

|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
Overcorrection
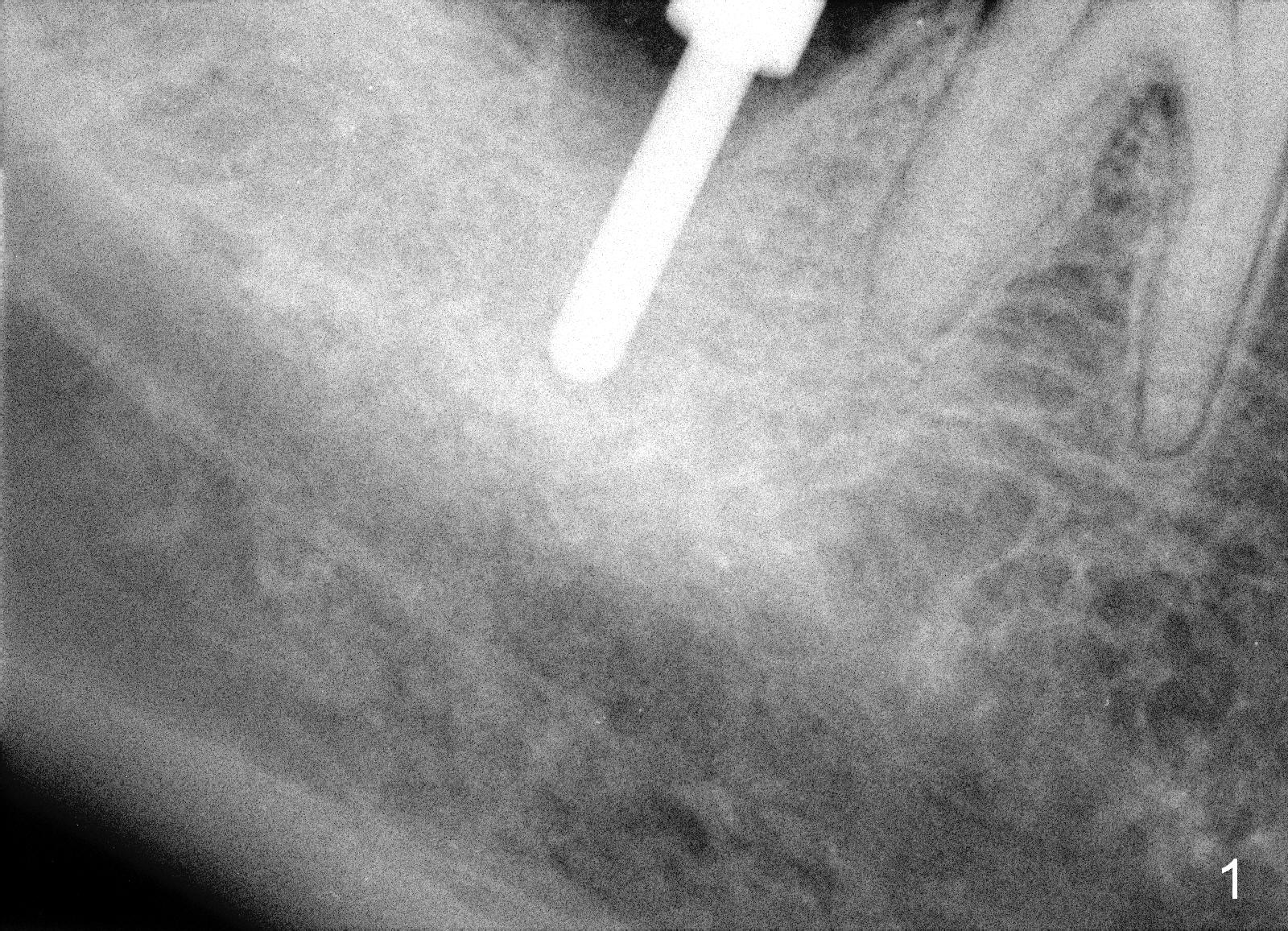
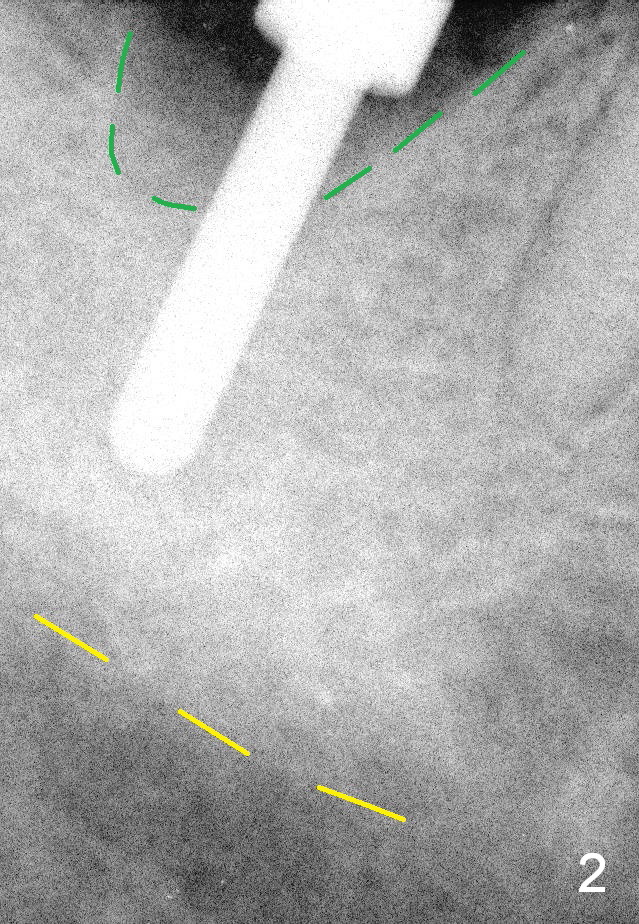
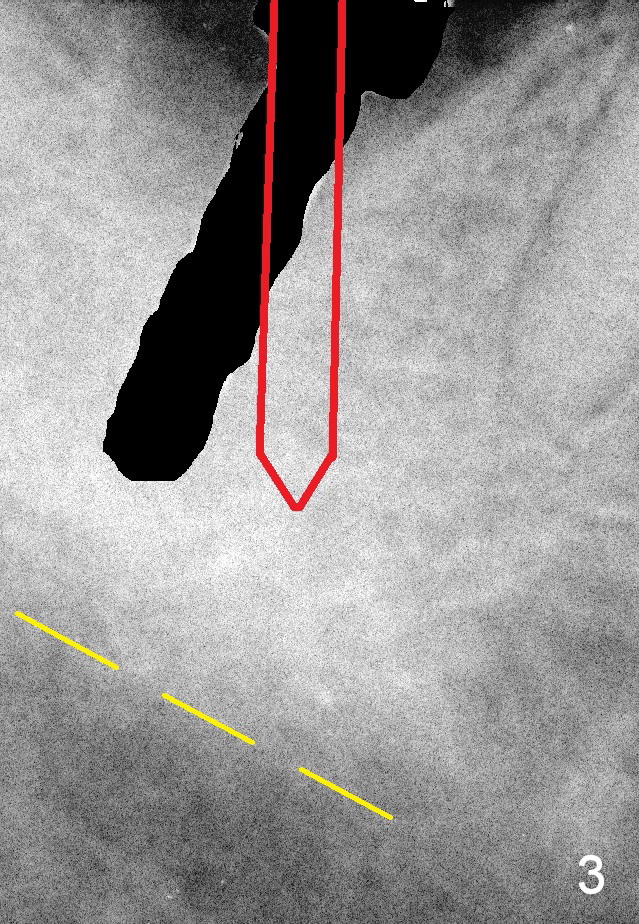
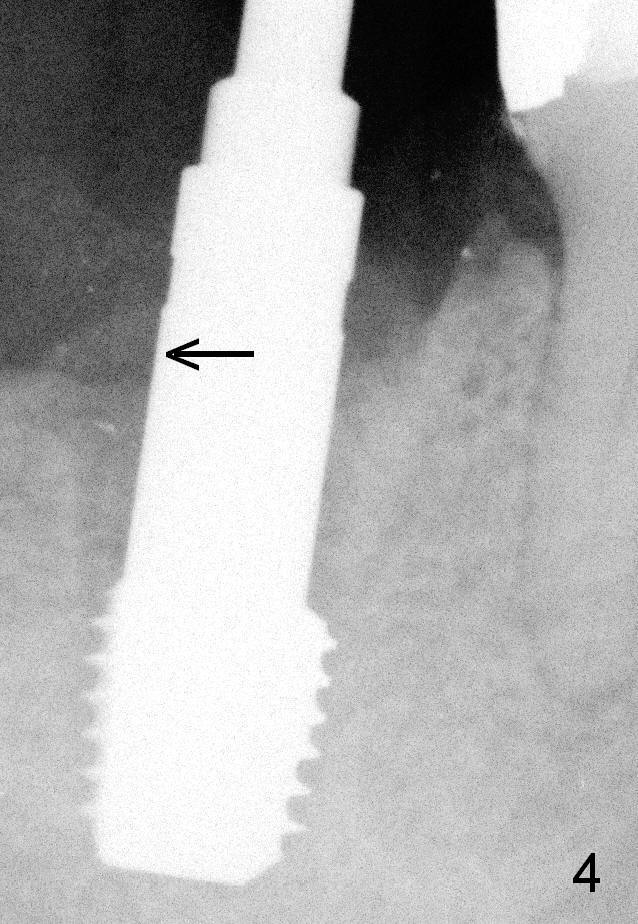
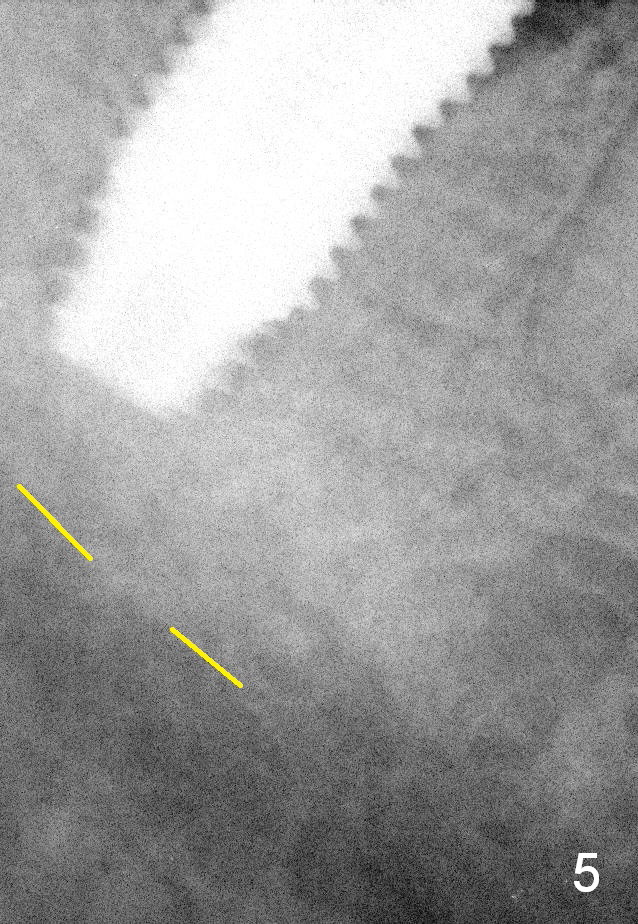
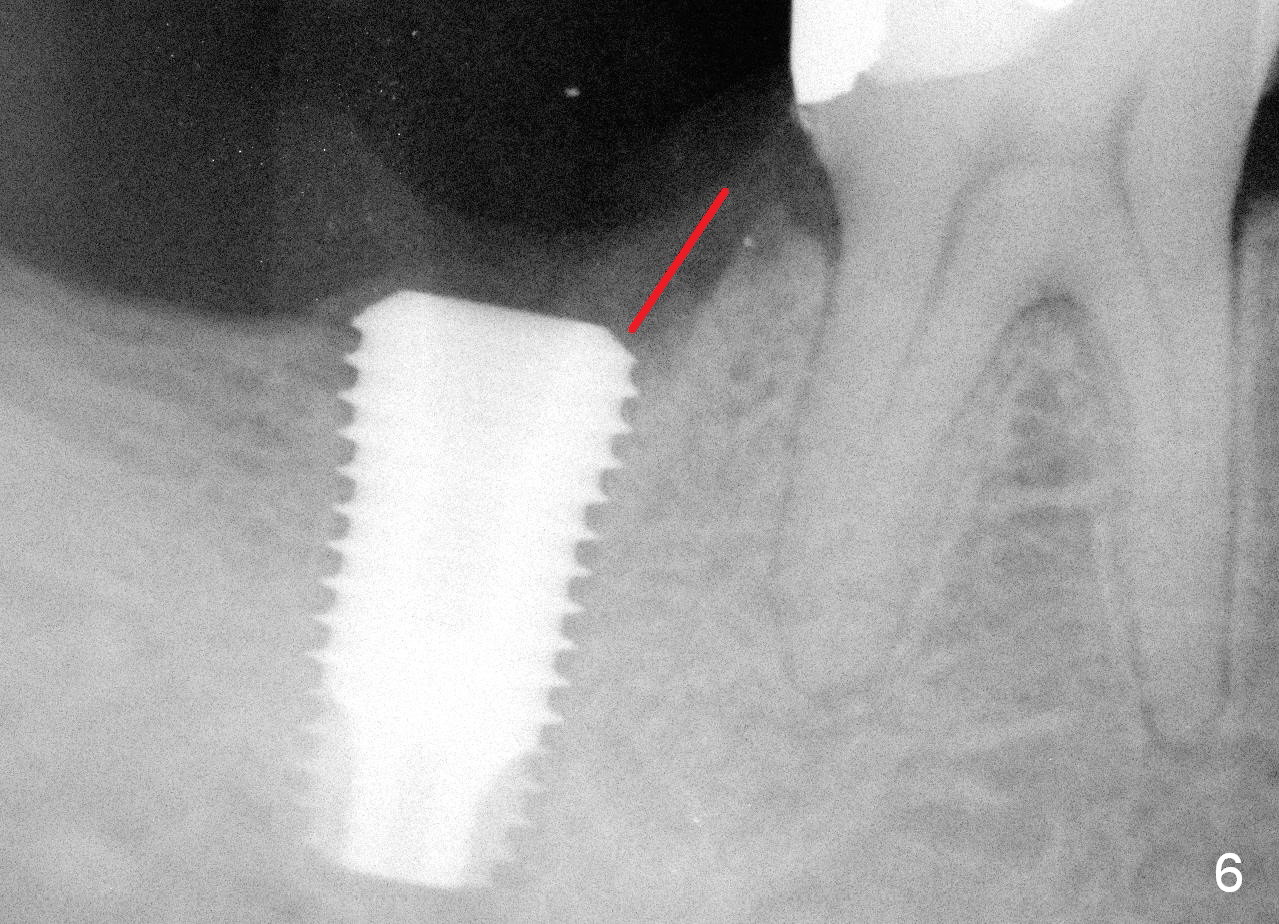
As planned, osteotomy is initiated in the mesial slope of the socket after extraction (Fig.1,2). As the osteotomy is being enlarged, it is being shifted unavoidably distally (Fig.4 arrow: 6 mm tap). Although the implant (Fig.5,6: 6.5x12 mm) is placed with high insertion torque and away from the Inferior Alveolar Canal (yellow dashed line), the implant is substantially under the mesial crest (Fig.6 red line). The trajectory should have been overcorrected (moved mesially and changed the angle) once it is found insufficient at the early stage of osteotomy (Fig.3 from black area to red outline).
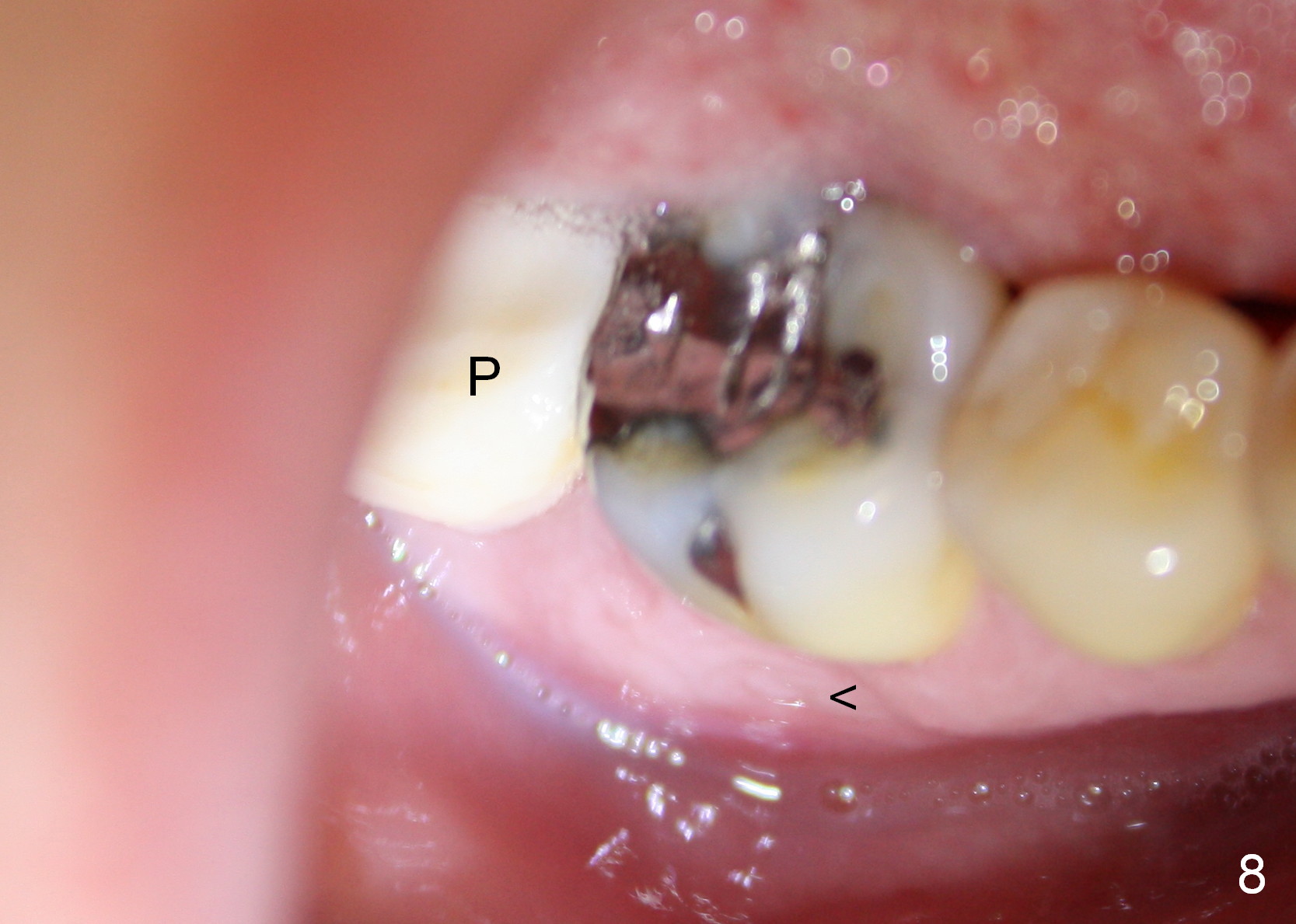
An abutment is placed immediately to hold an immediate provisional, which in turn keep bone graft in place. In spite of extraoral (Fig.7) and intraoral (Fig.8 <) herpetic infection, the provisional is stable 10 days postop (Fig.8 P).
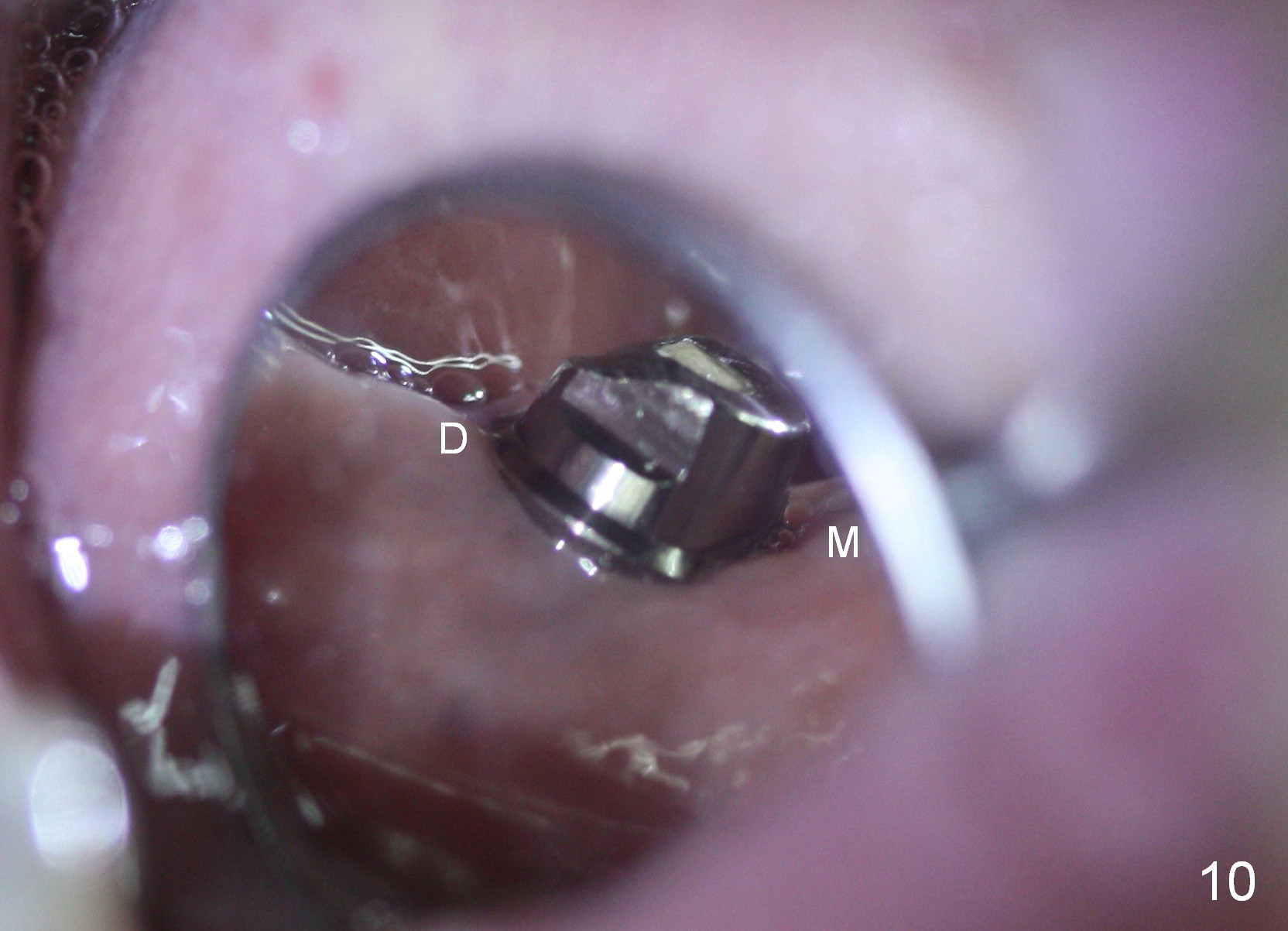
Three days later, the provisional dislodges. The gingiva around the implant/abutment is healthy. While the buccal (Fig.9) and mesial margin (Fig.10 M) is subgingival, the lingual and distal (Fig.10 D) is equigingival.
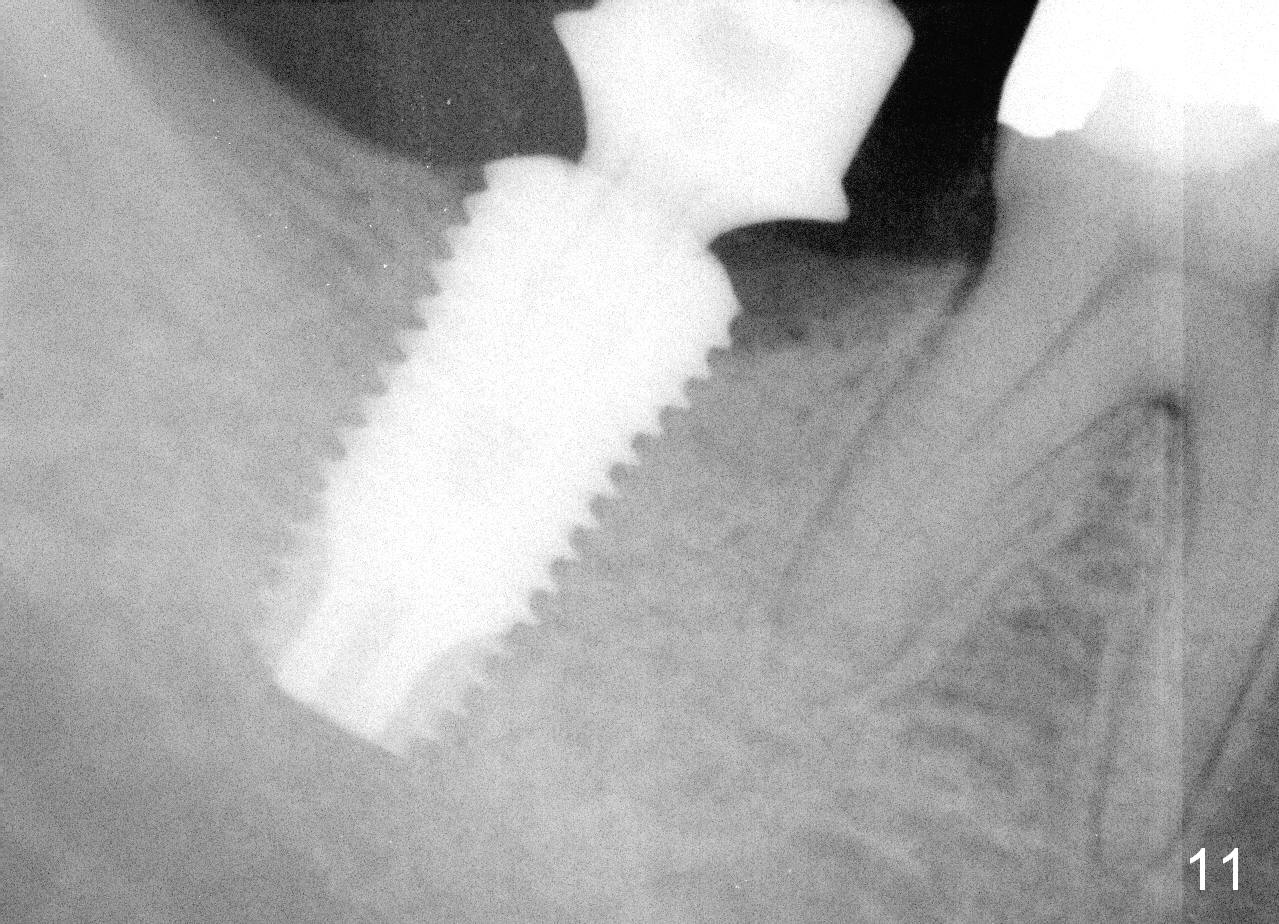
The patient returns for restoration 6 months postop. There is perforation in the occlusal surface of the provisional. It is obvious that the patient chews with it. The peri-implant gaps appear to have been closed (Fig.11, as compared to Fi.g6).
Return to
Professionals,
Lower Molar Immediate Implant,
Dr. Wu
Xin Wei, DDS, PhD, MS 1st edition 04/26/2015, last revision 10/06/2015