

|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
Redo Immediate Implant
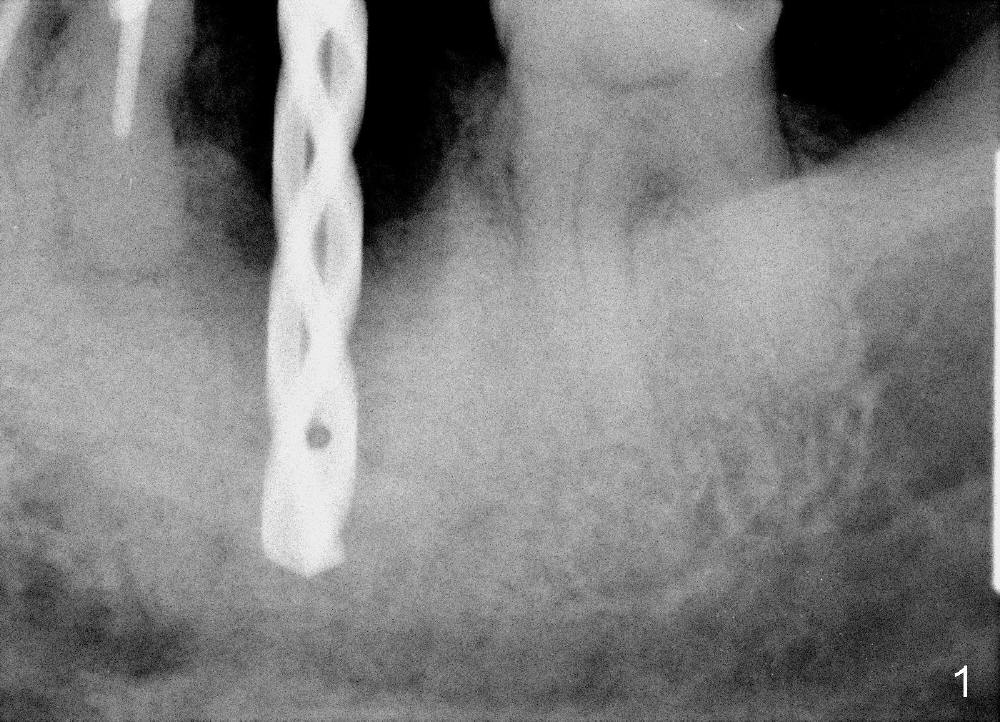
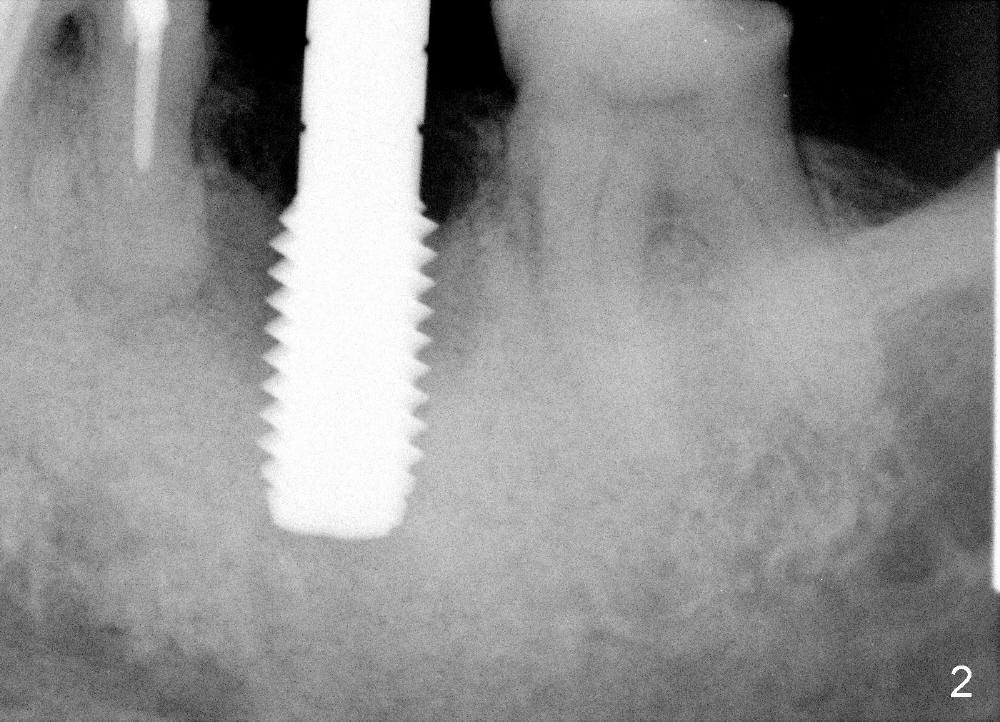
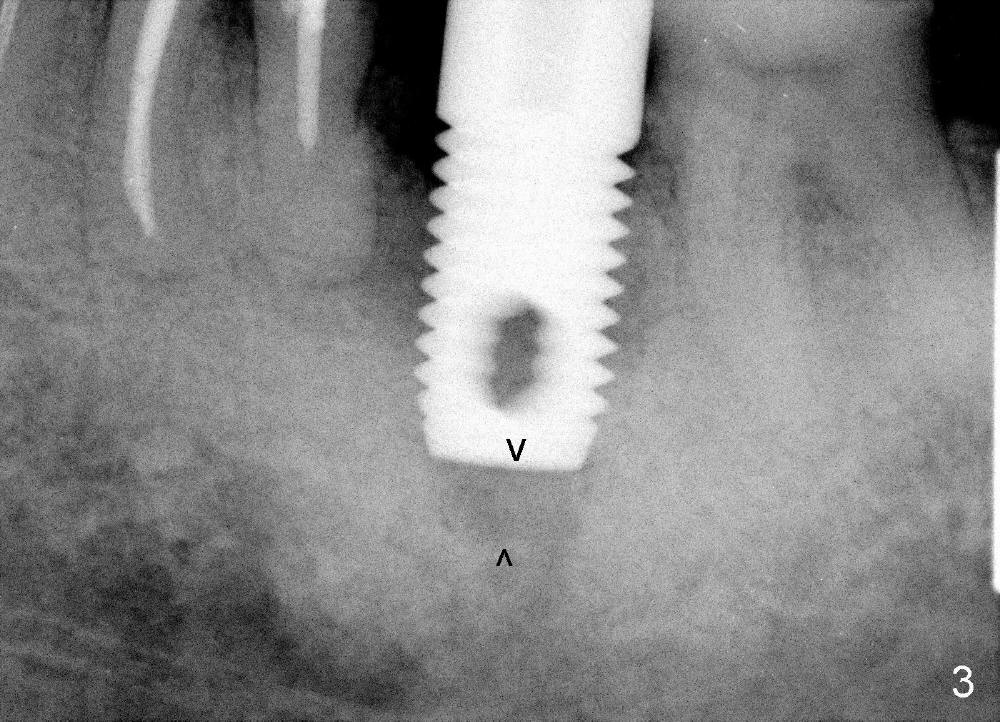
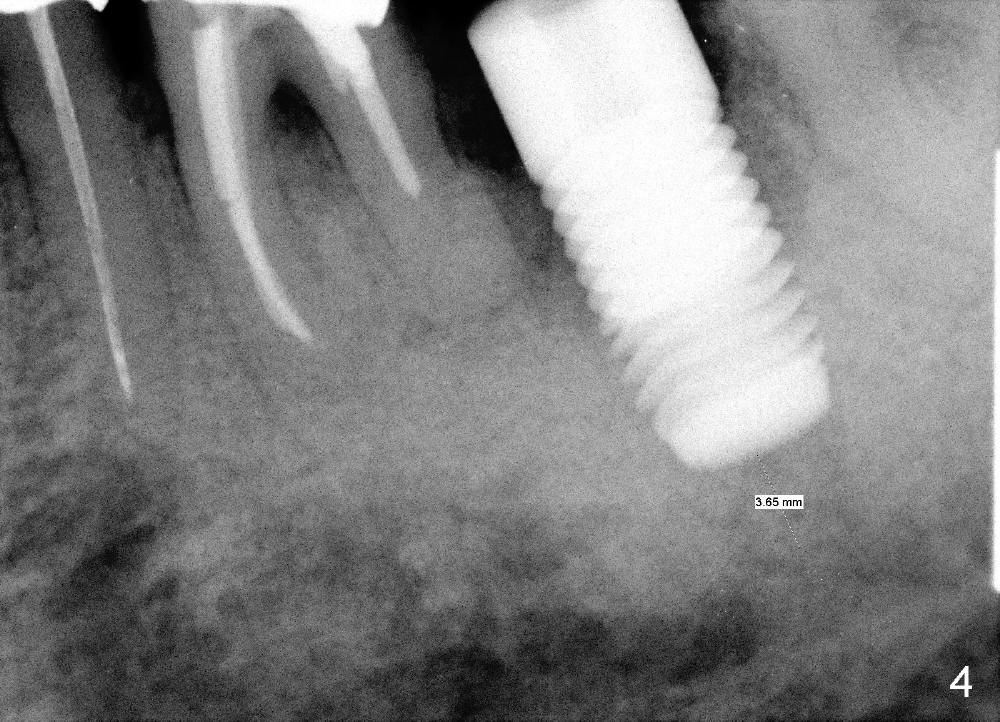
Suddenly several teeth of a 84-year-old man breaks down (#13-15 FPD, #29,30 single units). The implant at the site of #18 has mobility. It appears to be the best to redo immediate implant. The existing 7x17 mm tapered implant is removed without difficulty. The socket walls are basically intact. The socket is debrided with removal of bone graft, copious irrigation and Clindamycin soaking. Osteotomy depth is increased approximately 4 mm (Fig.1) with 2.5-4.5 mm drills. A 6 mm round tap is inserted 3 mm less than expected (Fig.2). The osteotomy is enlarged with 4.9 and 5.9 mm drills at the depth of 17 mm. A 7x17 mm cylindrical implant does not reach the depth of 17 mm (Fig.3). A 8x17 mm tapered tap is inserted relatively easy, but with marginal stability. The osteotomy is then repeatedly enlarged with 5, 5.5 and 6 mm reamers at slightly more than 17 mm. Finally the 7x17 mm straight implant is placed at a desirable level with insertion torque more than 60 Ncm (Fig.4). The top of the implant is equigingival, whereas the apical end is ~ 3 mm from the inferior alveolar canal. It appears that a 7x20 mm straight implant may be too long.
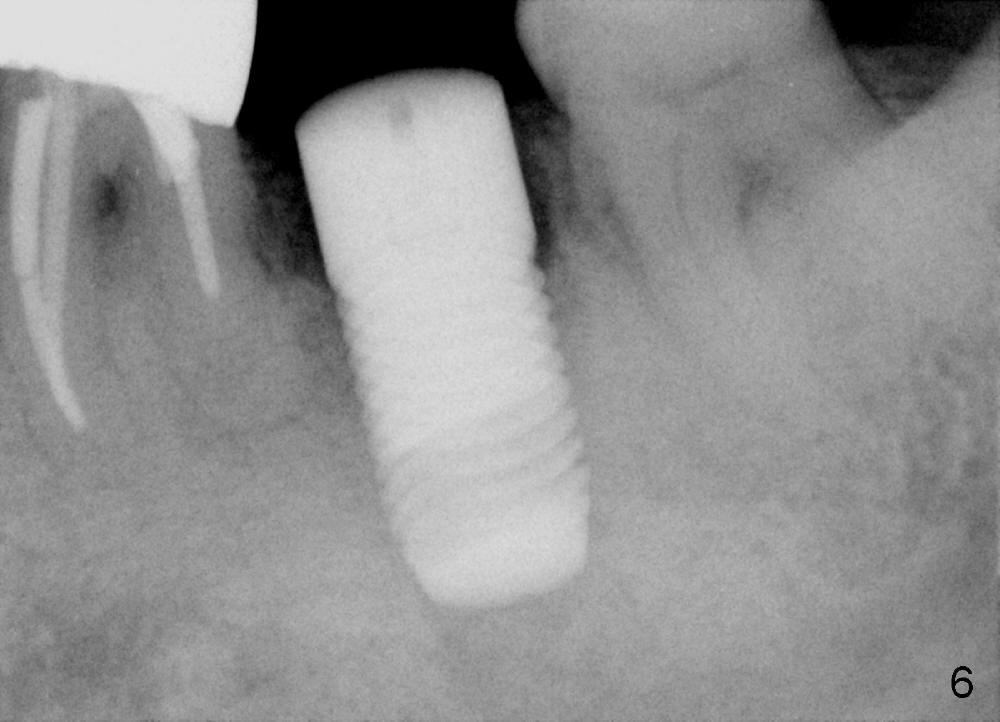
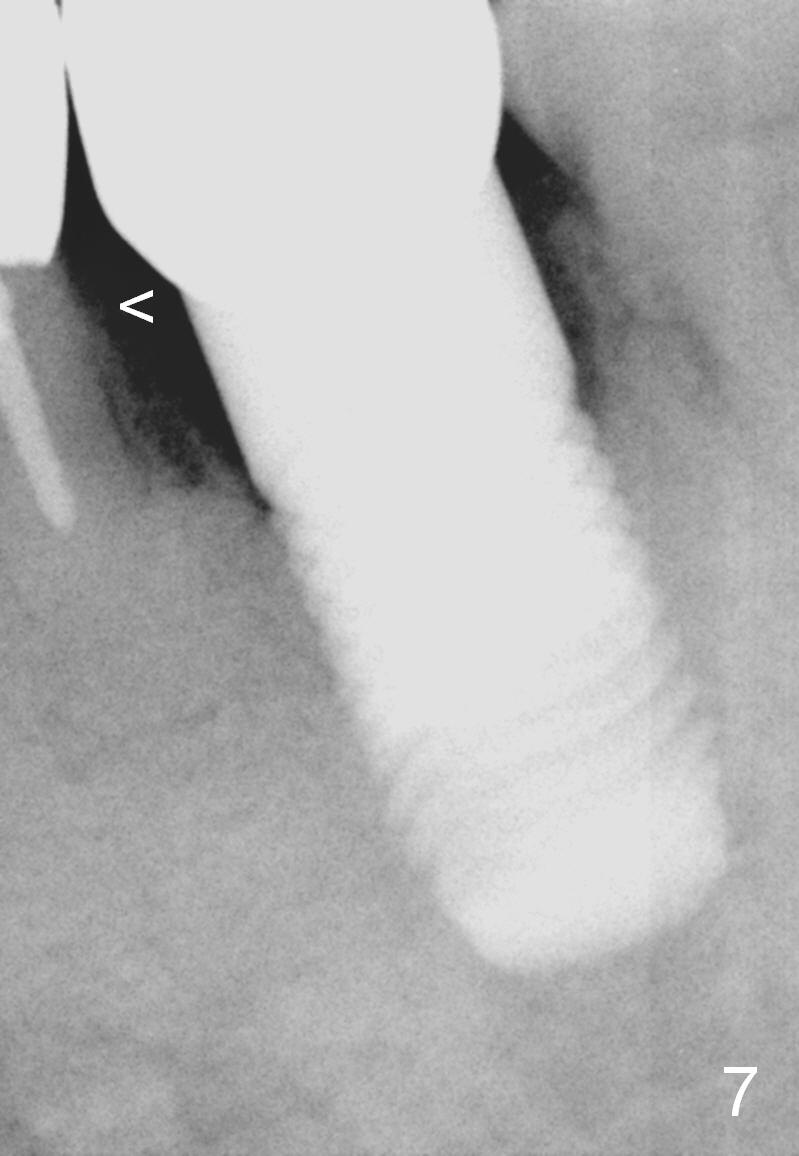
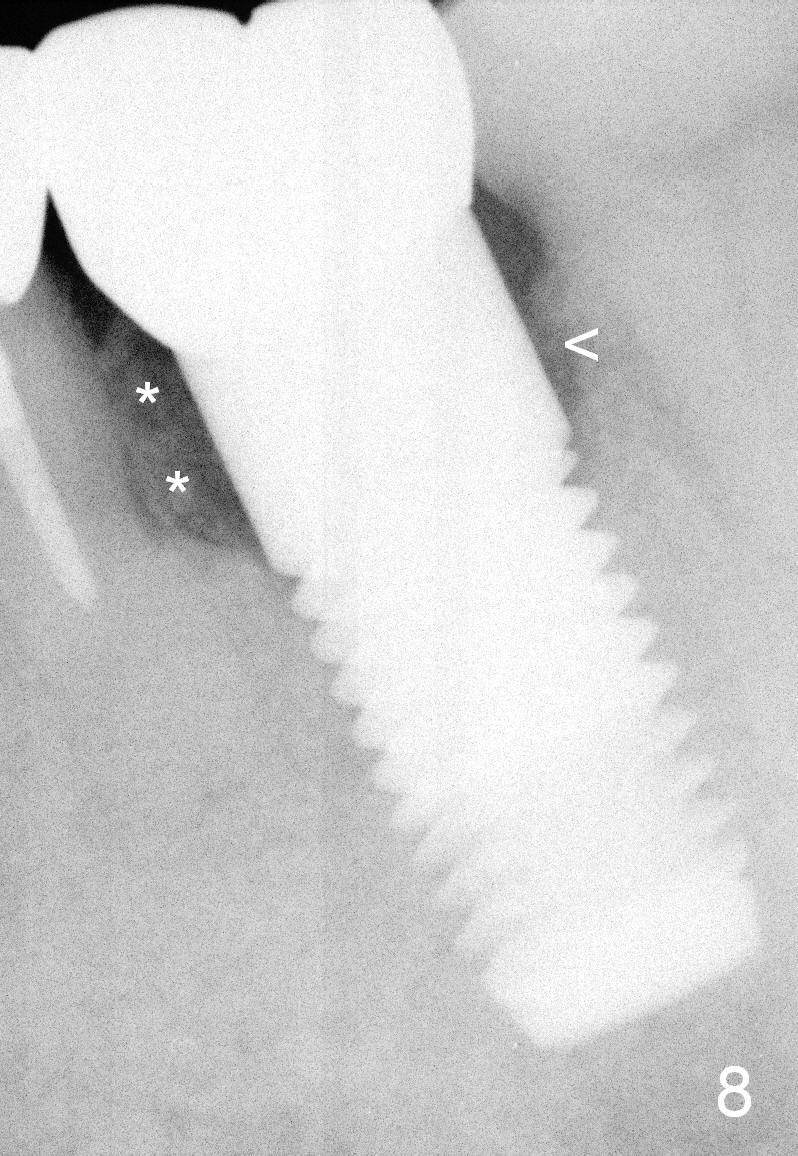
The implant remains stable 3 months post 2nd immediate placement (Fig.5,6). A permanent crown is cemented 7 months postop. The crestal bone between #18 and 19 has started to grow coronally 2 months post cementation (Fig.7 <) and continues to do so 4 months post cementation (Fig.8,9 *).
Return to Professionals, Lower Molar Immediate Implant, When An Implant Fails
Xin Wei, DDS, PhD, MS 1st edition 05/01/2014, last revision 04/14/2015