




|
|
|
|
|
||
|
|
|
|
|||
|
|
|
|
|
||
|
|
|||||
Taps Form Osteotomy
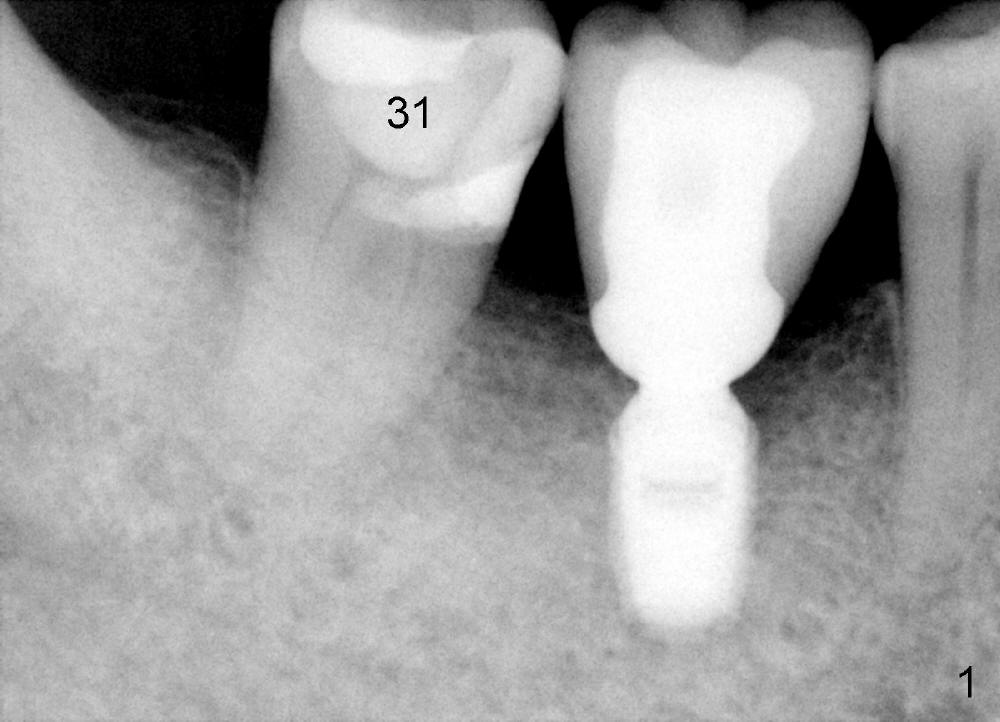
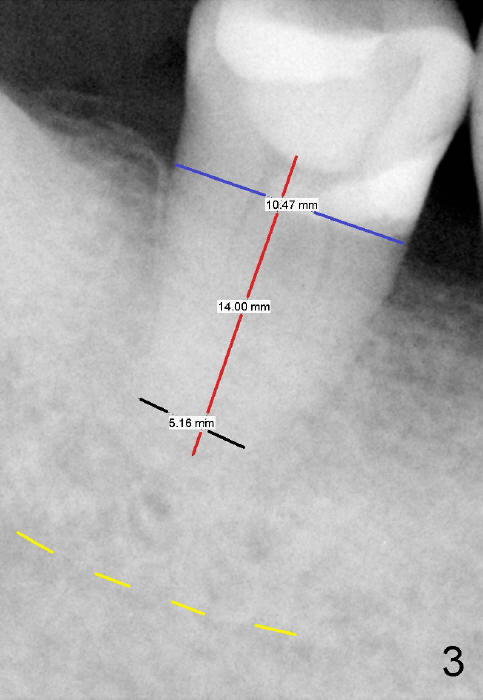
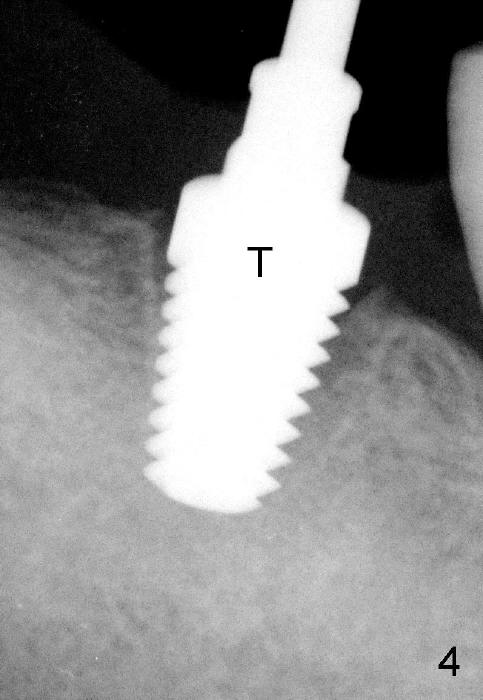
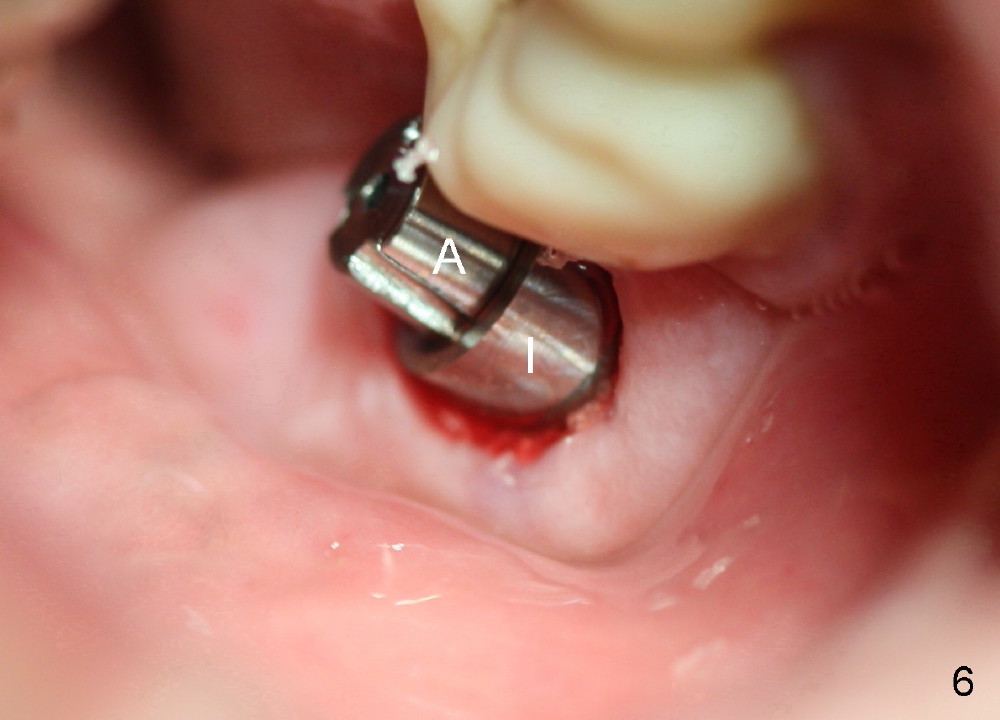
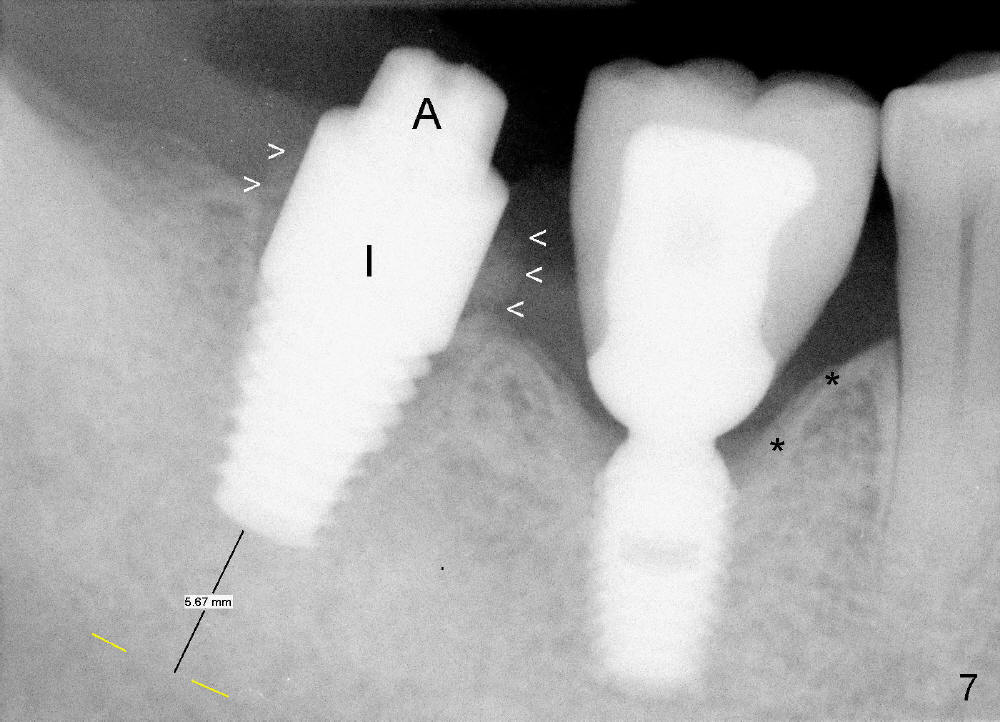
A 76-year-old man requests emergency root canal therapy (RCT) for the lower right 2nd molar (Fig.1: #31, PA taken 5 year earlier). Initial excavation reveals that the tooth is beyond salvation (Fig.2). The Inferior Alveolar Canal (IAC, Fig.3 yellow dashed line) is barely identified. To avoid complication, an implant is to be confined to boundary of the socket (7x14 mm). No drill is to be used. A 5x14 mm tap is inserted without stability, whereas a 6x14 mm one establishes initial stability (apparently in its apex). When a 7x14 mm tap is placed, stability is satisfactory; the tap almost obliterates the socket (Fig.4 T). When a 7x14 mm implant is placed, it tilts lingually. It is removed with intention to use drills to form osteotomy in the linguoapical area. The socket is re-examined. It is felt fairly large. The trajectory of the implant should be able to change when the implant is re-inserted. In fact, it does (Fig.5 I: implant; A: straight short abutment). The implant platform is at the gingival margin except buccal (Fig.6). Allograft and Osteogen is placed in the remaining mesiobuccodistal socket (Fig.6,7 arrowheads). Although there is 5-6 mm from IAC, the patient experiences pain when the apical socket is curetted and the implant is placed. Multiple injection should be added before implant placement is finished.
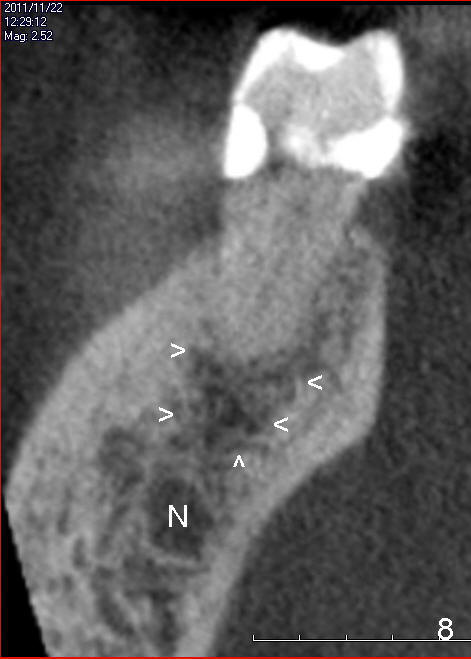
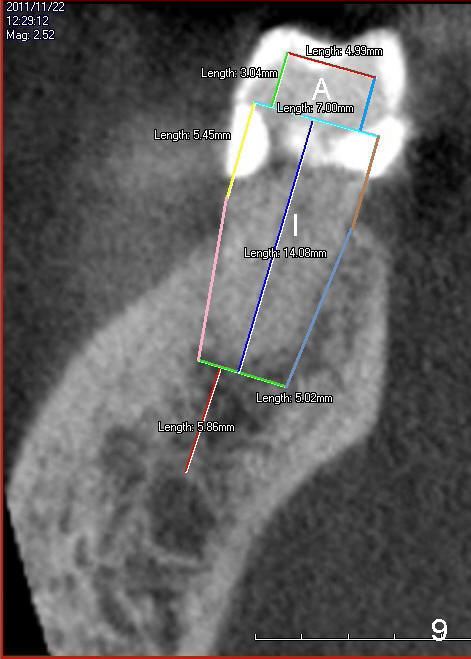
After surgery, CBCT taken 3 years ago is reviewed. It appears that there is periapical radiolucency (Fig.8 arrowheads, hidden infection, pain source). According to all of preop and intraop information, it appears that the implant (Fig.9 I) is slightly placed apical to the original socket (compare to Fig.7) so that there is room for the short abutment (A) placement and reduce the degree of exposure of buccal threads. When anesthesia resolves 6 hours postop (Marcaine), there is no severe pain or paresthesia.
The patient returns for restoration 4 months postop. There is no thread exposure (Fig.10), although there is mild buccal rough surface exposure (Fig.12 *). The latter is probably related to the buccal placement of this large implant. It would be the best to use drill to move osteotomy lingually (not apically) so that the implant would be placed more lingually and there would be less chance of buccal thread exposure. The implant surface exposure does not get worse much 1 year 1 month post cementation (Fig.12). The surrounding gingiva is healthy and keratinized. This is probably due to the fact that water pik has been used for oral hygiene.
Return to Lower Molar Immediate Implant,
Dr.
Wu
Xin Wei, DDS, PhD, MS 1st edition 11/25/2014, last revision 05/14/2016