


|
|
|
|
|
|
|
|
|
|
|
Osteotomy Before Extraction of the Roots
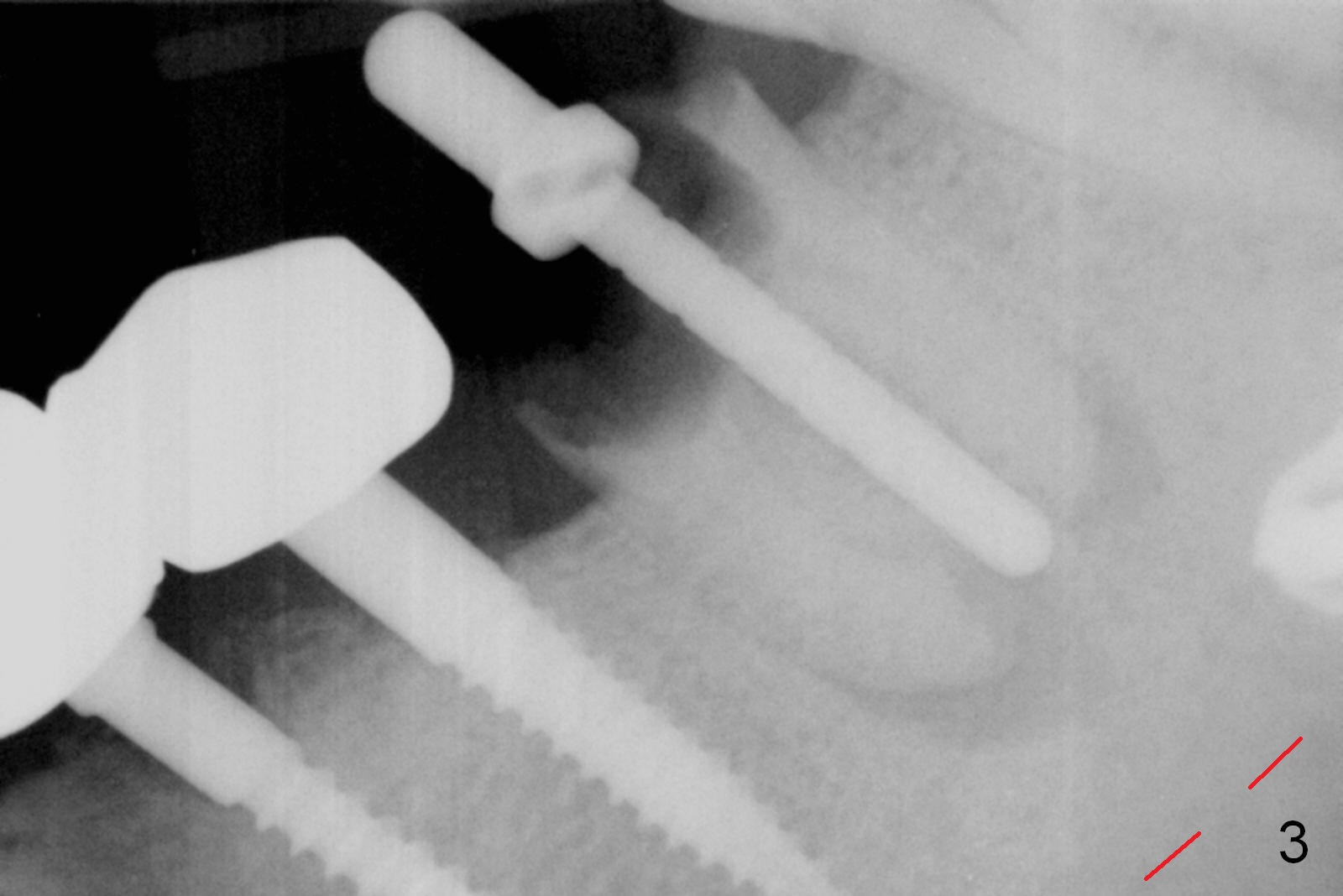
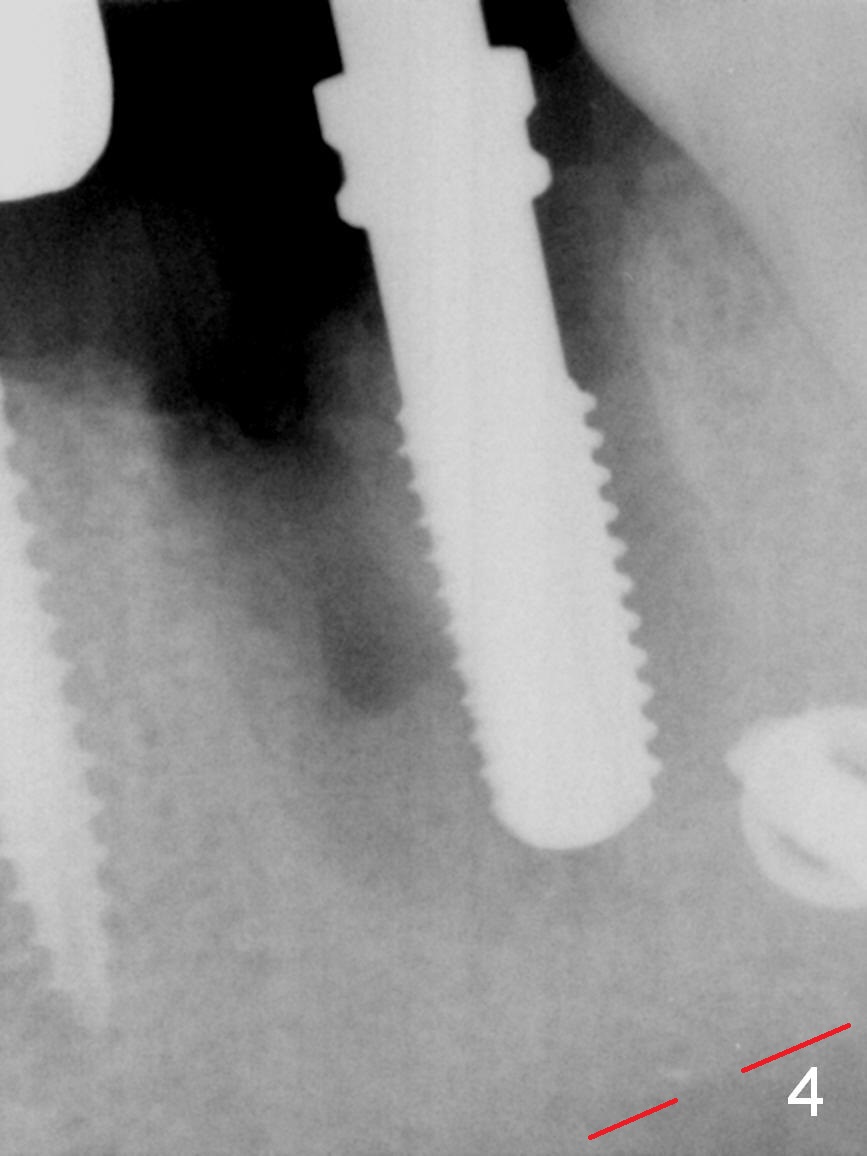
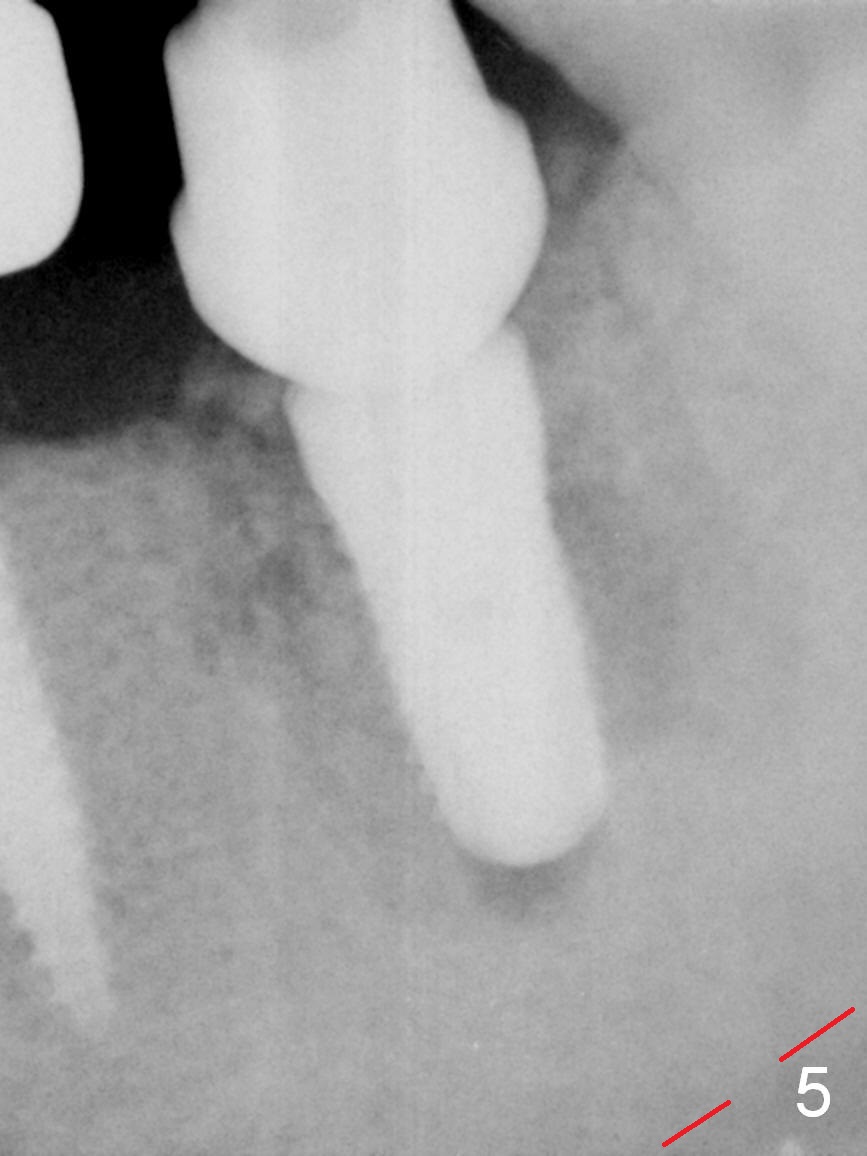
The patient requests extraction and implant because of tenderness when his tongue touches the lingual defect (open margin, Fig.2) of the tooth #19. The tooth fractures upon application of forceps. After flattening the middle portion of the root stump, osteotomy is established through the root with the initial depth 12 mm (Fig.3 (red dashed line: the superior border of the Inferior Alveolar Canal)). Sequential osteotomy is finished until 4.5x14 mm. Autogenous bone and dentin are collected. Then the 3 roots are extracted with difficulty because of dense bone. Apical granulation tissue is removed. Tap drills are used (4.5 and 5 mm). The latter barely achieves stability, being tilted distally while X-ray is being taken (Fig.4). Then the osteotomy depth increases by another 2 mm before placement of 5.3x12 mm implant, 7.8x4(4.5) mm abutment and allograft as well as autogenous bone and dentin (Fig.5). Sutures are placed to hold the displaced buccal flap in place. As usual, an immediate provisional is fabricated to keep bone graft and collagen plug in place.
It seems to be easier to control the position of the osteotomy mesiodistally than buccolingually through the root stump. If CT confirms a wide septum, it would be easier and more precise to establish osteotomy with roots being extracted first.
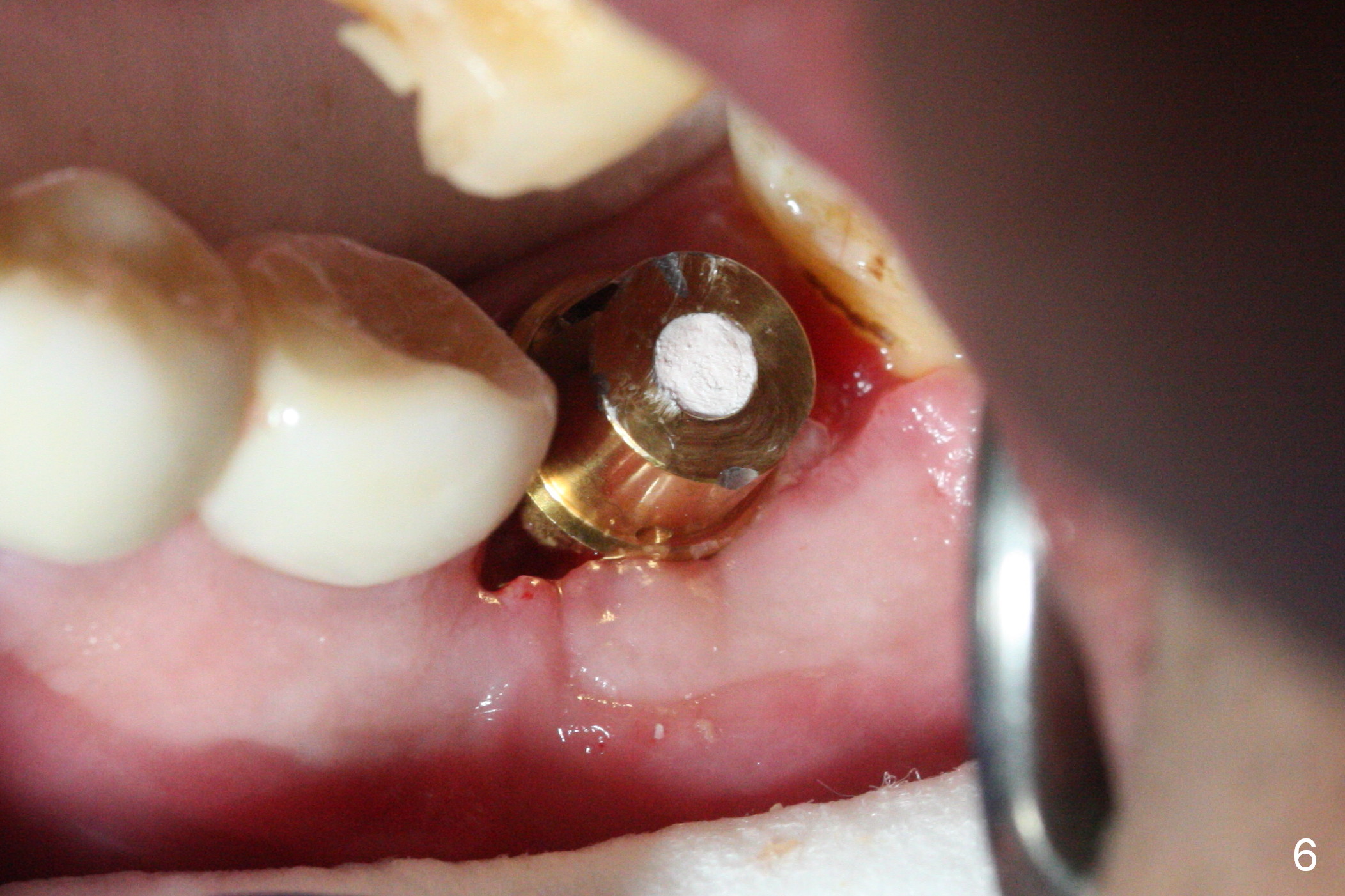
The patient has moderate pain for 4 days postop, probably due to difficult extraction. The socket heals except mesial portion 3 weeks postop, when the provisional is removed for revision. Loose bone graft granules have been washed away from the mesial socket (Fig.6). The implant seems to have osteointegrated 3 months postop (Fig.7). Before restoration, tooth sensitivity associated with #15 severe wear should be treated.
Return to Lower Molar, Arch Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), IBS
Xin Wei, DDS, PhD, MS 1st edition 10/14/2016, last revision 02/05/2017