


|
|
|
|
|
|
|
|
Complex Distal Defect
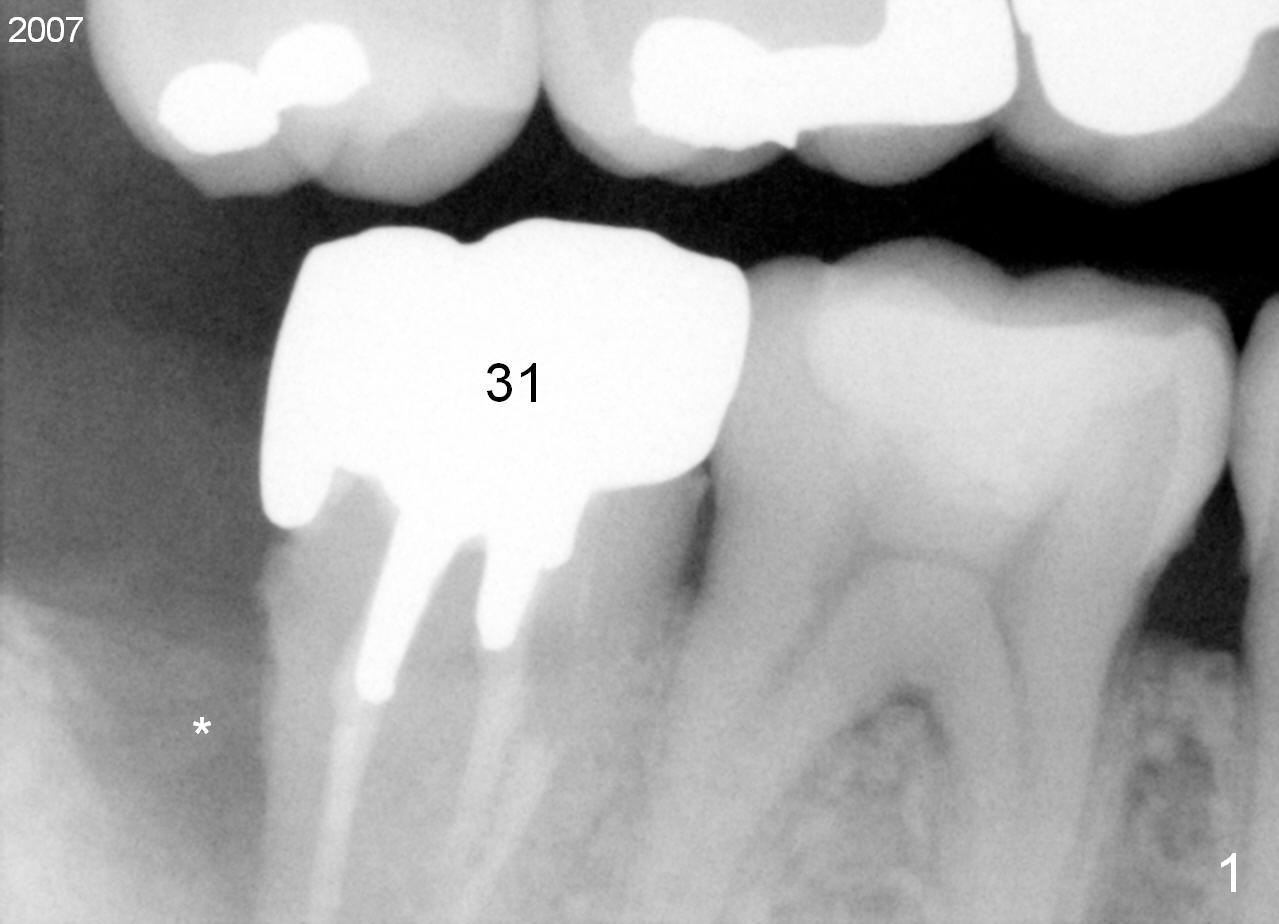
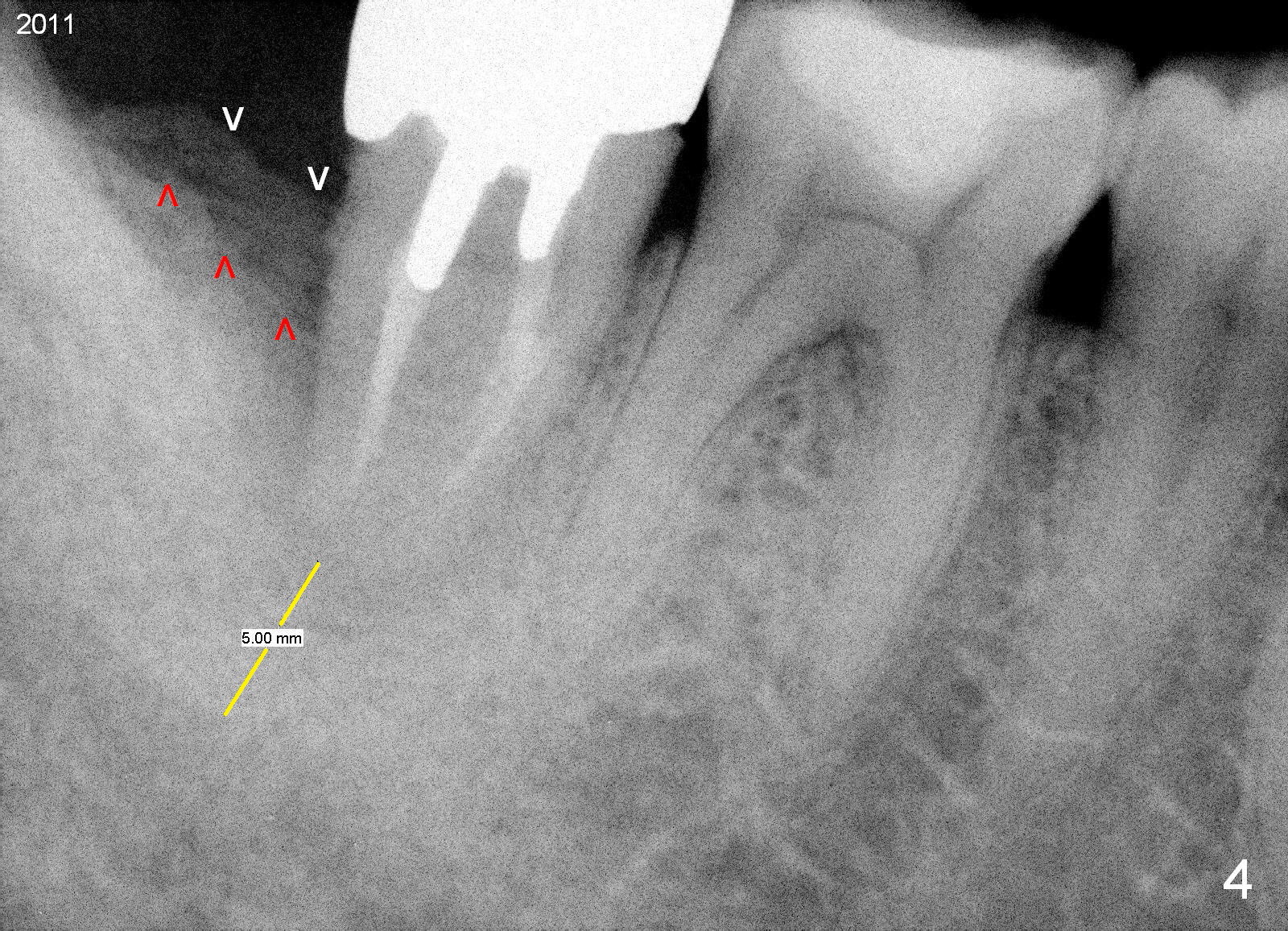
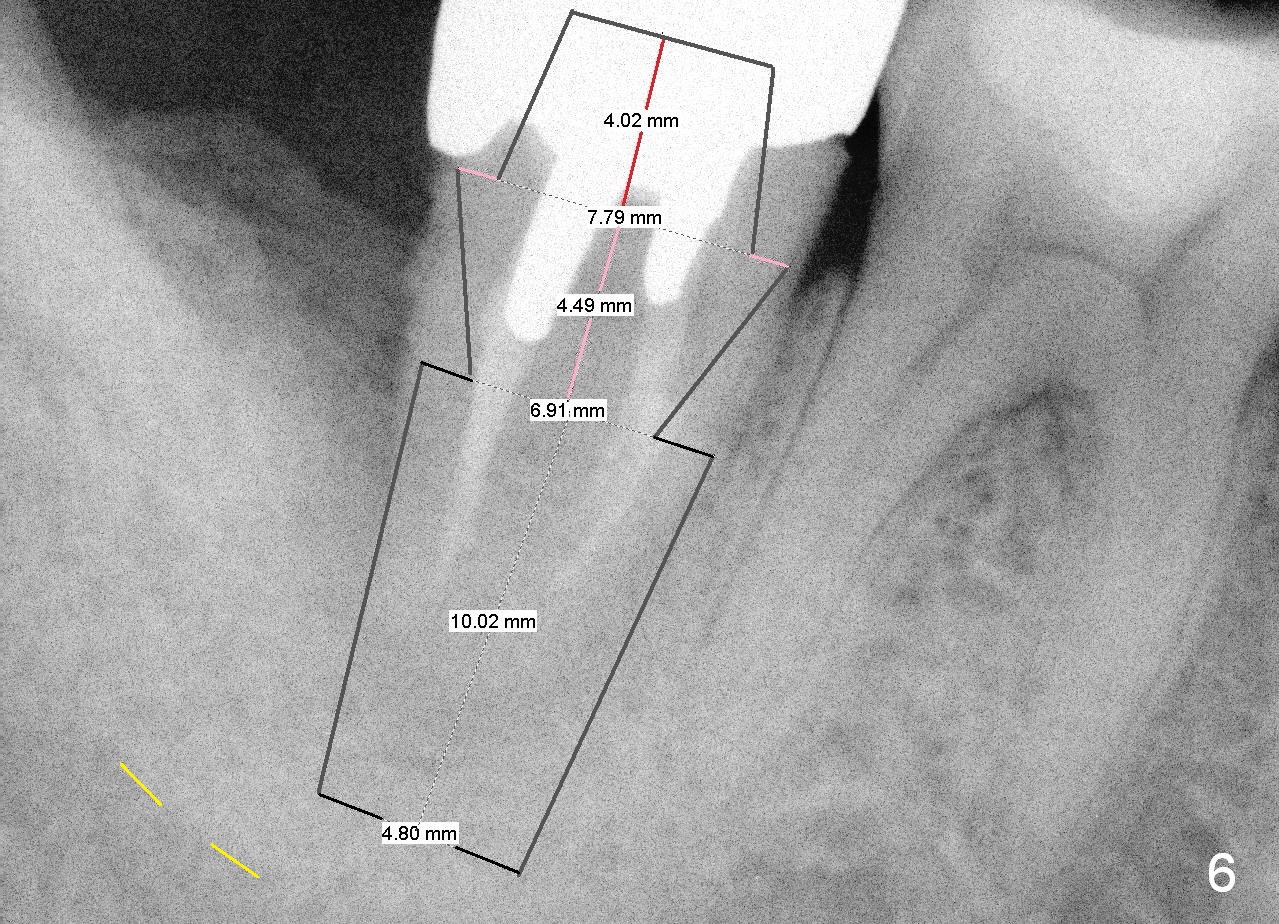
A 44-year-old man has had an asymptomatic distal defect of the tooth #31 for 8 years (Fig.1-5). Recently there is an acute episode of swelling and pain. A fistula develops mesiobucally. Panoramic X-ray films tend to show that the distal defect is deep (Fig.2,5; yellow dashed line: upper border of the Inferior Alveolar Canal). In addition, the distal defect may be not even buccolingually, as indicated by white and red arrowheads in Fig.3,4. Following placement of a 6.9x10 mm bone-level implant, a 7.8x4 (4.5) mm cemented abutment is inserted for try in (Fig.6). When it is fit, it is removed and a cover screw is temporarily placed. A piece of Osteotape (~10x4 mm) is placed distobuccally or distolingually (depending upon which wall is lower). A small amount of bone graft is packed between the most coronal portion of the implant and the Osteotape. The cover screw is then removed and the abutment is re-inserted and tightened by hand. An immediate provisional is fabricated with well-trimmed margin. Reline is done if necessary for securely holding bone graft in place. A new PA is to be taken prior to surgery to determine the extent of the lesion. Photos are taken to show the mesiobuccal fistula. Return to Lower Molar Immediate Implant Xin Wei, DDS, PhD, MS 1st edition 04/12/2015, last revision 05/25/2018