|
|
|
|
|
|
Be Cautious about Immediate Implant After Block Anesthesia
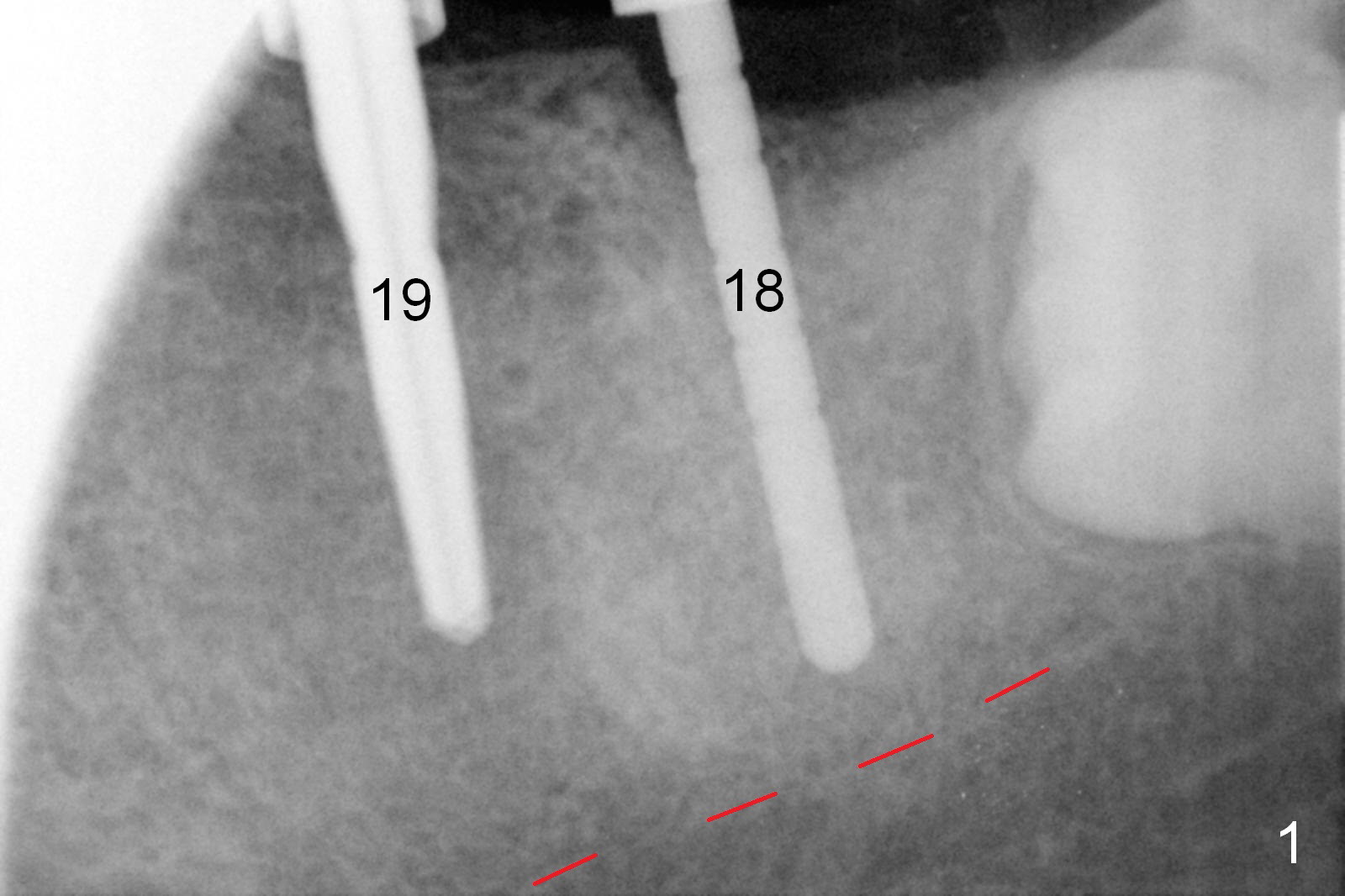
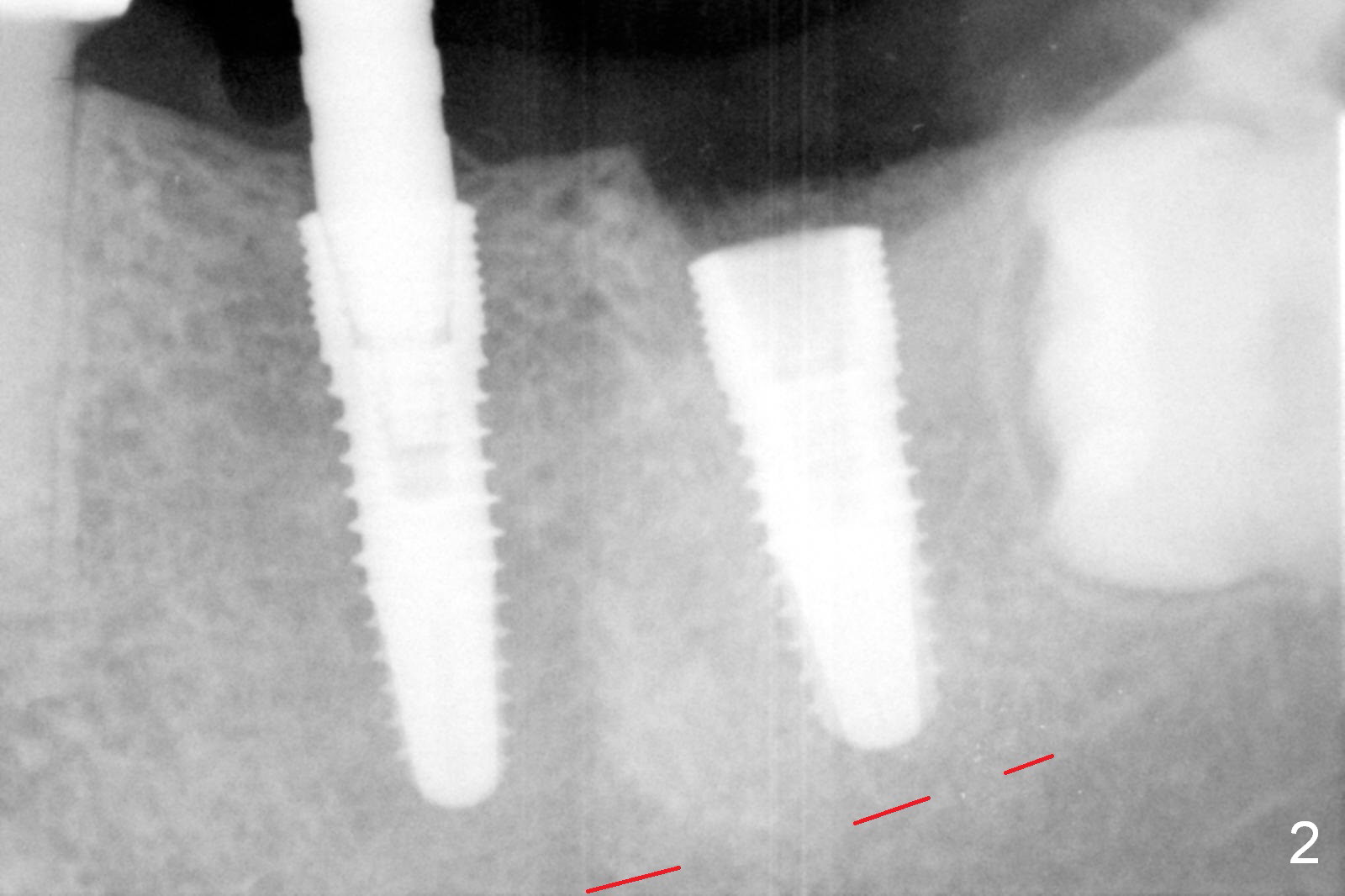
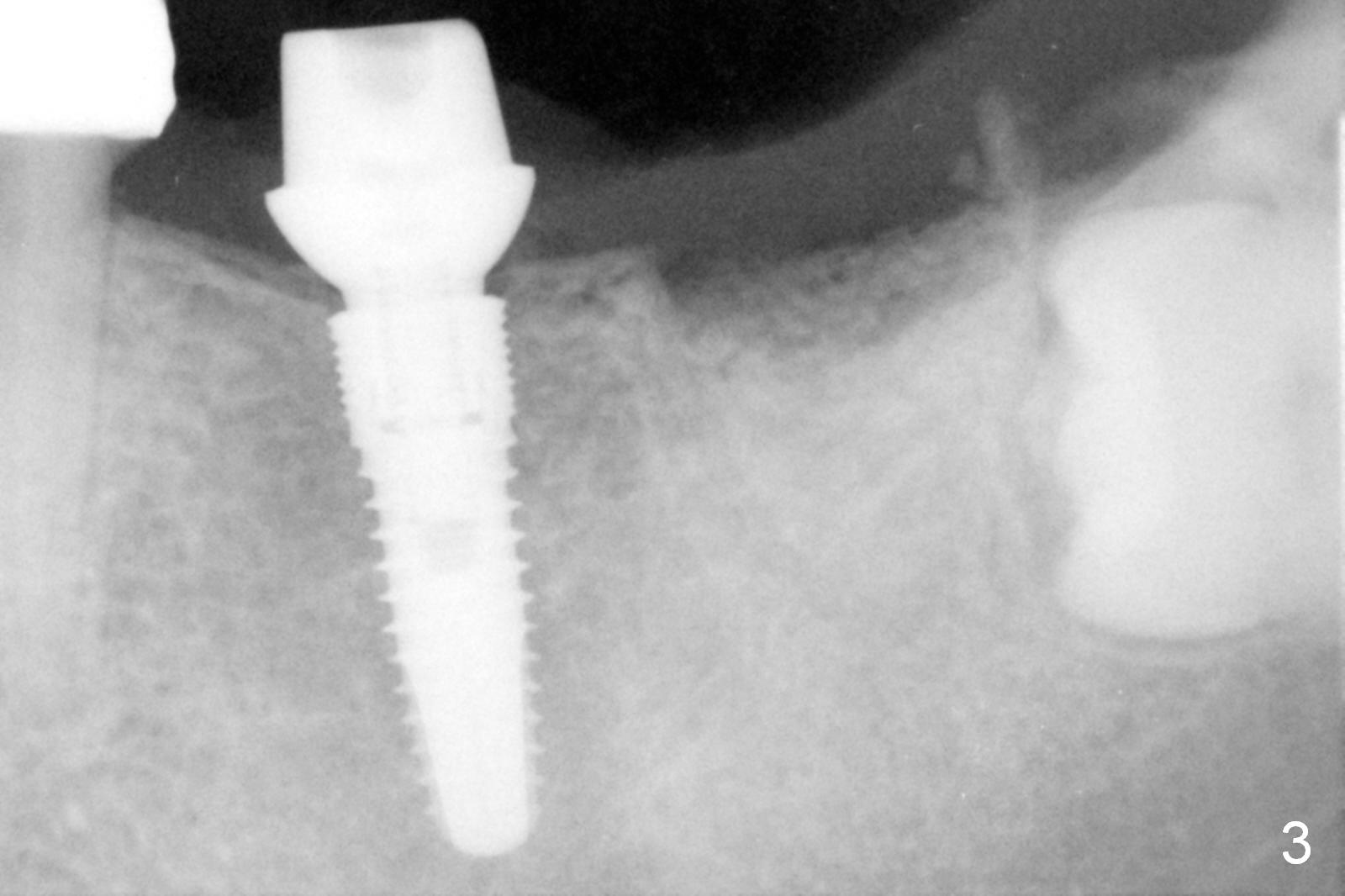
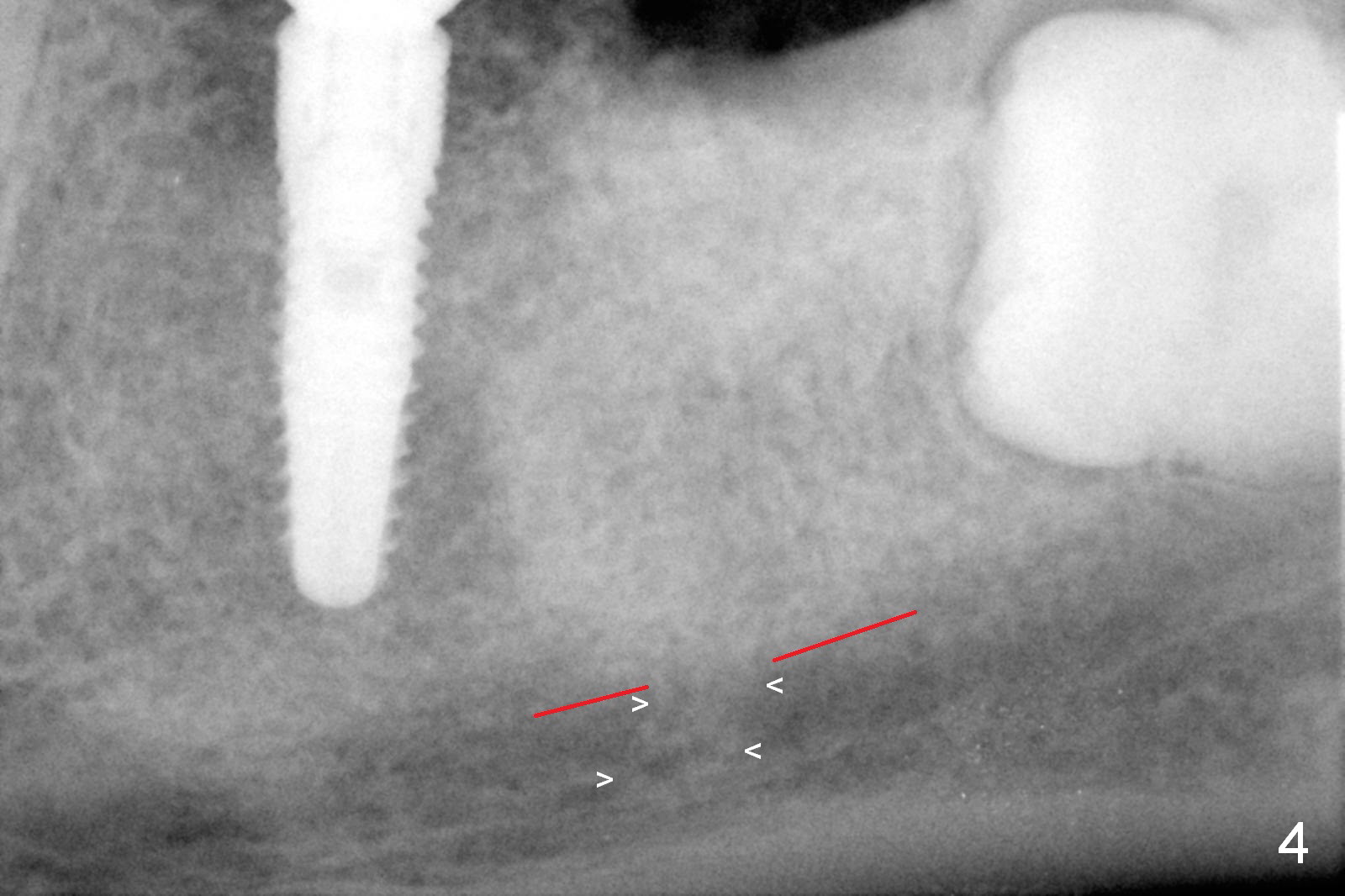
Infiltration anesthesia is enough for initial osteotomy at the site of #19 (Fig.1), but not for sectioning the tooth #18. Block anesthesia has to be administered. Fortunately it is safe to start osteotomy at #18 (~ 3 mm beyond the socket bottom, Fig.1 (red dashed line: the superior border of the Inferior Alveolar Canal (IAC))). A 4.5x14 mm implant is stable at #19, while a 5x12 mm one at #18 is not (Fig.2). Unfortunately bone graft has been placed. When the implant is removed, a 4.5x14 mm drill is used to deepen the osteotomy for 2 mm. The patient reports mild discomfort later on. Hemorrhage occurs, which is stopped when the same implant is re-placed. There is no stability. The implant is removed (Fig.3,4). More bone graft is placed, followed by collagen plug. It appears that bone graft has been pushed into the IAC (Fig.4 arrowheads). Medro dose pak is prescribed. In fact, no paresthesia is reported postop.
When block anesthesia is used, be cautious with implant placement (especially immediate one). Do not deepen osteotomy too readily. Use taps before implant placement. In this case, a larger implant should be inserted.
The patient will return 3.5 months postop. Take PA. Consider using Magic Expanders or Tatum Taper Osteotomes and Tatum or SM taps prior to placing a 5 or 5.3x10 or 12 mm implant. Prepare #15 blade.
Return to
Lower Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols,
Table),
#3
Xin Wei, DDS, PhD, MS 1st edition 07/14/2016, last revision 04/07/2017