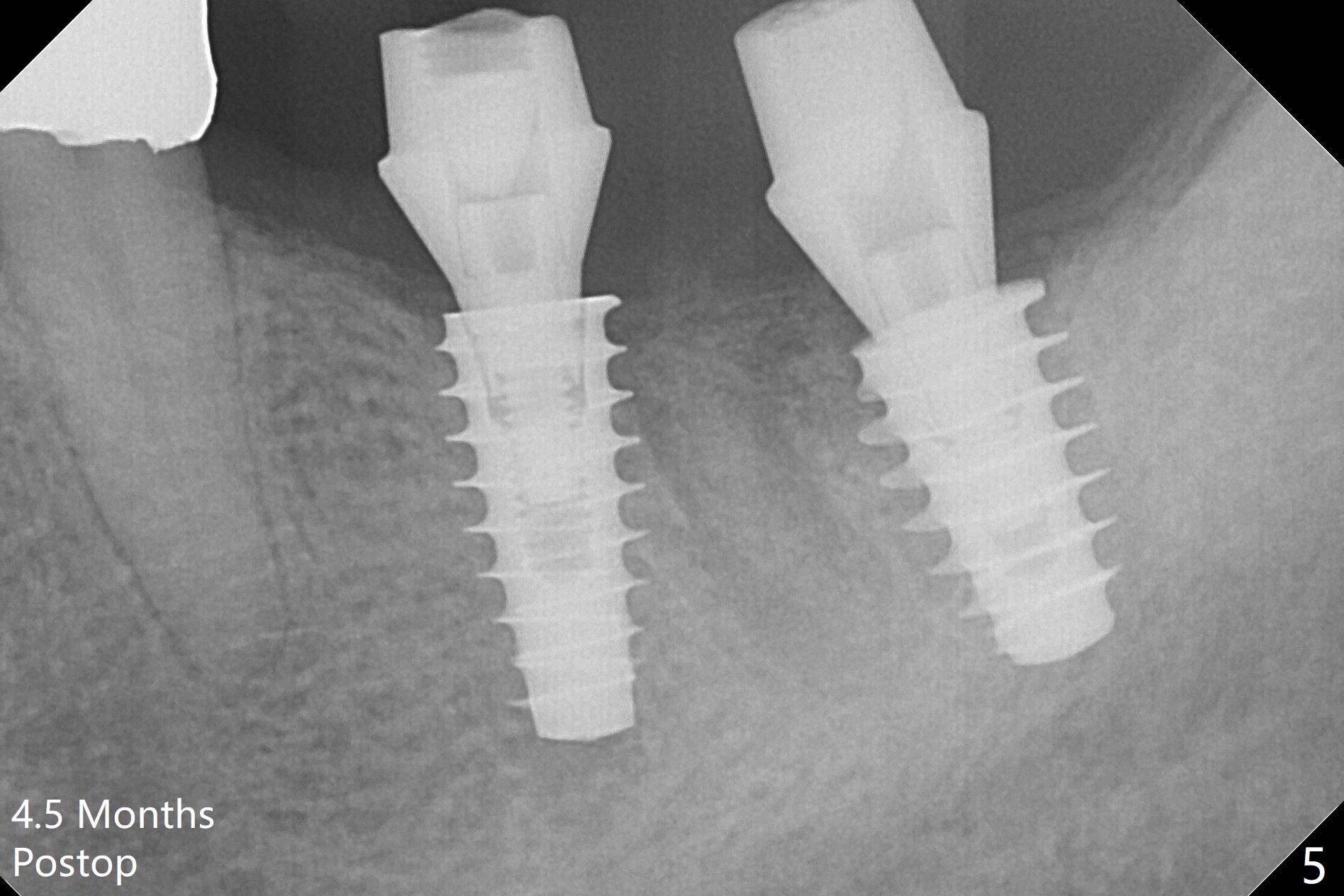
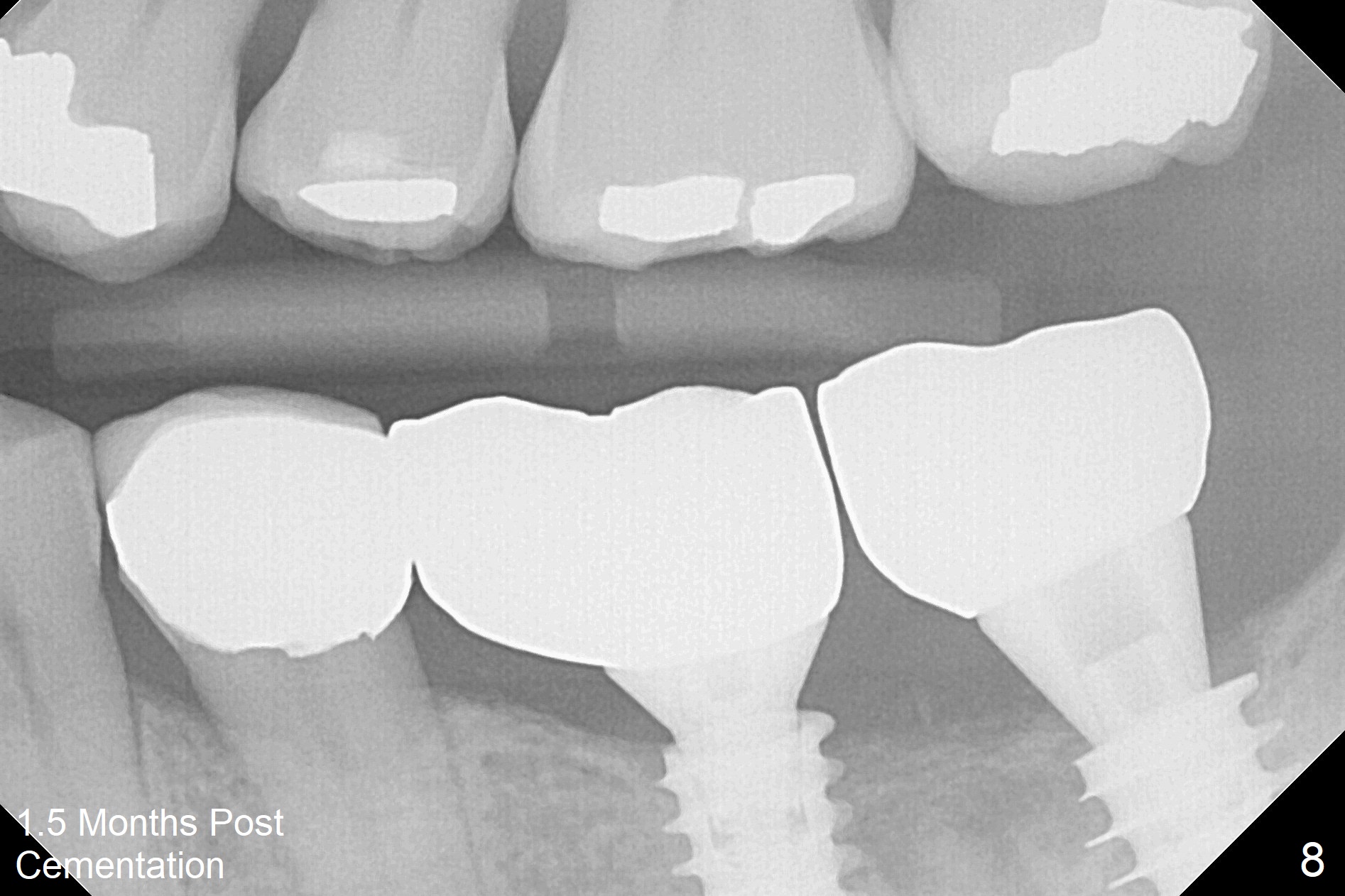
A drawback of placing an implant in the distal socket of the 2nd lower molar is closer to the Inferior Alveolar Canal. The implants seem to have osteointegrated 4.5 months postop (Fig.5). While the ridge at #19 appears to be wider than preop (as compared to Fig.1), that at #18 seems to be atrophic 5 months postop (Fig.6 * (1 week post cementation)). The distal implant placement at #19 may increase possibility of abutment screw loosening during functioning (Fig.7 *). When the patient returns for periodic exam 1.5 months post cementation, loose contact between the implant crowns is noted (Fig.8). The bony trabeculae form between the 2 implants crestally 12 months postop, i.e., 7 months post cementation (Fig.9). The loose contact between the 2 implants is corrected 14 months post cementation.
Return to Lower Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), Armaments
Xin Wei, DDS, PhD, MS 1st edition 11/14/2017, last revision 08/18/2019