|
|
|
|
|
|
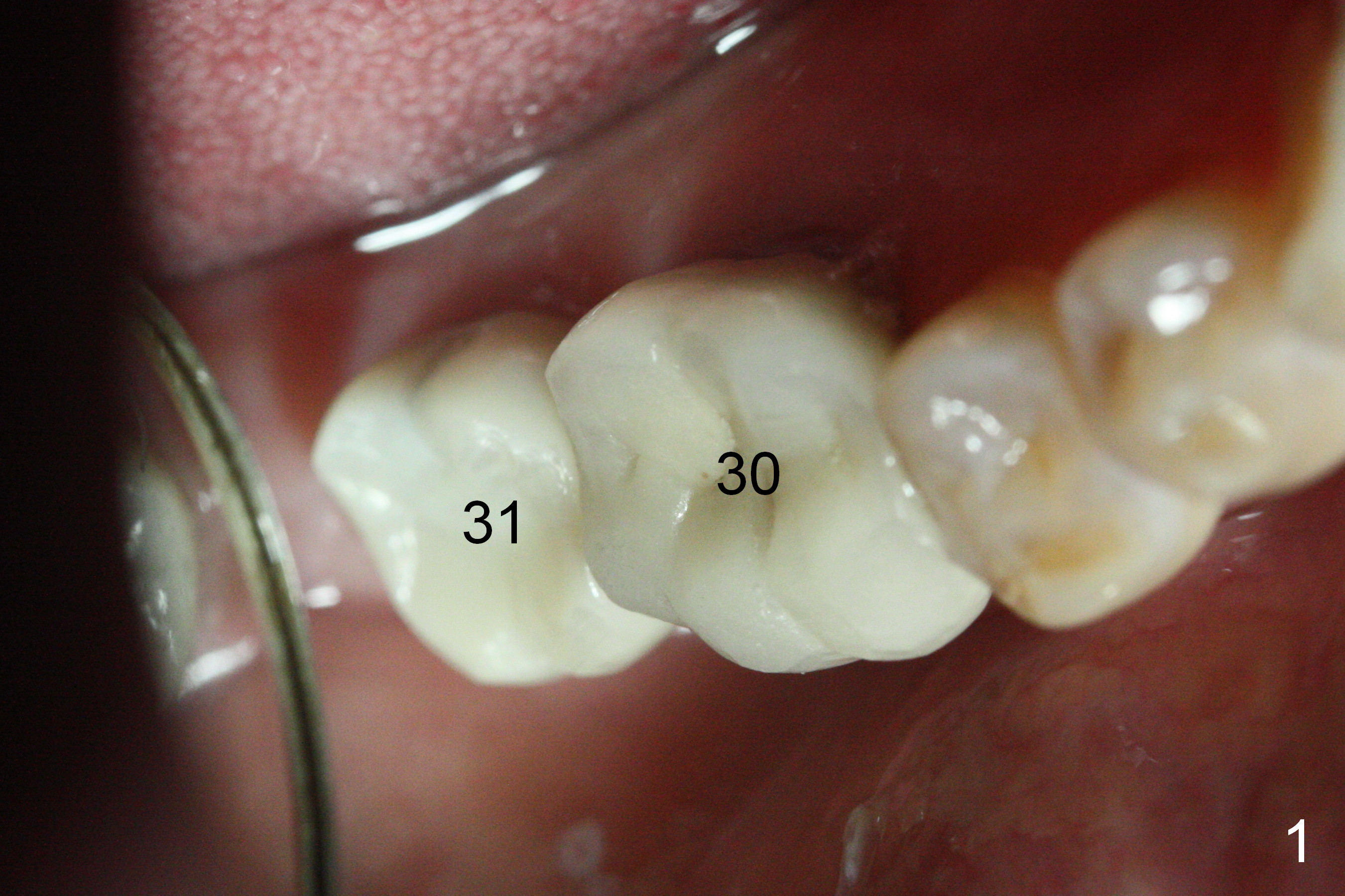
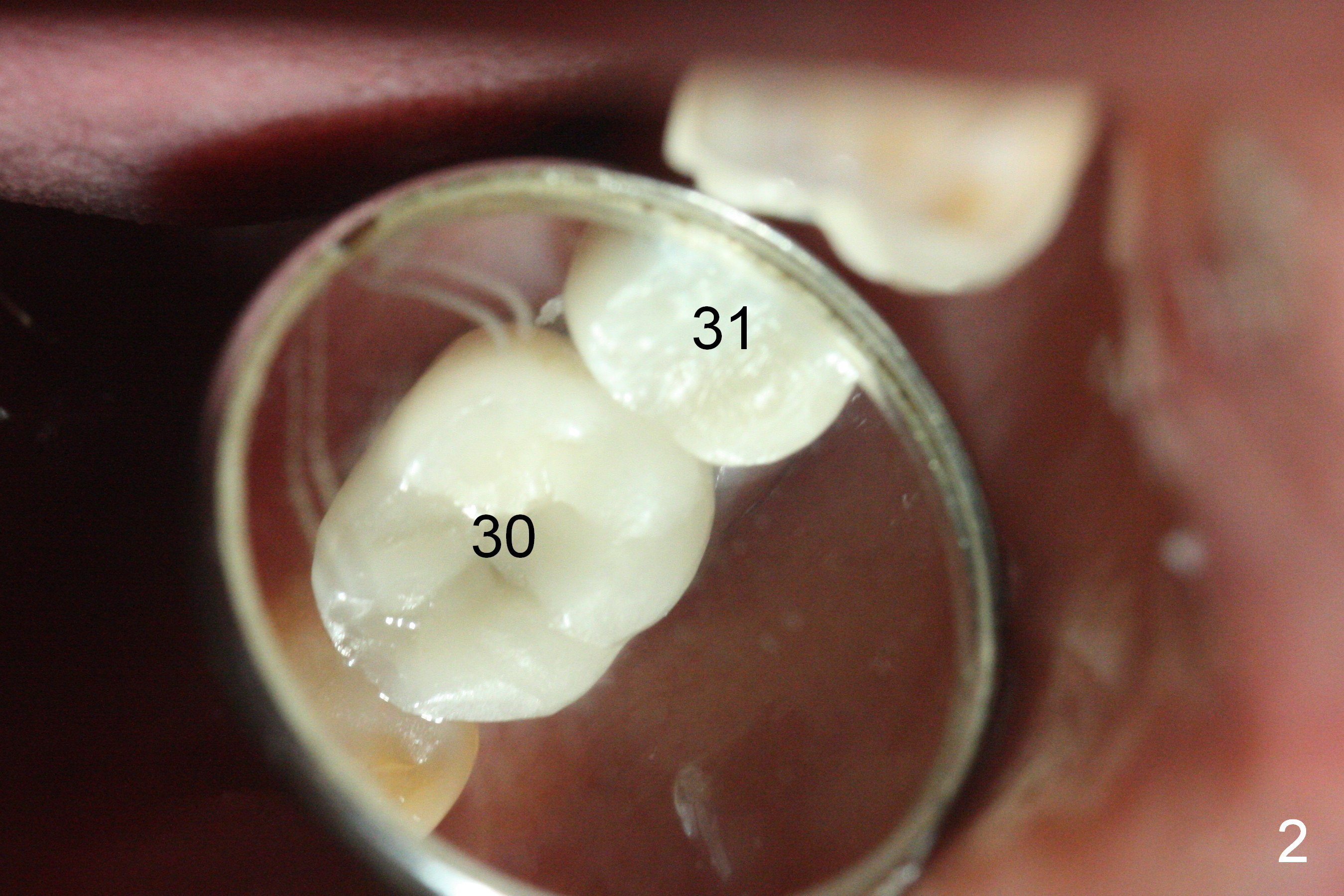
Redo #31 Crown
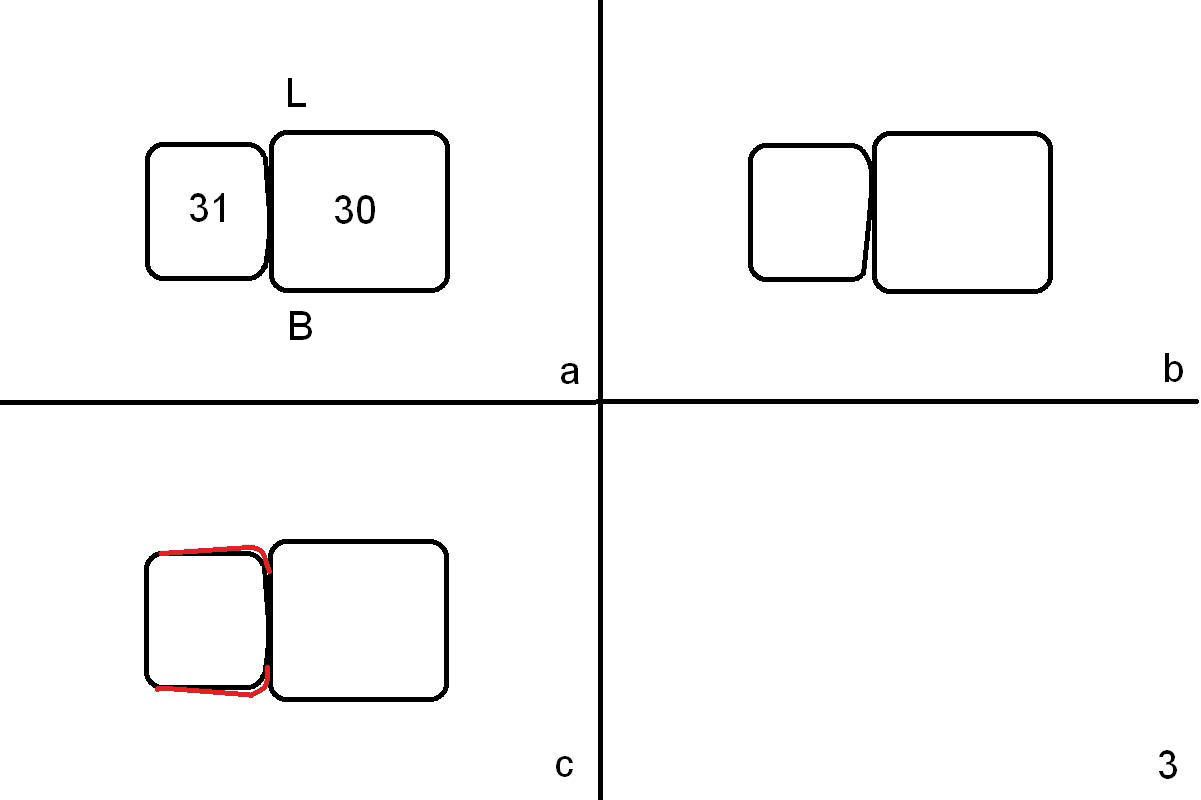
Three months post cementation of #31 crown, the patient returns with chief complaint of "food impaction". Exam shows that the crown at #31 is smaller than that at #30 (Fig.1,2). The proximal contact is small and uneven (Fig.3b illustration (occlusal view; B: buccal; L: lingual), as compared to the ideal condition in Fig.4a). Food impaction is more likely related to small contact area than so-called gap. In fact the floss has a certain degree to pass the contact. Therefore when a new crown is designed and fabricated, try to make contact surface as large as possible. For example, make the mesial portion (occlusal table) of the crown larger than the distal one buccolingually (Fig.3c red lines) so that the proximal contact could be a little larger. The large mesial occlusal table is alright with the implant, which has been placed for 14 months (well heals).
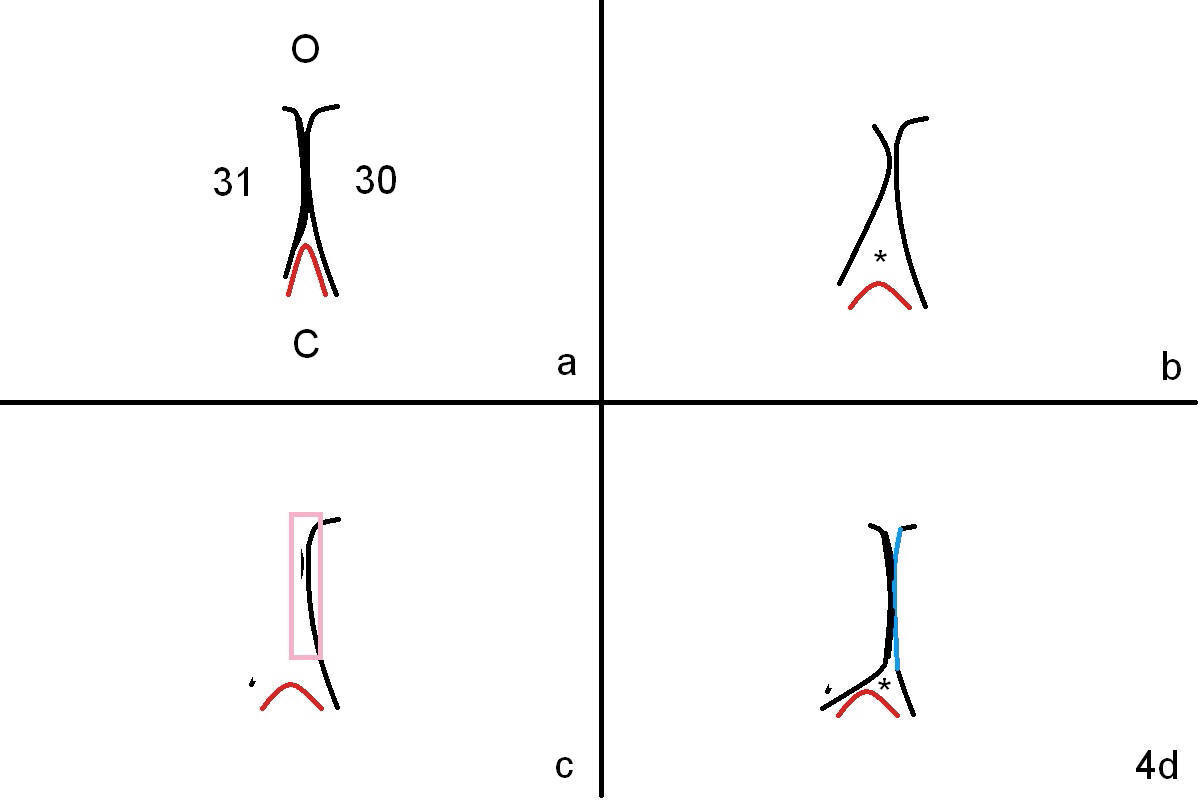
The ideal contact area (buccal view) should be also wide occlusocervically (Fig4a (O, C)). Between the 2 natural teeth is the gingival papilla (red outline). The latter undergoes recession after extraction and implant (Fig.4b red outline). When the contact is small and light, the food is easily driven into the large gingival embrasure (*). The tooth #30 has a PFM crown; the distal surface is a slope. In order to increase the contact area, the distal surface is flattened (Fig.4c pink rectangle to Fig.4d green line) after removal of the crown of #31. The mesial surface of the new crown is to be fabricated as wide as possible occlusocervically. In addition, try to close the gingival embrasure as much as possible (Fig.4d *, as compared to Fig.4b).
Last, reduce die space so that there is less rotation of the crown during cementation. Rotation may be associated with uneven contact of the proximal surfaces (Fig.3b).
Return to
Lower Molar Immediate Implant,
Technicians
Xin Wei, DDS, PhD, MS 1st edition 12/14/2016, last revision 12/15/2016