|
|
|
|
|
|
|
|
|
|
|
|
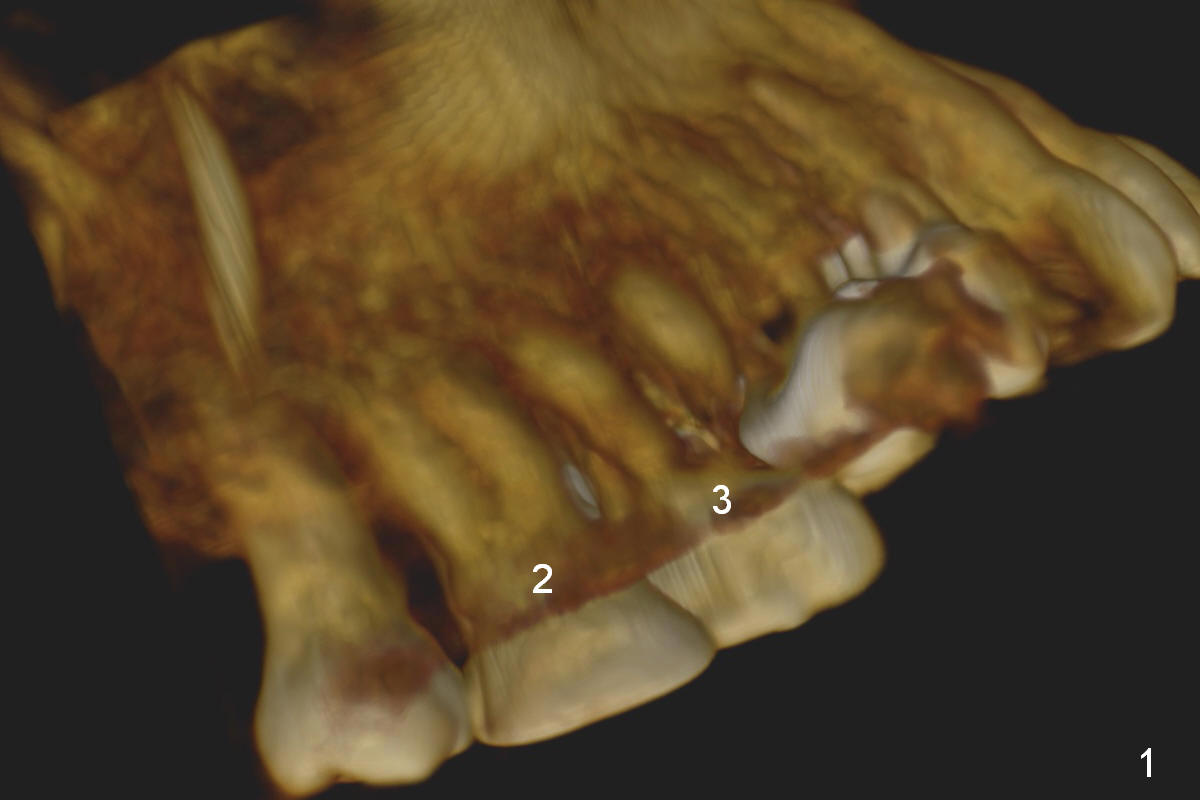
Surgical Intrusion
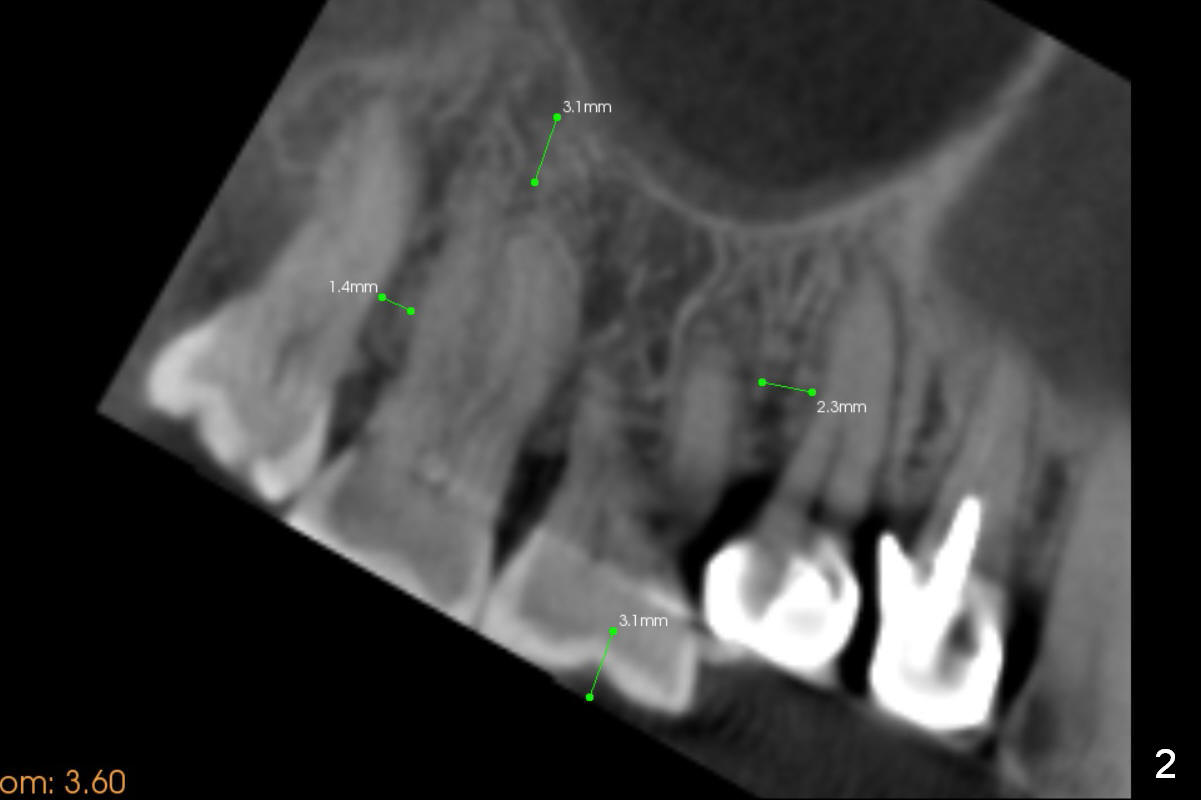
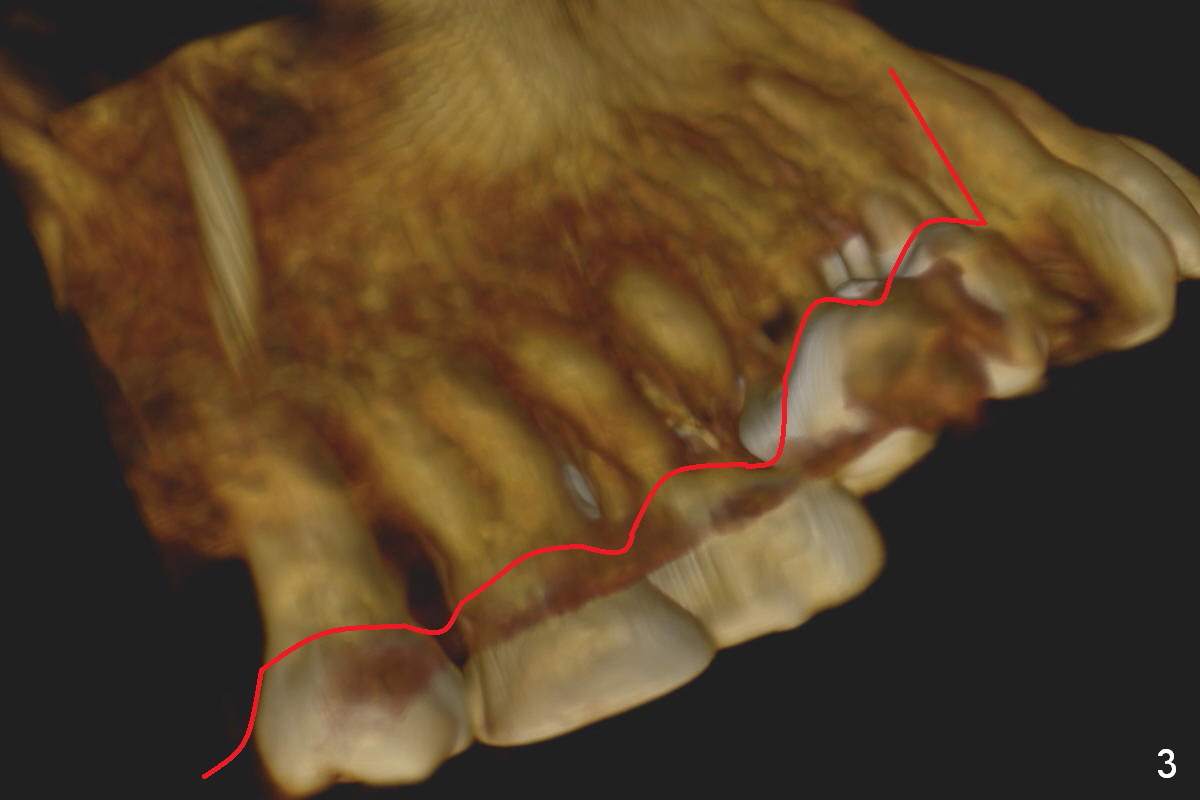
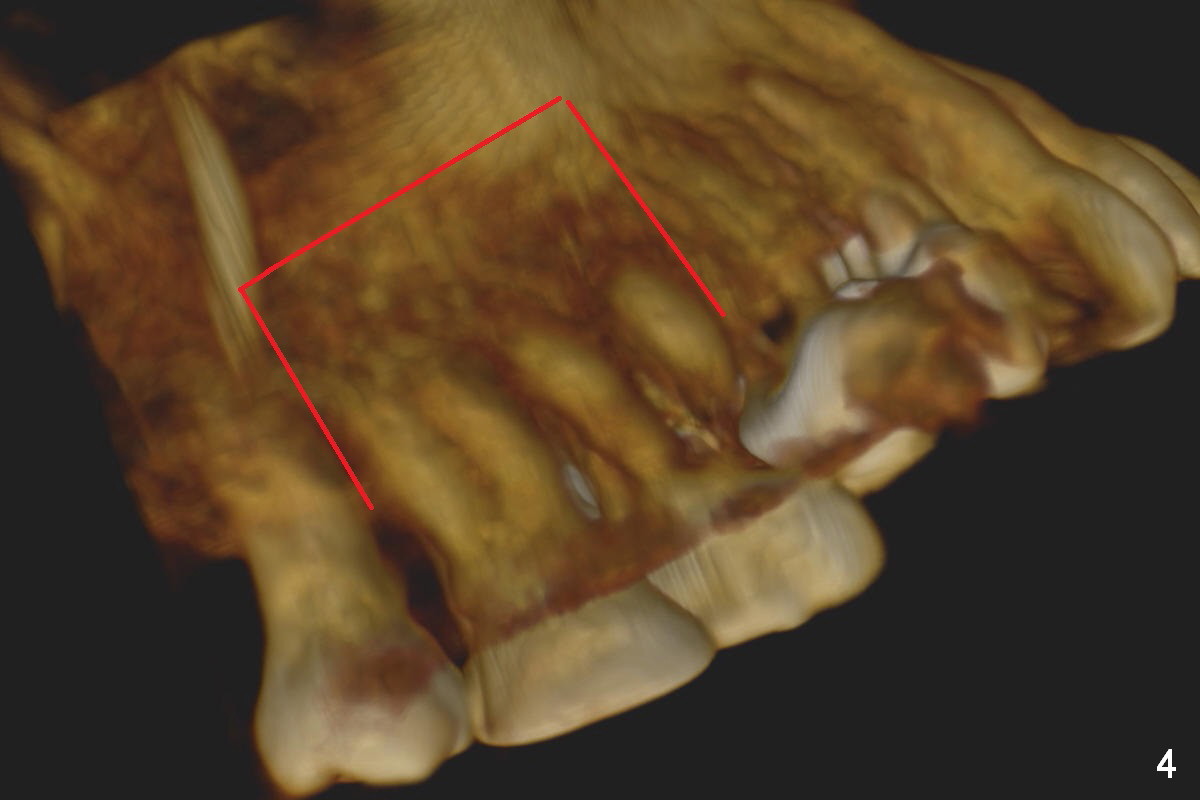
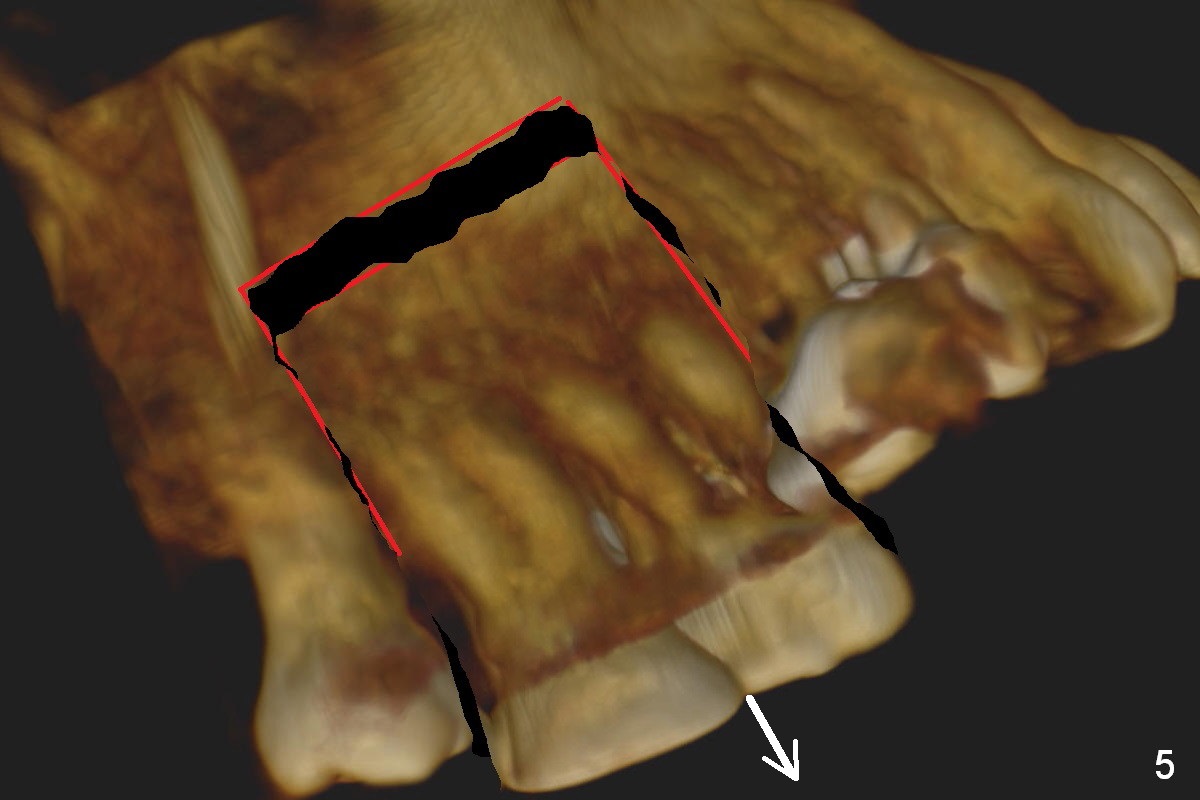
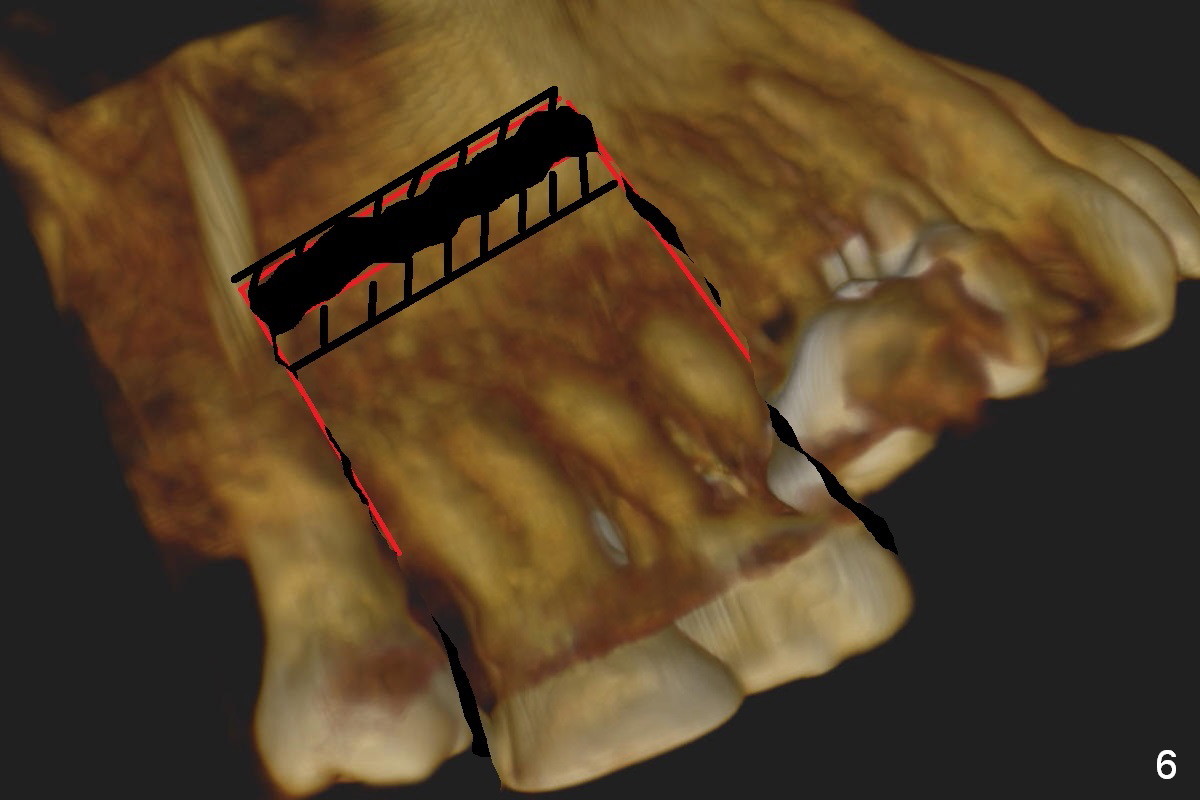
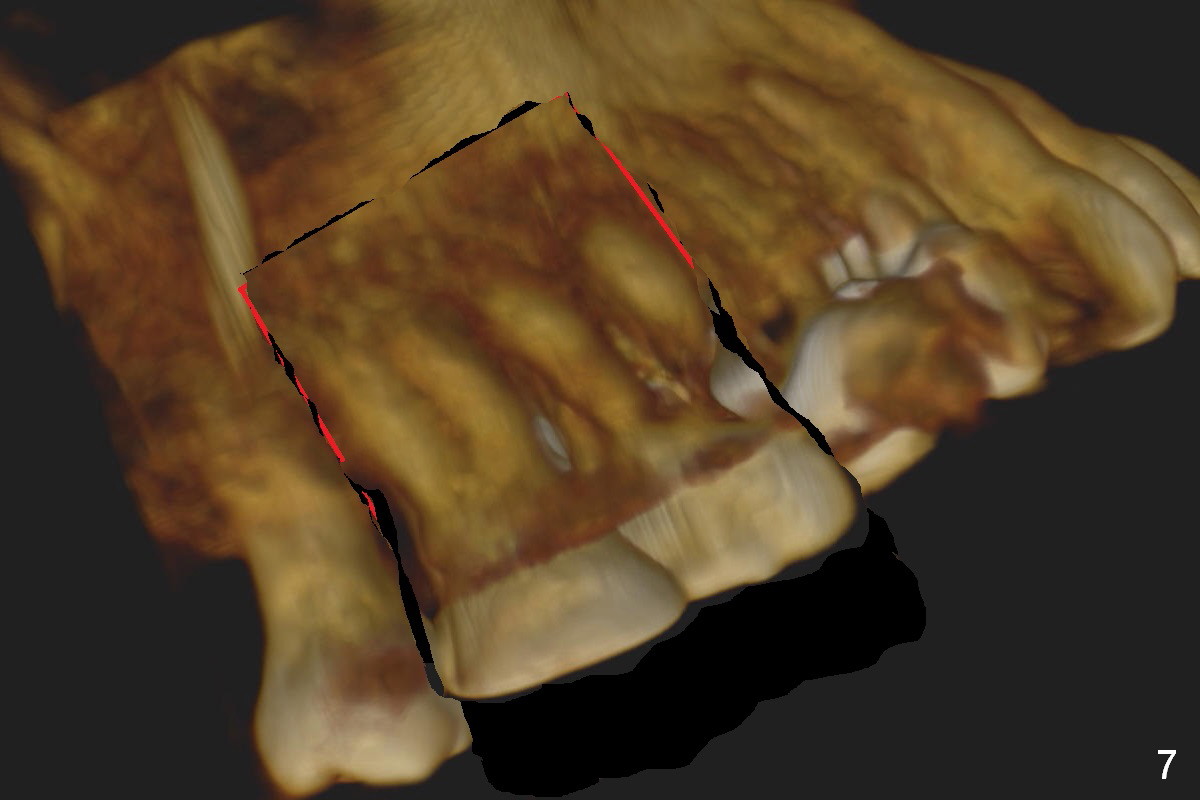
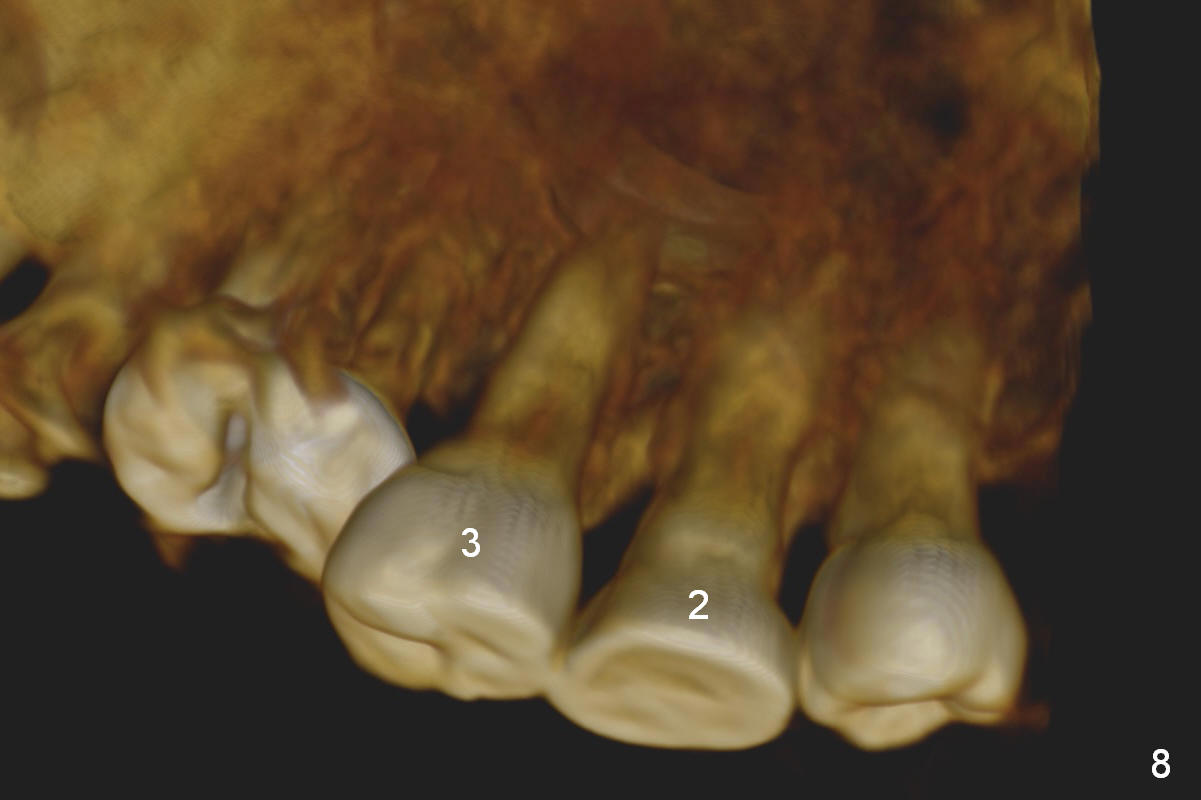
Orthodontic intrusion with mini-implants does not seem to work. When segmental brackets and bands are supplemented, the neighboring tooth (#14) becomes loose. CBCT 3 D and sagittal section show ~3 mm supraeruption of the teeth #2 and 3 (Fig.1,2). Diagnostic wax up demonstrates that the teeth #2 and 3 need to be intruded for 4 and 2 mm, respectively. Buccal gingival sulcus and anterior oblique incisions are shown in Fig.3 (red line). Osteotomy will be made with surgical fissure bur and chisels (Fig.4 red lines). The segment is down fractured (Fig.5 arrow). Apical bone is removed with acrylic bur and/surgical burs (Fig.6 cross lines). The segment is elevated and checked with a prefabricated splint out of diagnostic wax up. Insert a thicker orthodontic wire into brackets and bands buccally.
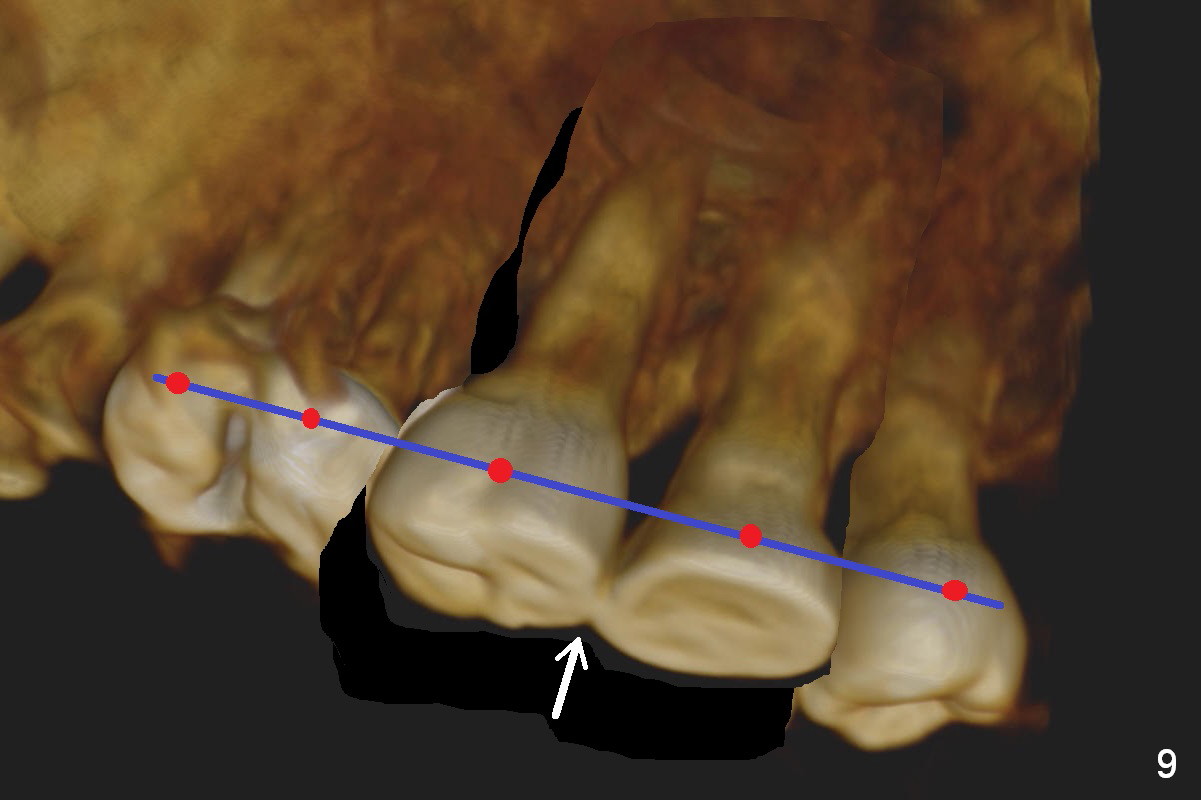
Fig.8 is a preop palatal view of the region. When the segment is lift (Fig.89 arrow), use a twisted wire (lingual retainer; blue line) and composite (red dots) for fixation. The splint may be also used for fixation. On the right, use a thin ortho wire to tighten the splint against mini implants, while on the left, thin ortho wire and composite will be used. The patient will eat soft diet for several months. Keep good oral hygiene.
Return to Lower Arch
Reconstruction
Xin Wei, DDS, PhD, MS 1st edition 02/07/2016, last revision 02/07/2016