


|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
||
Trajectory Associated with Immediate Implant
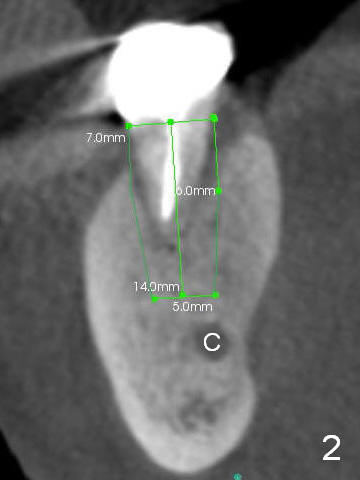
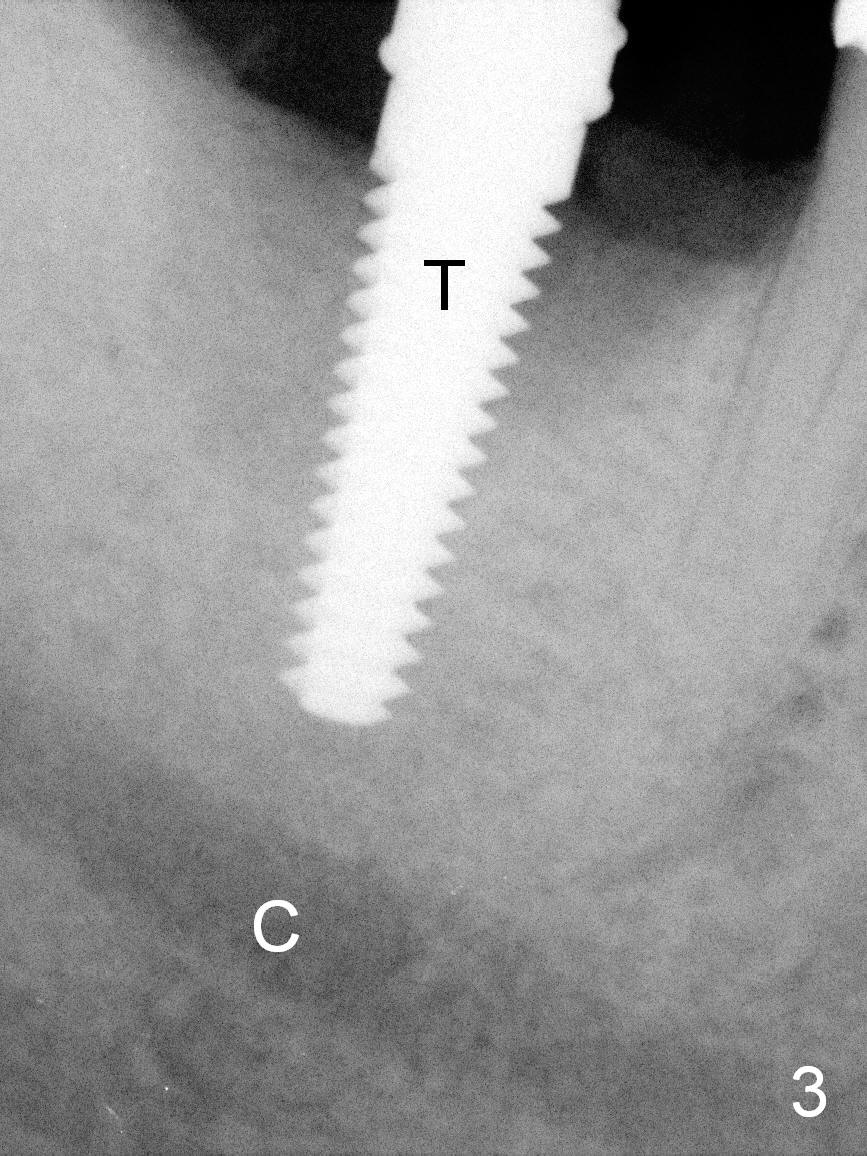
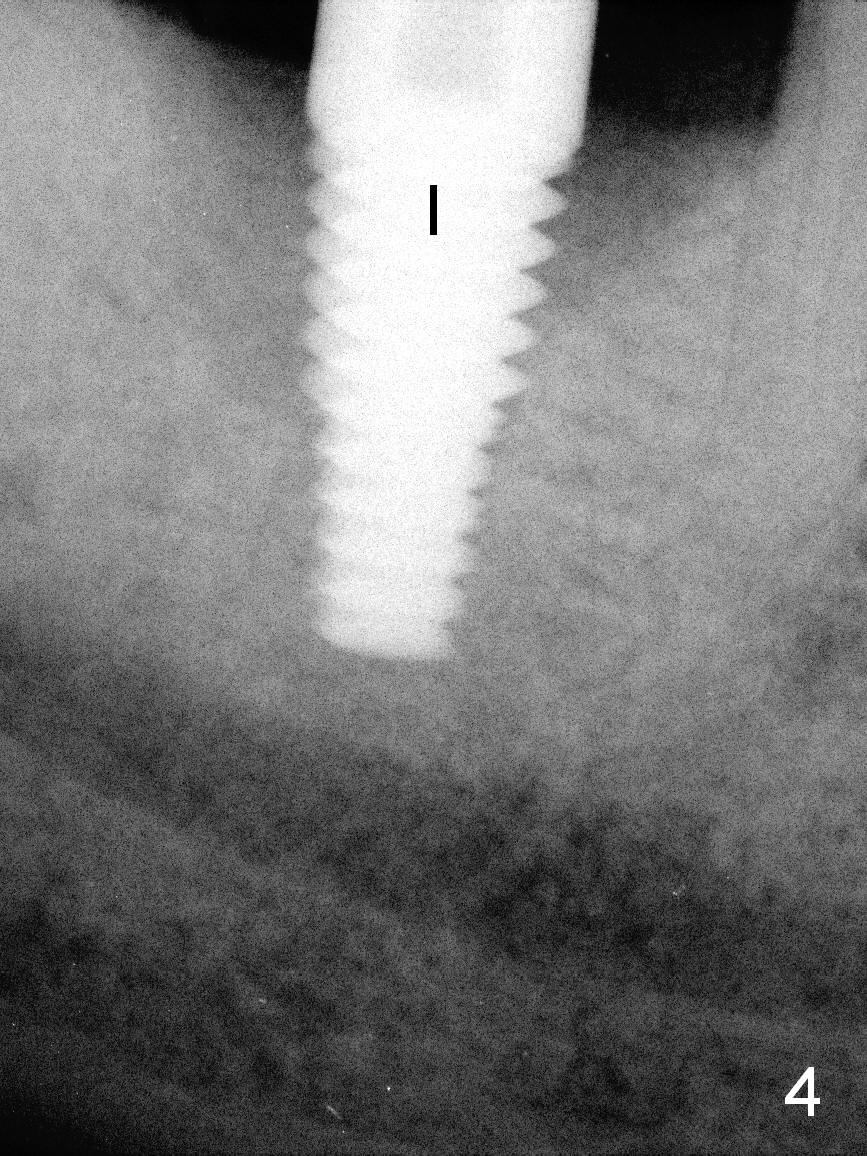
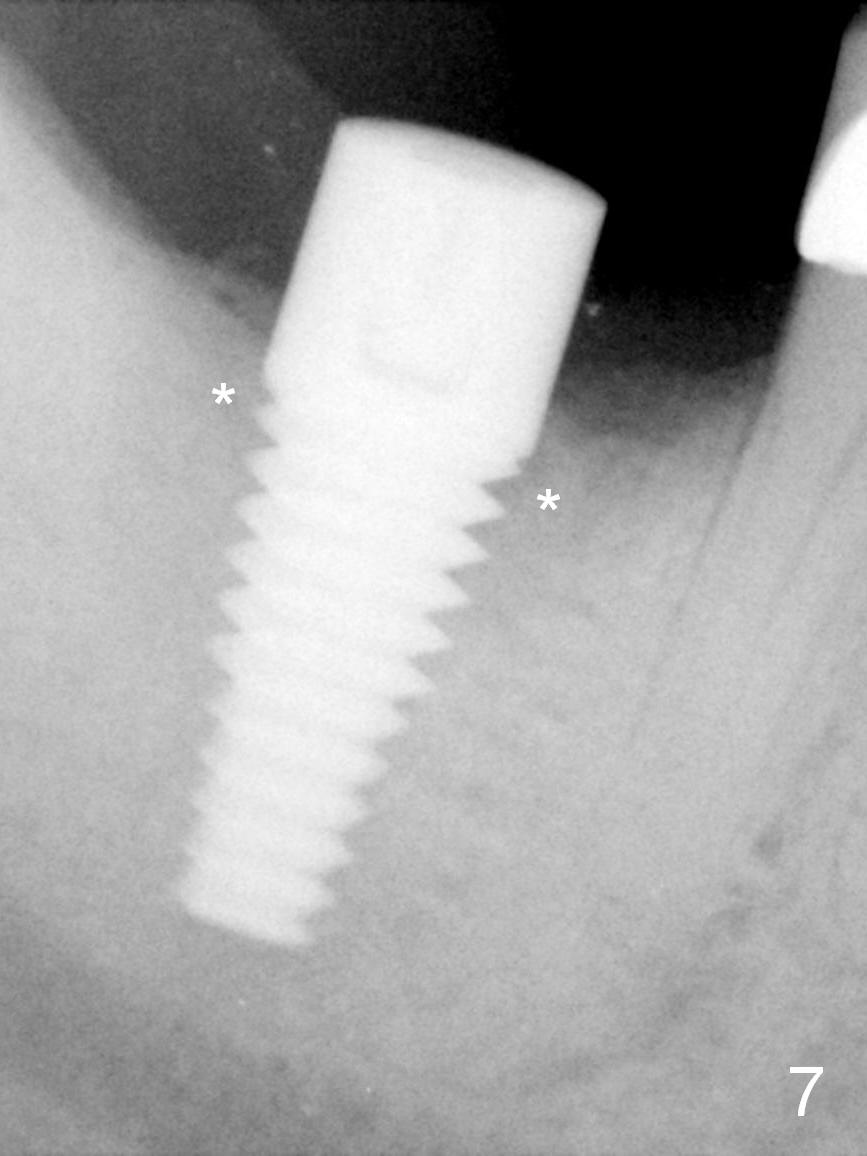
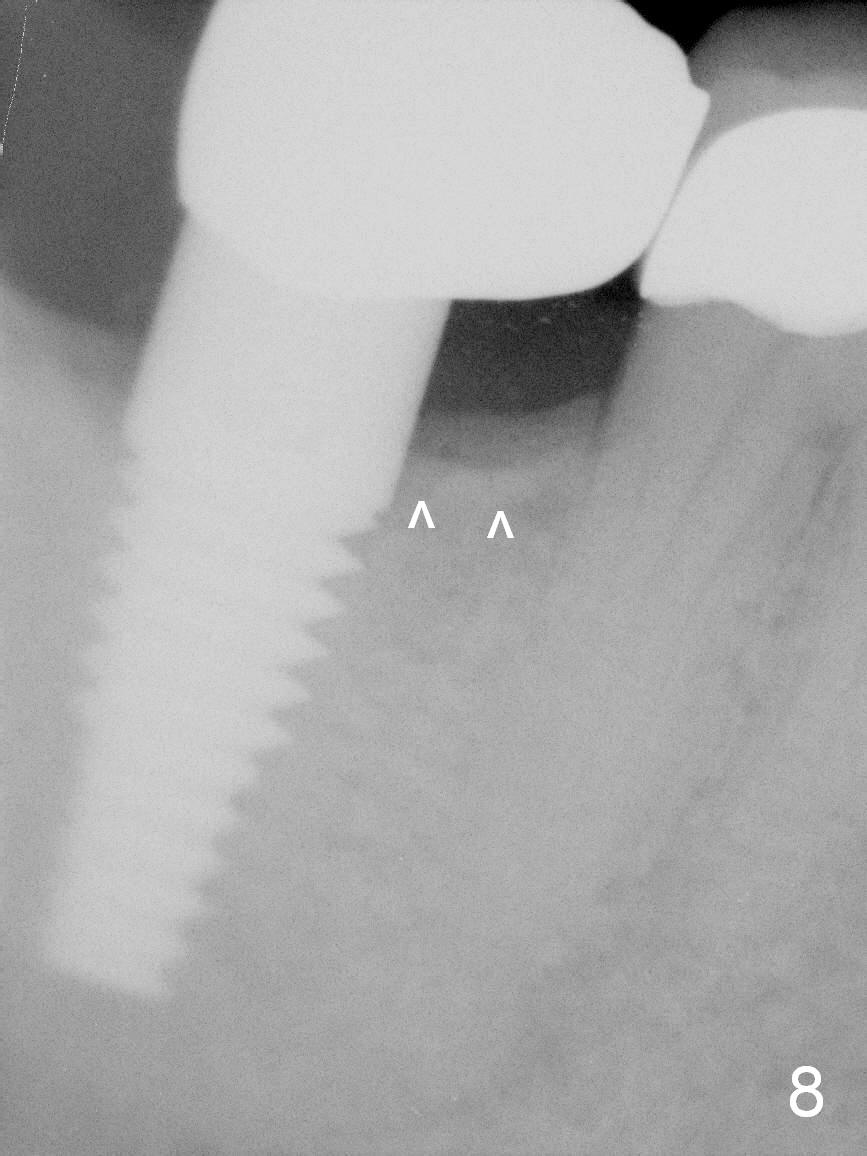
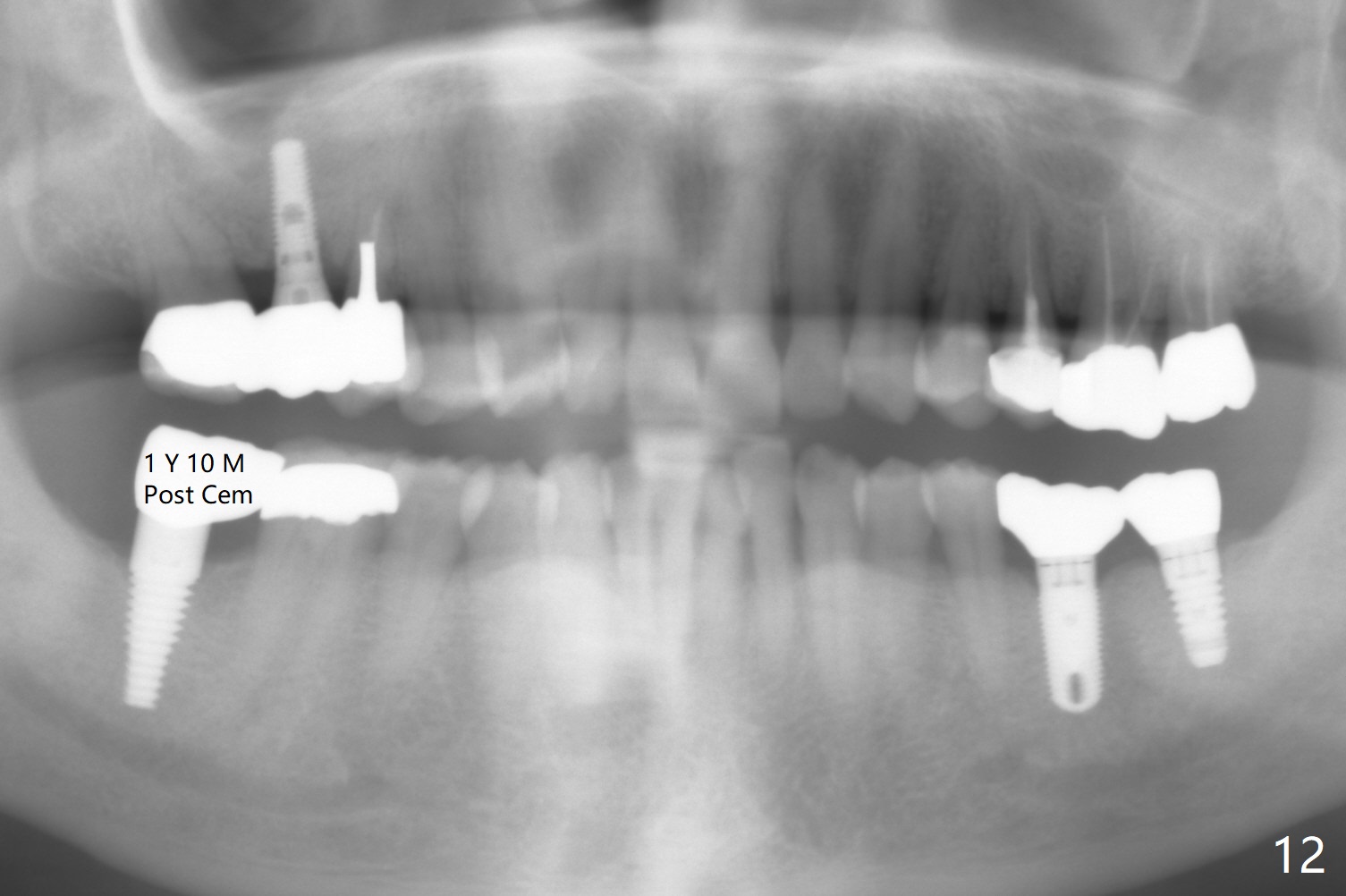
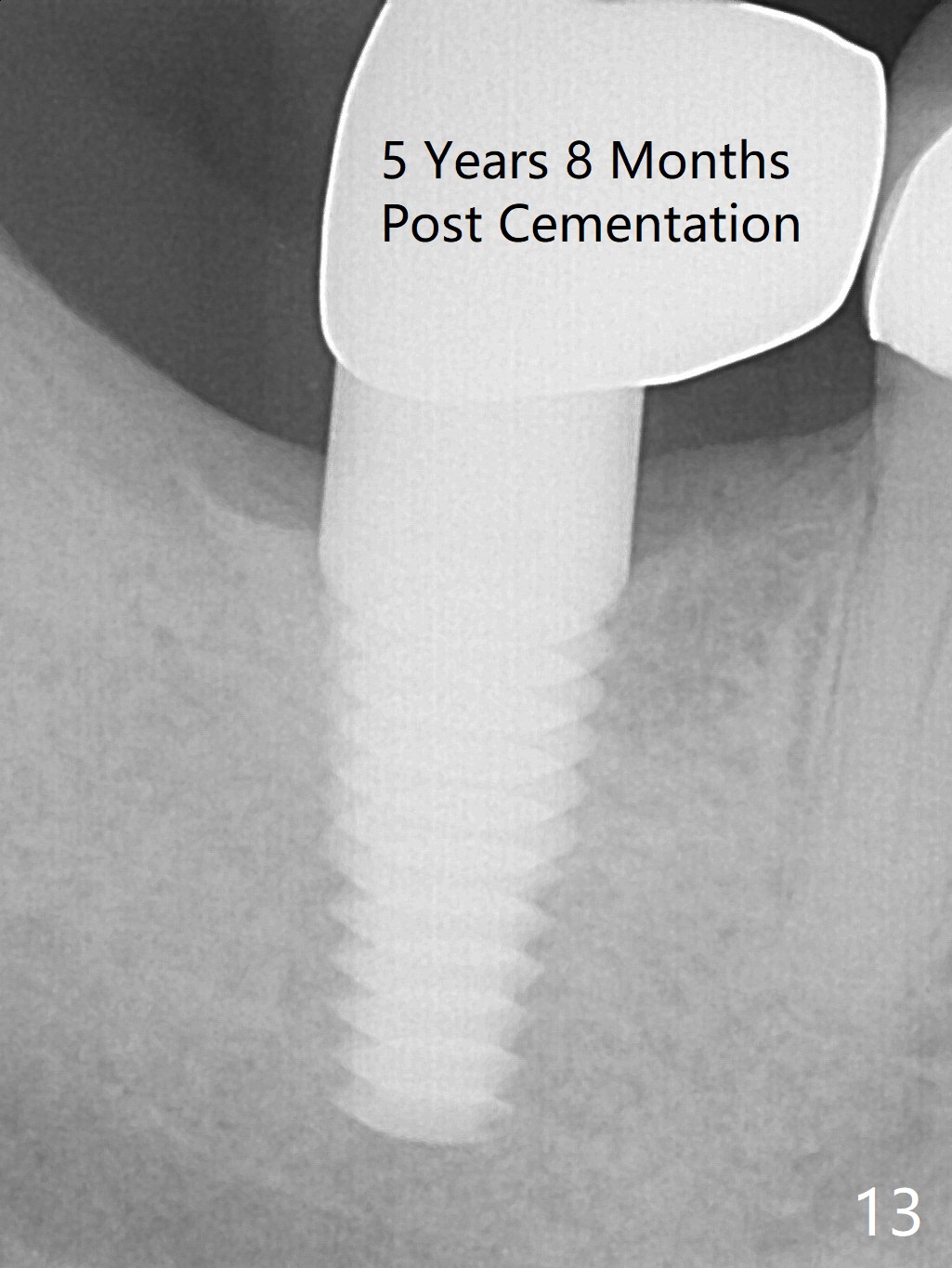
A 67-year-old man (bruxer) had endo failure at #31 (Fig.1). Coronal CT section of the distal root shows that a 7x14 mm gingiva-level implant can be placed (Fig.2 (C: Inferior Alveolar Canal)). Immediately after extraction, osteotomy is initiated with drills (D1 or 2 bone), followed by insertion of a 4.5x17 mm tap (Fig.3). A 6x17 mm implant is placed with insertion torque > 60 Ncm (Fig.4 without bone graft). The gingiva contacts the implant, while it is difficult to approximate the mesial aspect of the socket. Periodontal dressing is applied. One month and a half postop, the gingiva around the implant is healthy (Fig.5); there is fresh granulation tissue in the mesial socket (Fig.6 <). Bone density in the mesial and distal sockets appears to increase 3 months postop (Fig.7 *). A high-noble crown is cemented 4 months postop. The mesial crest has formed cortical bone nearly 2 years post cementation (Fig.8 ^).
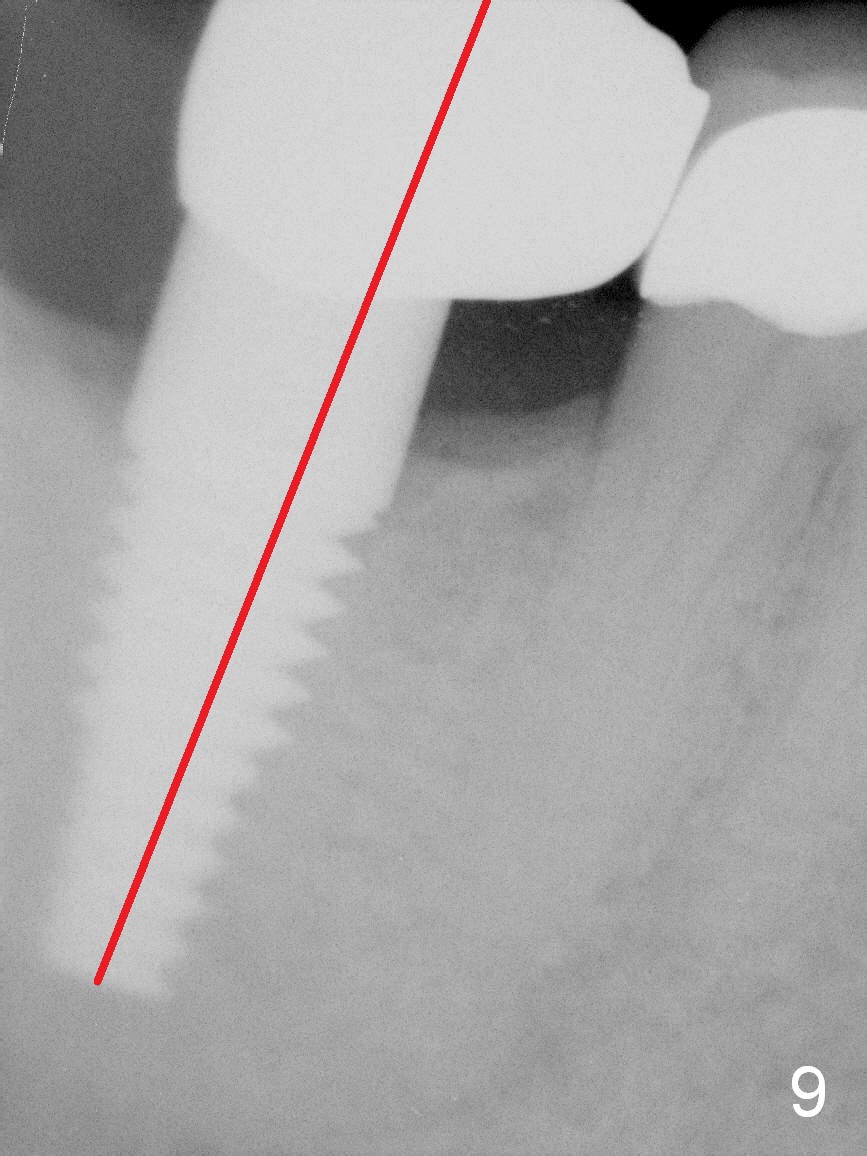
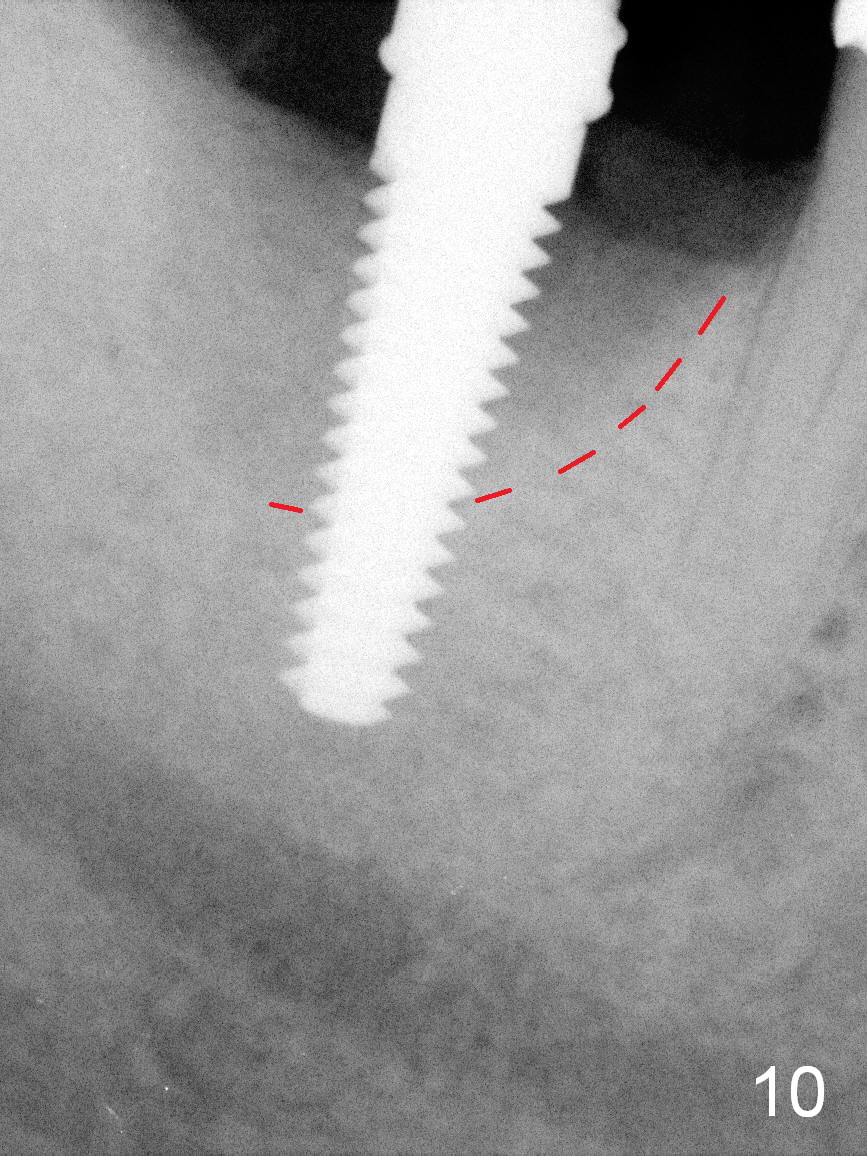
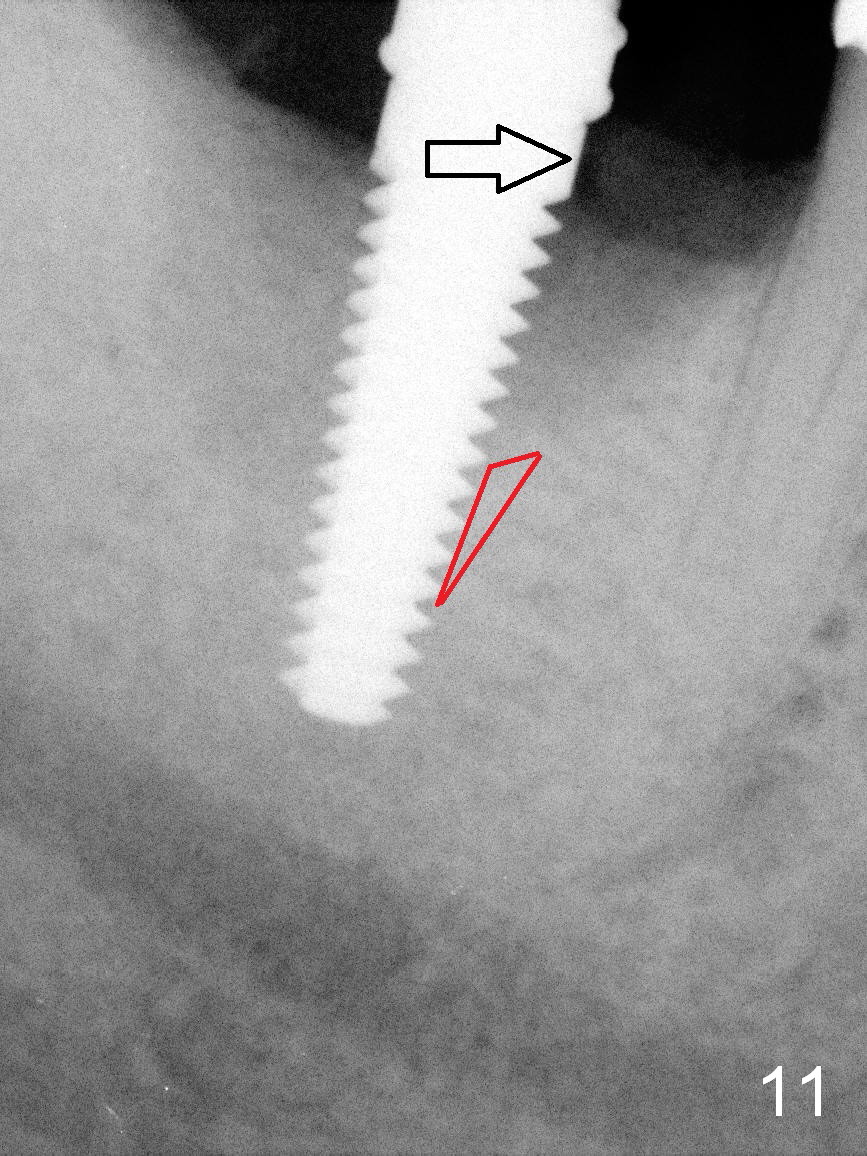
It appears that the axis of the implant is off (Fig.9). In fact the osteotomy is established in the mesial slope of the socket (Fig.10 red dashed line). There is more resistance mesially. To correct the trajectory (Fig.11 arrow), the mesial bone should have been removed (red triangle). Or the implant should have been leaned as mesial as possible while being placed.
Return to Lower Molar Immediate Implant
Better Trajectory
Xin Wei, DDS, PhD, MS 1st edition 09/07/2015, last revision 07/16/2019