


|
|
|
|
|
|
|
|
|
|
|
|
|
|
Seeking Better Trajectory and More Bone Contact
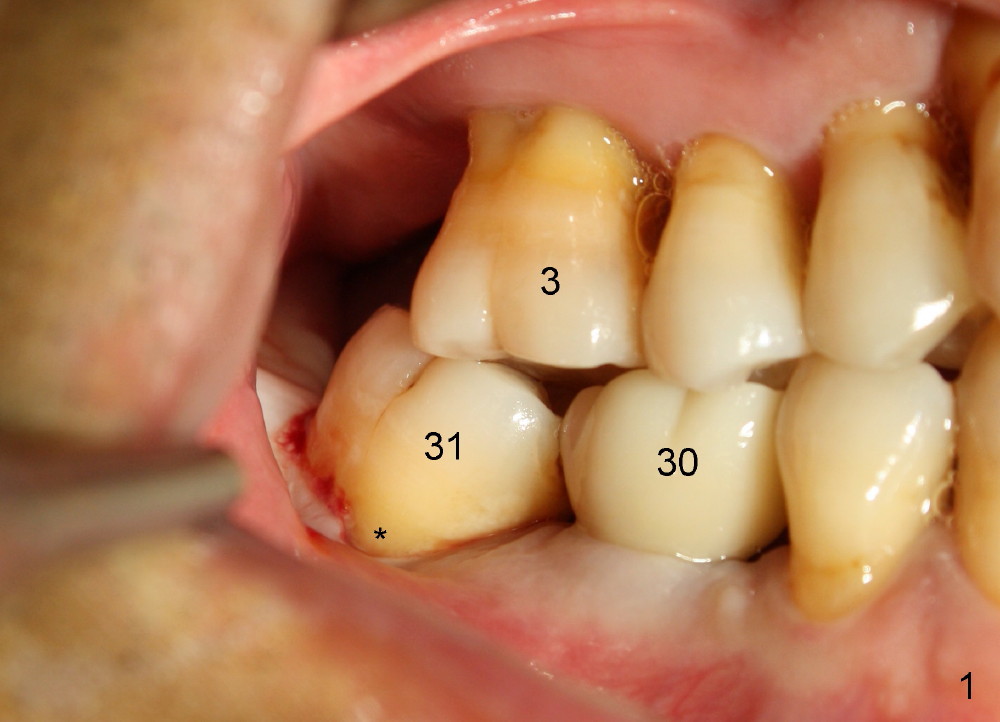
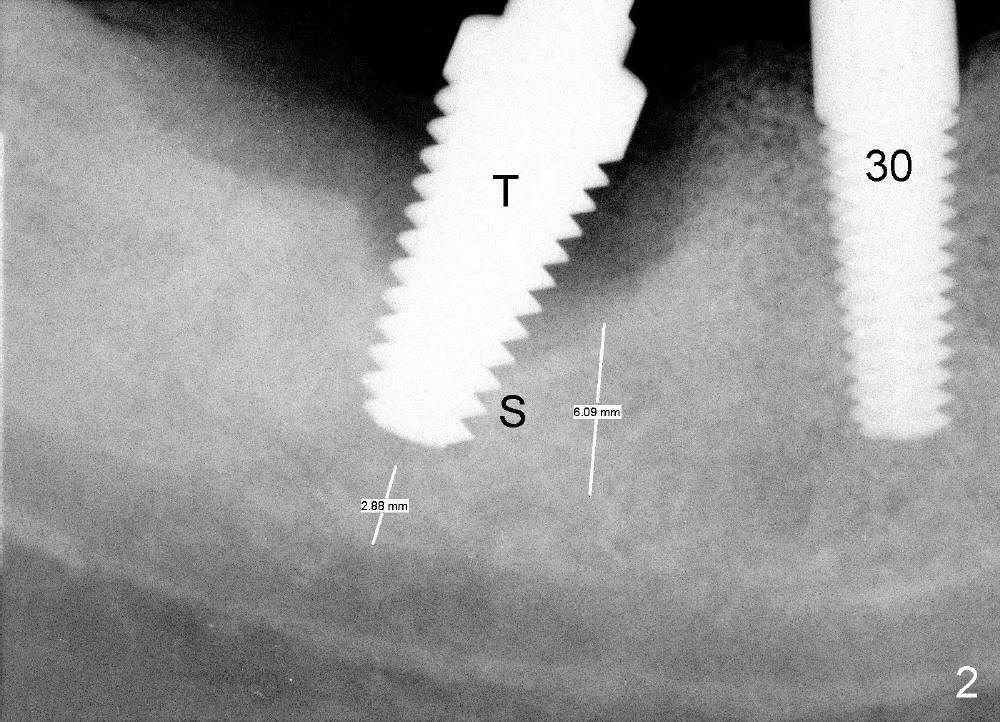
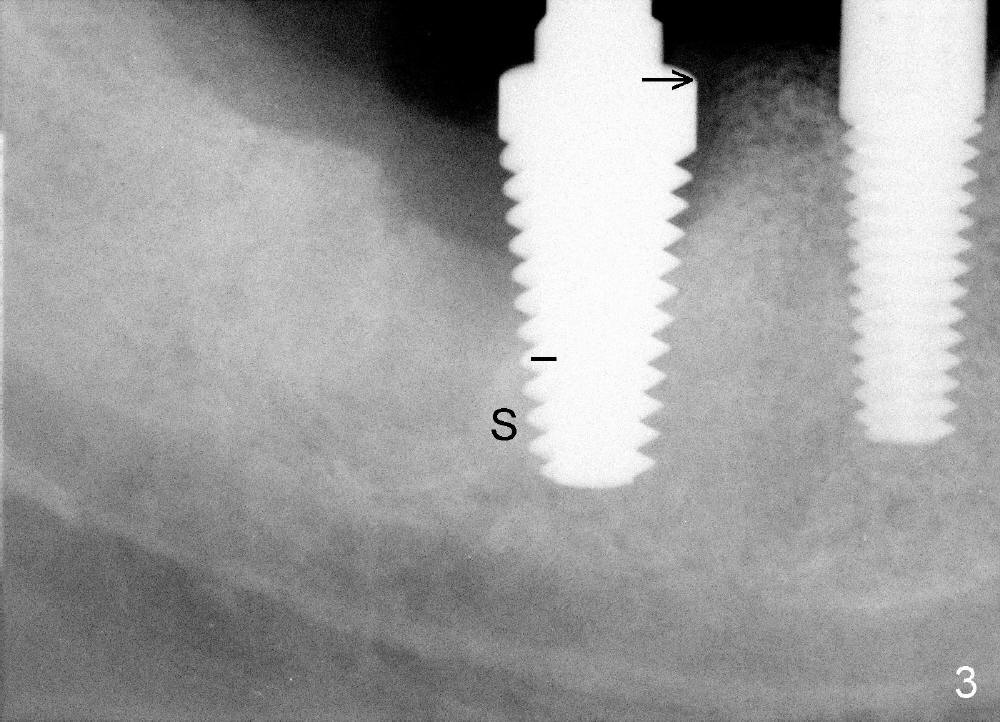
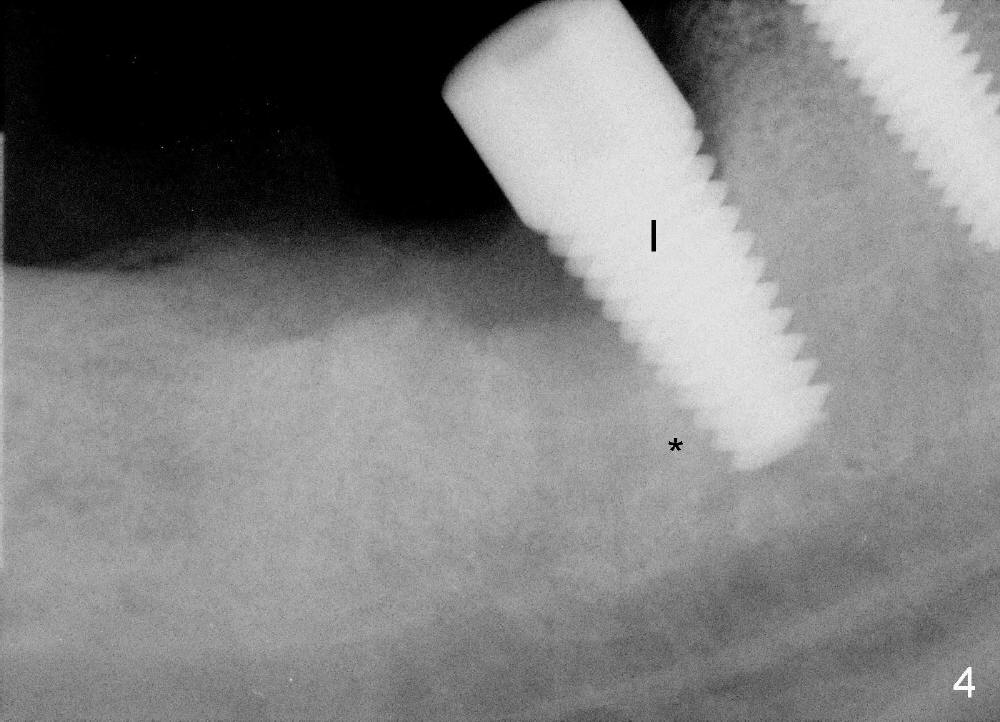
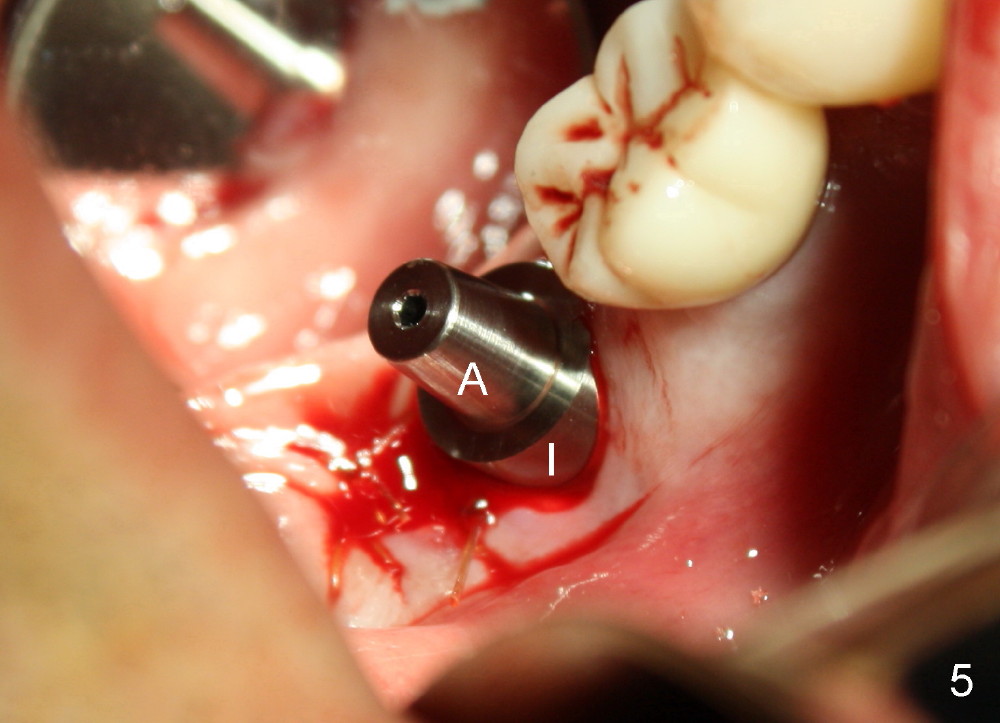
The patient wants to extract the tooth #31, which occludes obliquely with #3 (Fig.1). Immediately after extraction, the osteotomy is intended to be established in the mesial socket, but ends up in the distal one with tilting (Fig.2 (T: tap)). More bone height appears to be obtained in the mesial socket than in the distal one (S: septum, compare two white lines). In fact better trajectory and more bone contact is achieved once the osteotomy is made in the mesial socket (Fig.3). A 7x17 mm gingiva-level implant (Fig.4 I) is placed with insertion torque > 60 Ncm (*: septum). Following bone graft and membrane placement, the distal socket is sutured; the implant is exposed more in the buccal aspect (Fig.5,6) in part due to pre-existing gingival recession (Fig.1 *). An abutment (A) is temporarily placed to hold perio dressing in place.
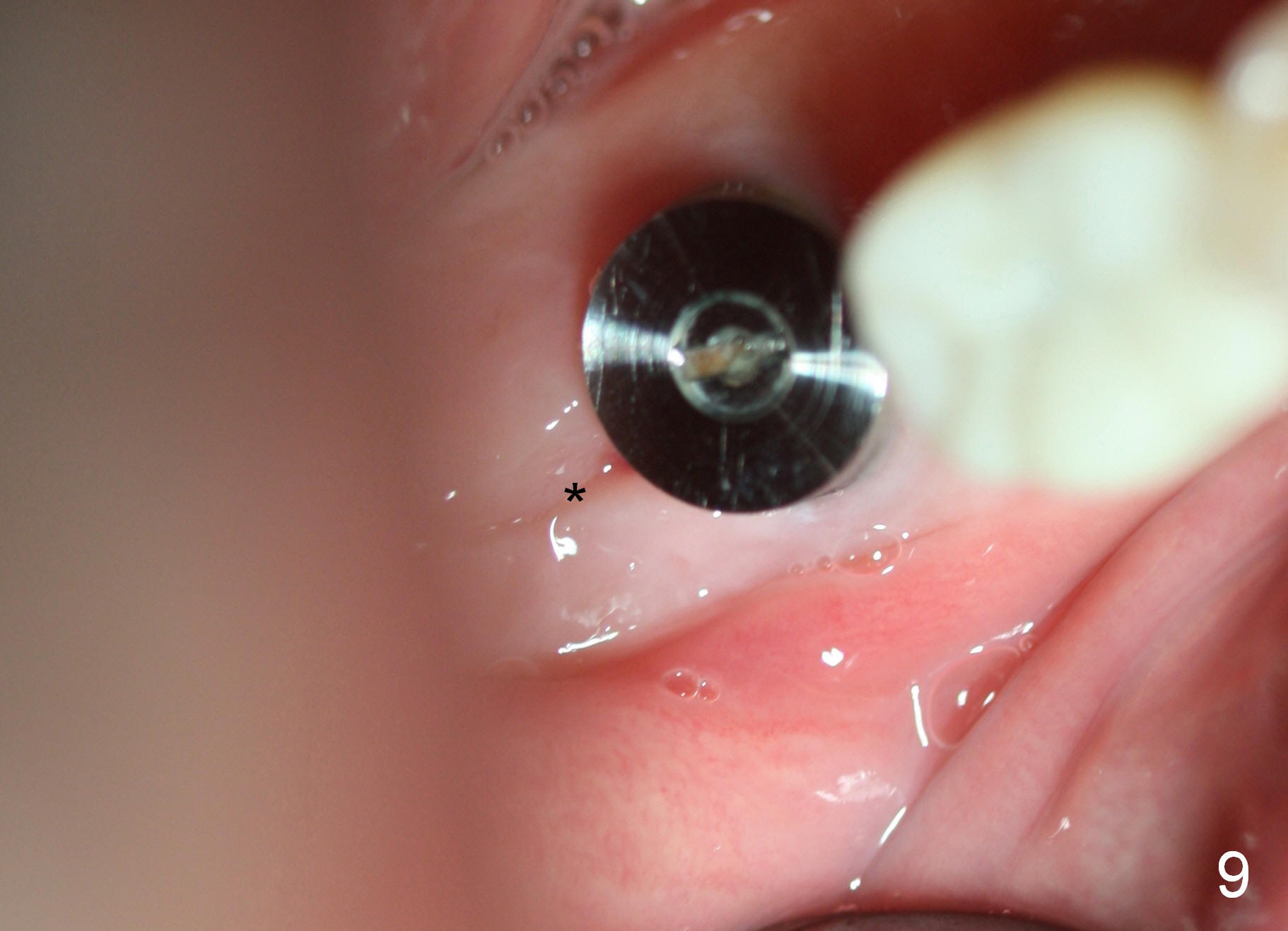
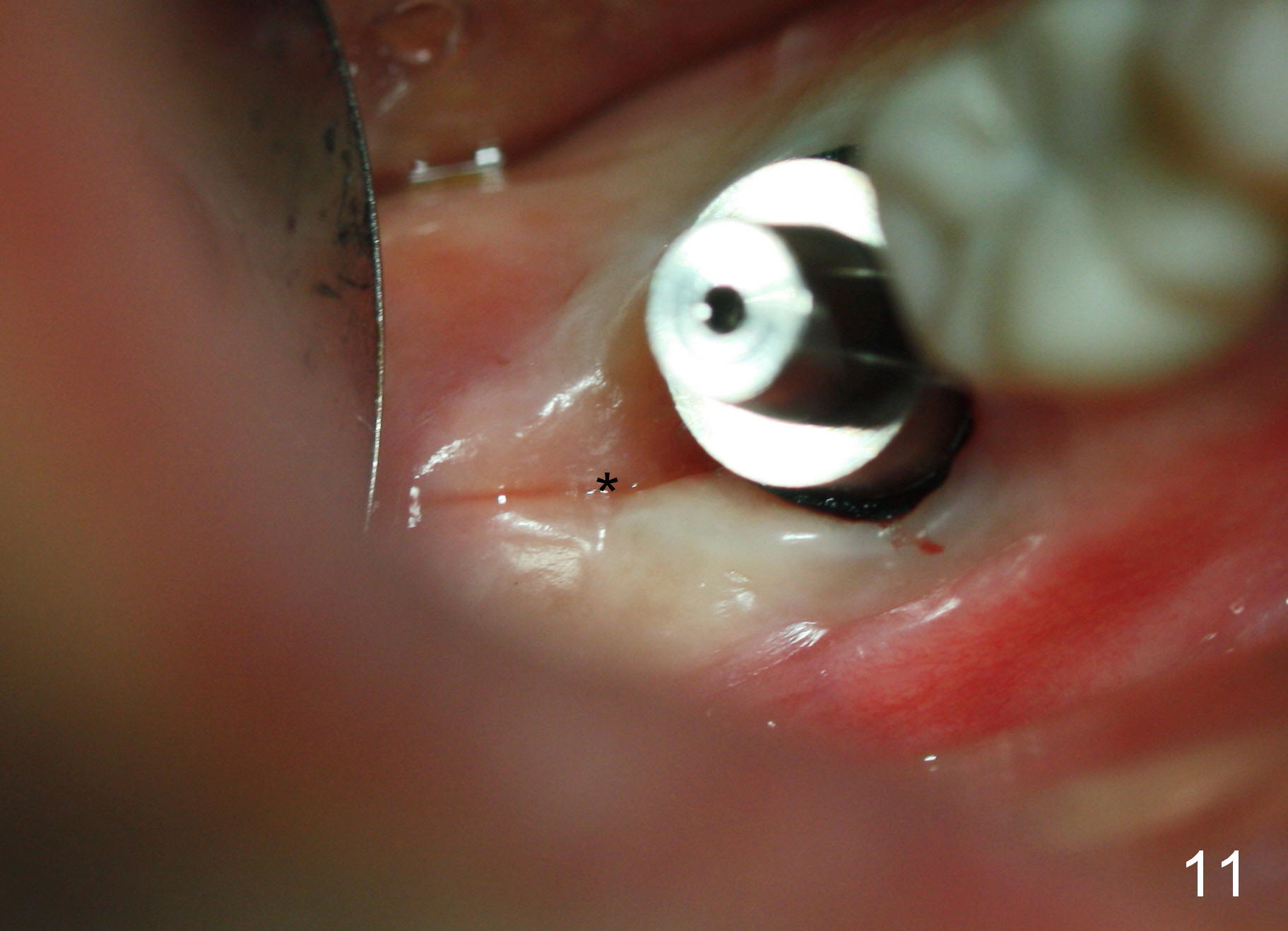
The patient returns asymptomatic 12 days postop (Fig.7,8). There is no excessive buccal gingival recession. The minor distal socket exposure (*) should heal normal shortly. In fact, the distal socket has healed 3 and 4 months postop (Fig.9,11 *), while bone graft (Fig.10 *) has apparently grown into the distal coronal implant threads (>). These two implants are parallel to each other. Periimplantitis develops 11 months post cementation.
Return to Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 10/21/2014, last revision 02/12/2016