
|
|
|
|
|
|
|
|
How Does Low Bone Density Affect Osteotomy?
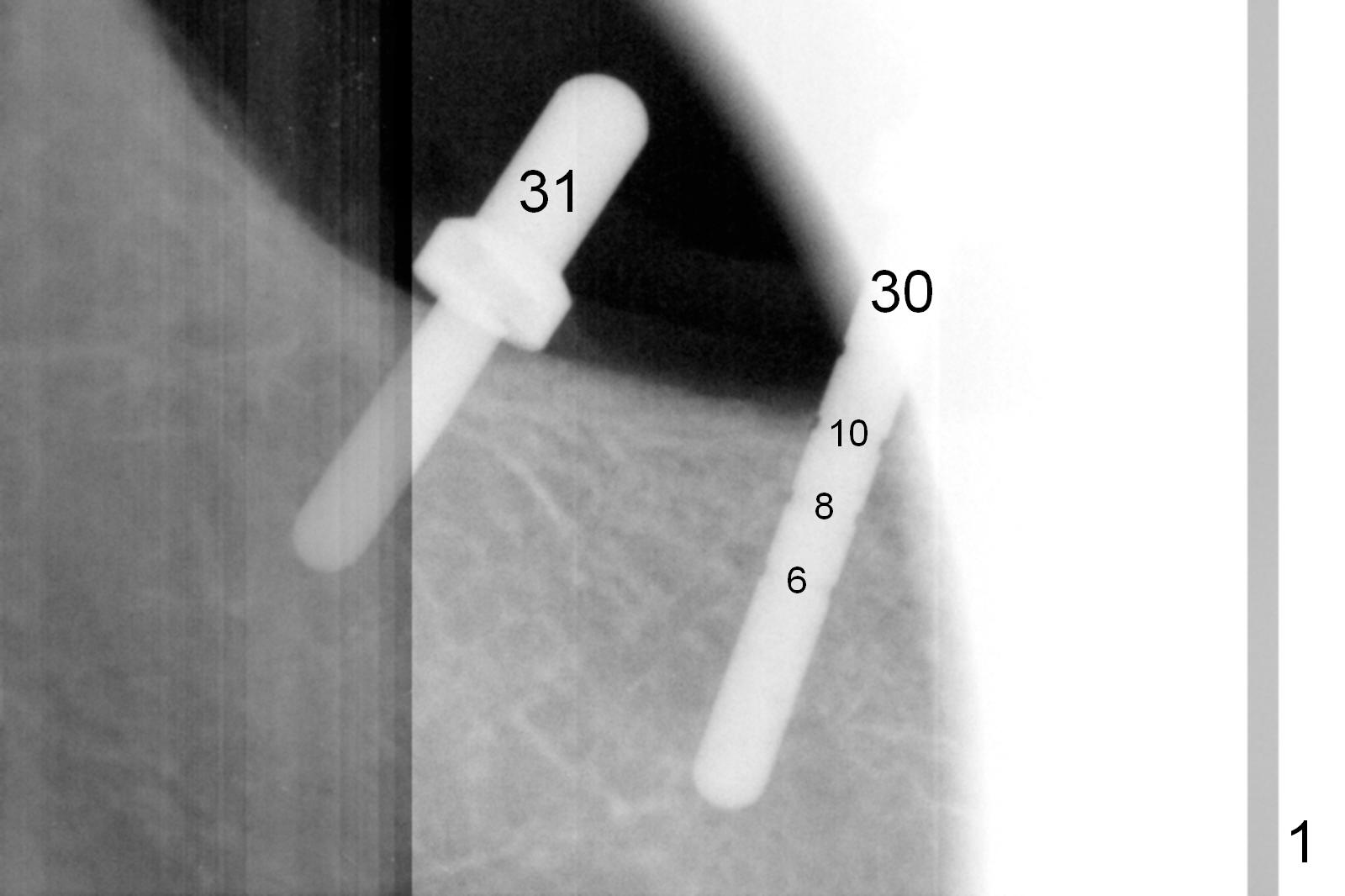
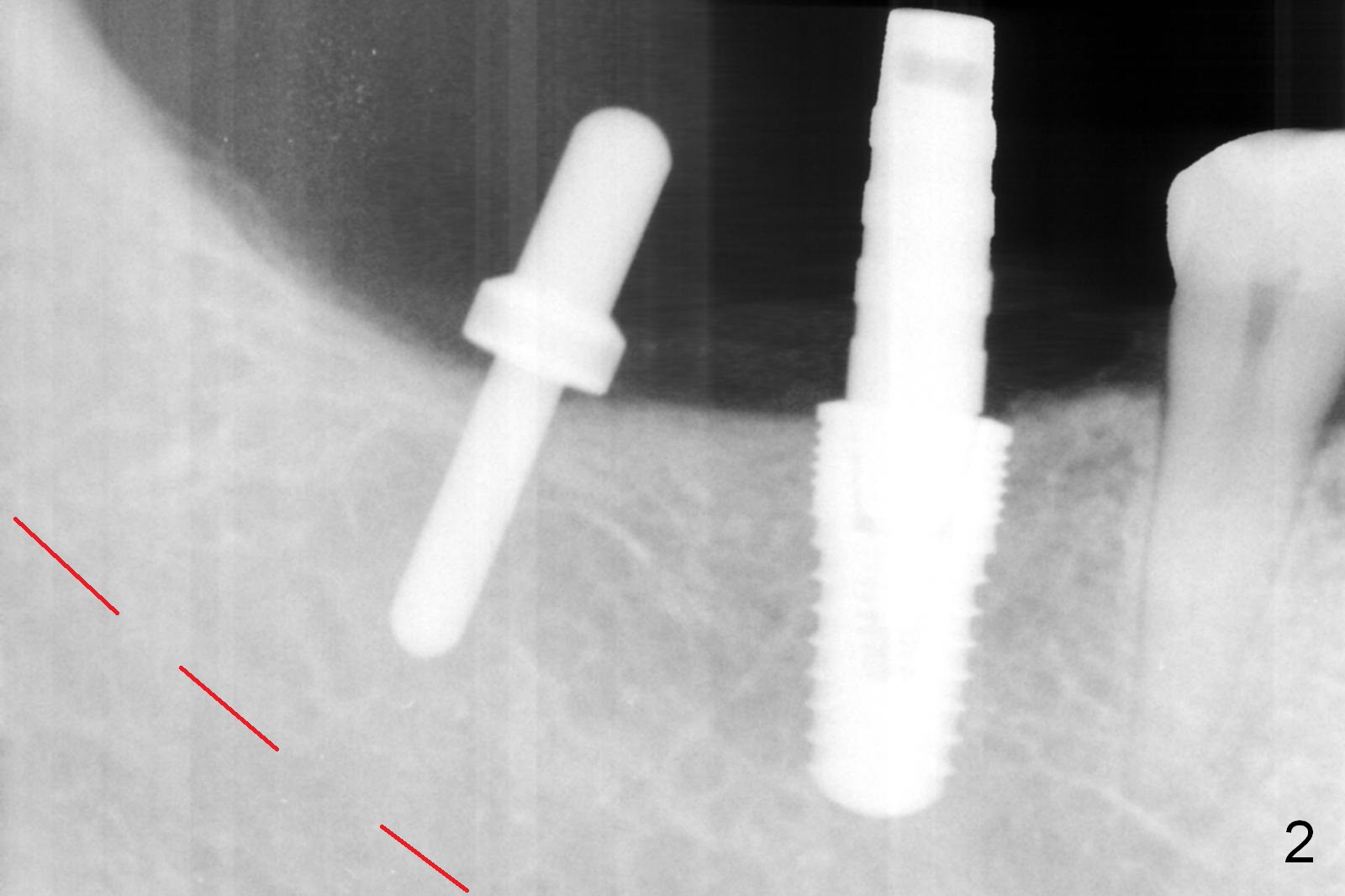
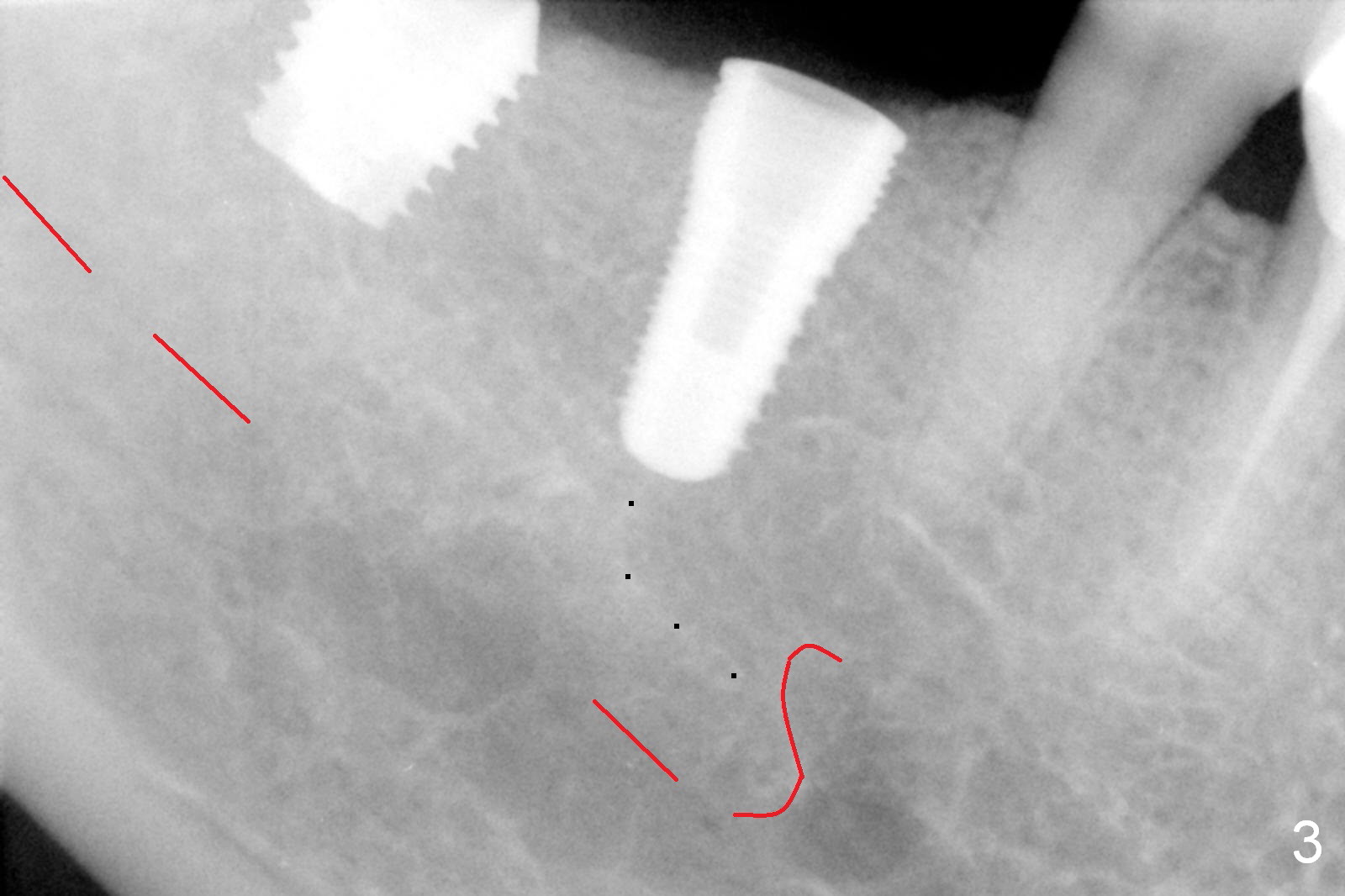
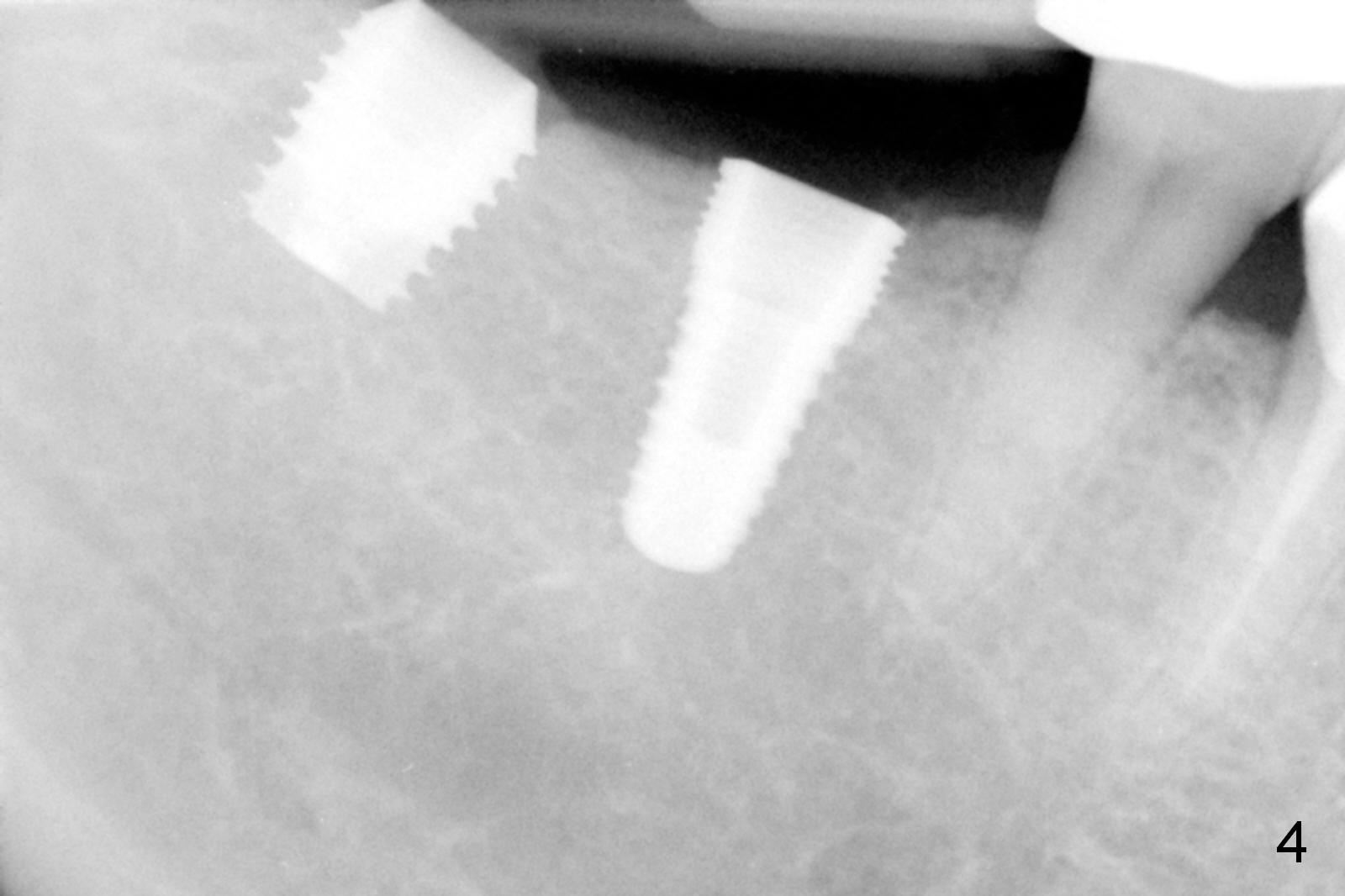
After vacation, the nervous patient returns for #30, 31 implant placement. After infiltration anesthesia, initial osteotomy goes on smoothly at the depth of 10 and 8 mm, respectively (Fig.1). Depth gauge post 5x10 mm drilling shows that the distal osteotomy at #30 is 14 mm in spite of depth control (using drill stopper). Damage the Inferior Alveolar Canal or Mental Loop? Since hemorrhage is moderate, a 5x10 mm submerged implant is placed without discomfort from the patient (Fig.2); when the osteotomy at #31 is being enlarged with 2/2.7 mm pilot drill at 8 mm, the patient experiences severe pain without any obvious reason. The infiltration anesthesia is increased with Articaine and Marcaine. The depth of the osteotomy reduces at 6 mm. The osteotomy and 5.9x6 mm implant placement is done in a slow and gentle manner (Fig.3,4). The bone density mesioapical to the implant at #30 is low (Fig.3 dot line, Fig.5 (CBCT, ≤50 units) *)). This may account for apparent increase in the osteotomy at #30. The soft bone gives in to the depth gauge!
How to explain pain and discomfort of osteotomy and implant placement at #31 in spite of large clearance from the Inferior Alveolar Canal (Fig.3 red dashed line)? Still the low bone density theory. The low bone density (Fig.5 * at #31) makes it easy to transmit the heat and vibration associated with the osteotomy to the underlying nerve!
Return to Lower Arch Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 06/16/2016, last revision 06/16/2016