%20change%20in%20trajectory%20not%20enough,%202x14(4)%20palatal%20plate%20low.jpg)
.jpg)
,%2012%201.5x10,%2013%201.2x8.jpg)
,%2013%202x8.jpg)
.jpg)
,%2012%202.5x10(2),%2013%203x10(2).jpg)







|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
||
|
|
|
|
|||
|
|
|
|
|
||
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
Never Too Late to Change Trajectory of 1-Piece Implant
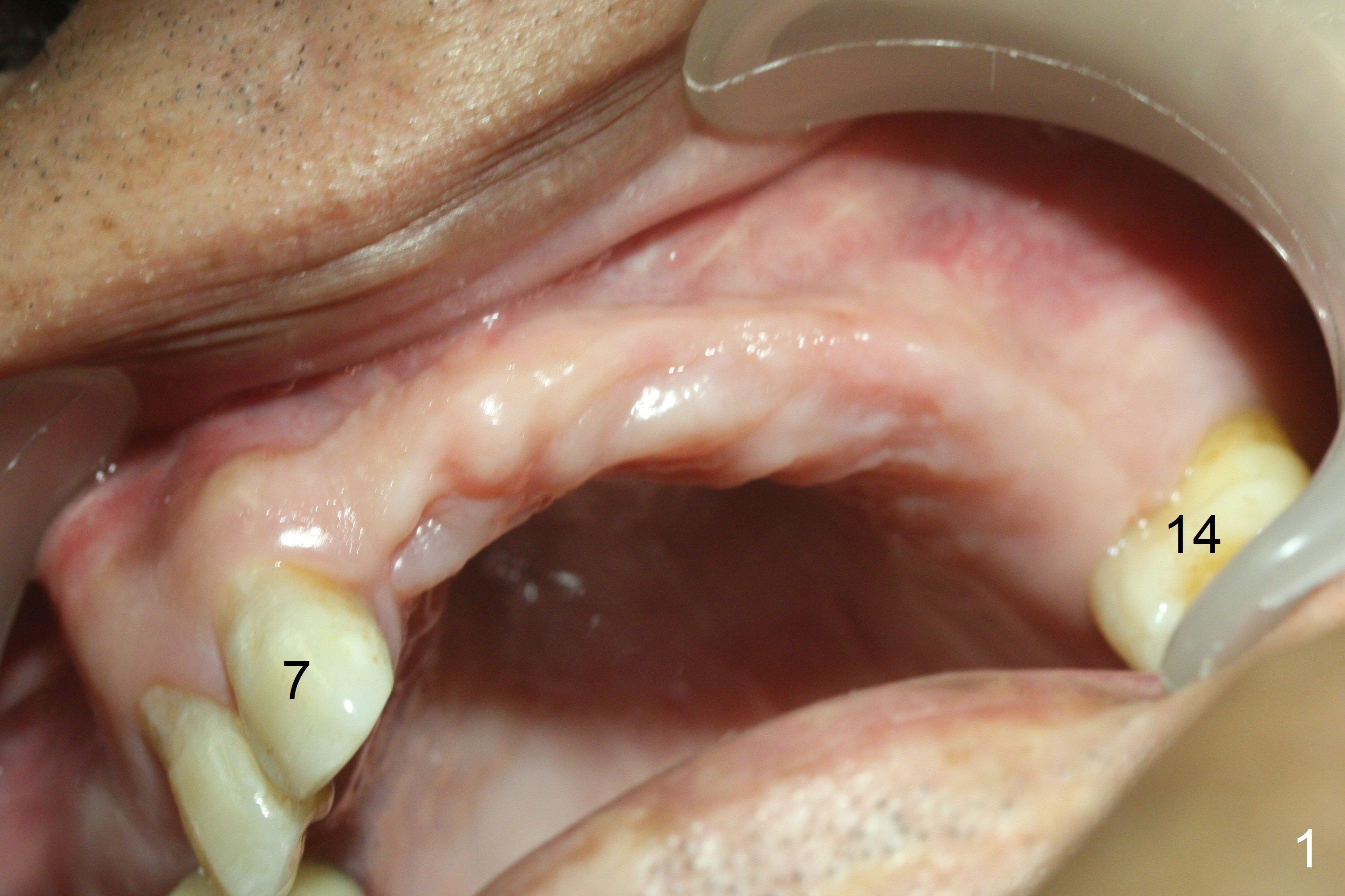
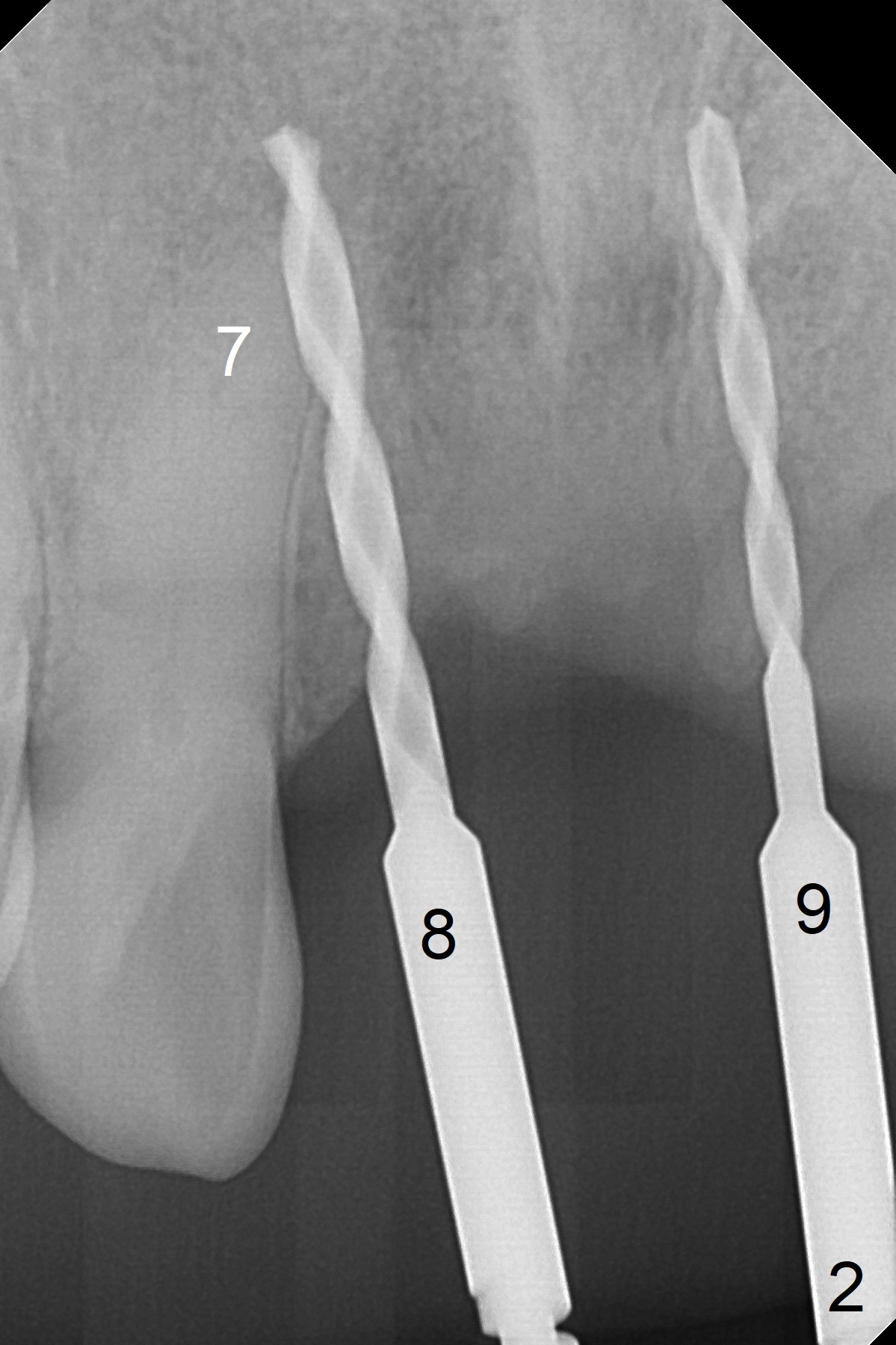
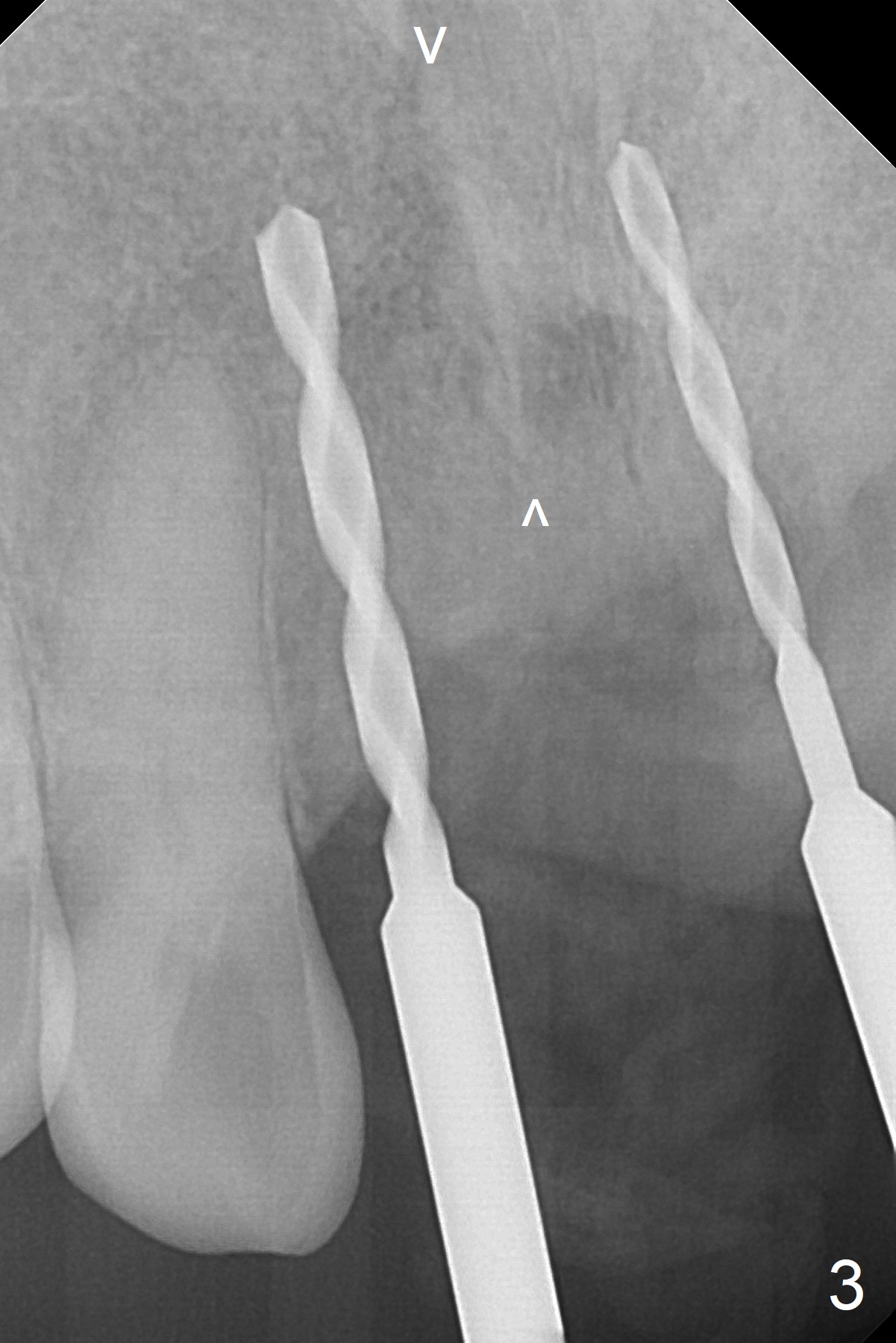
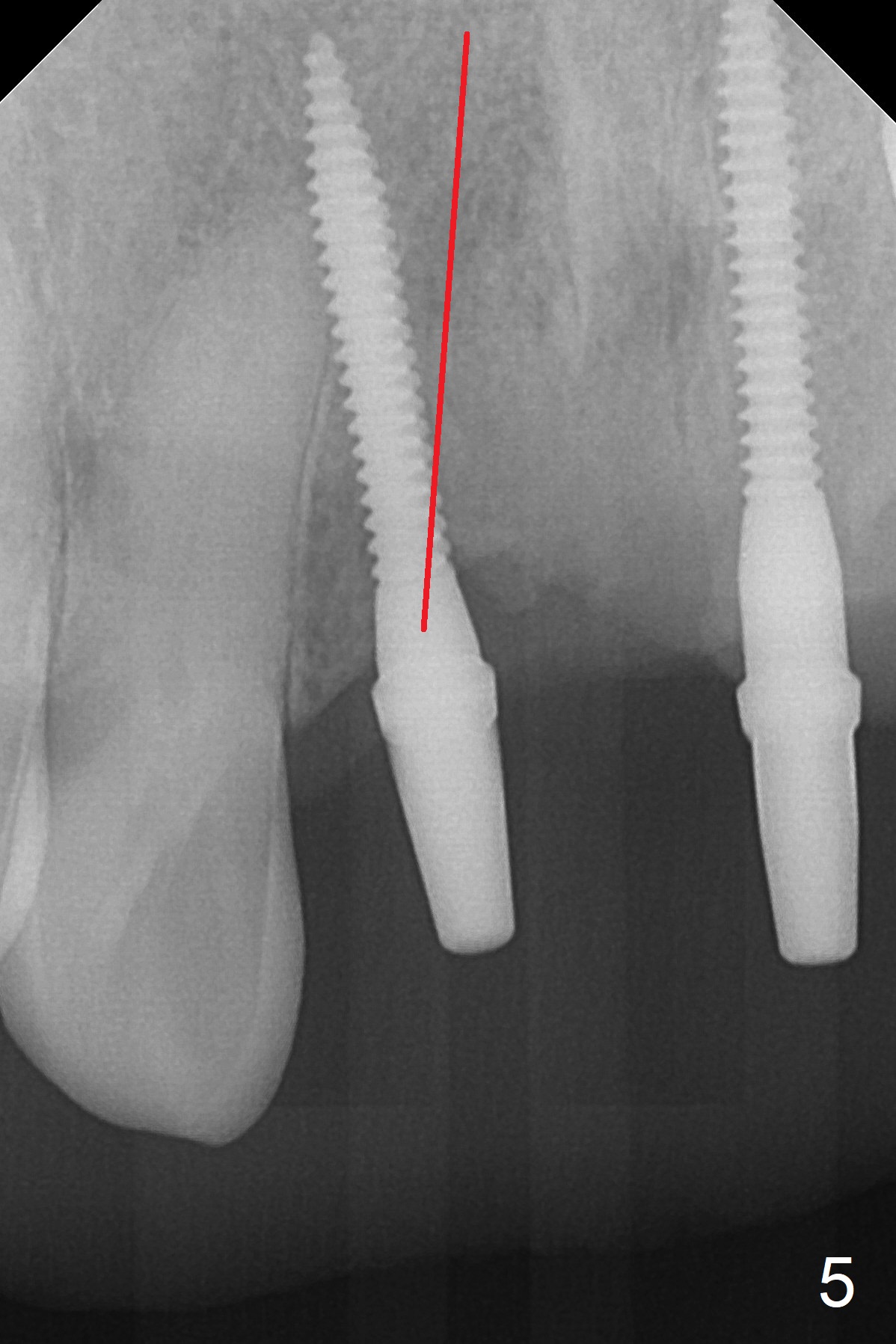
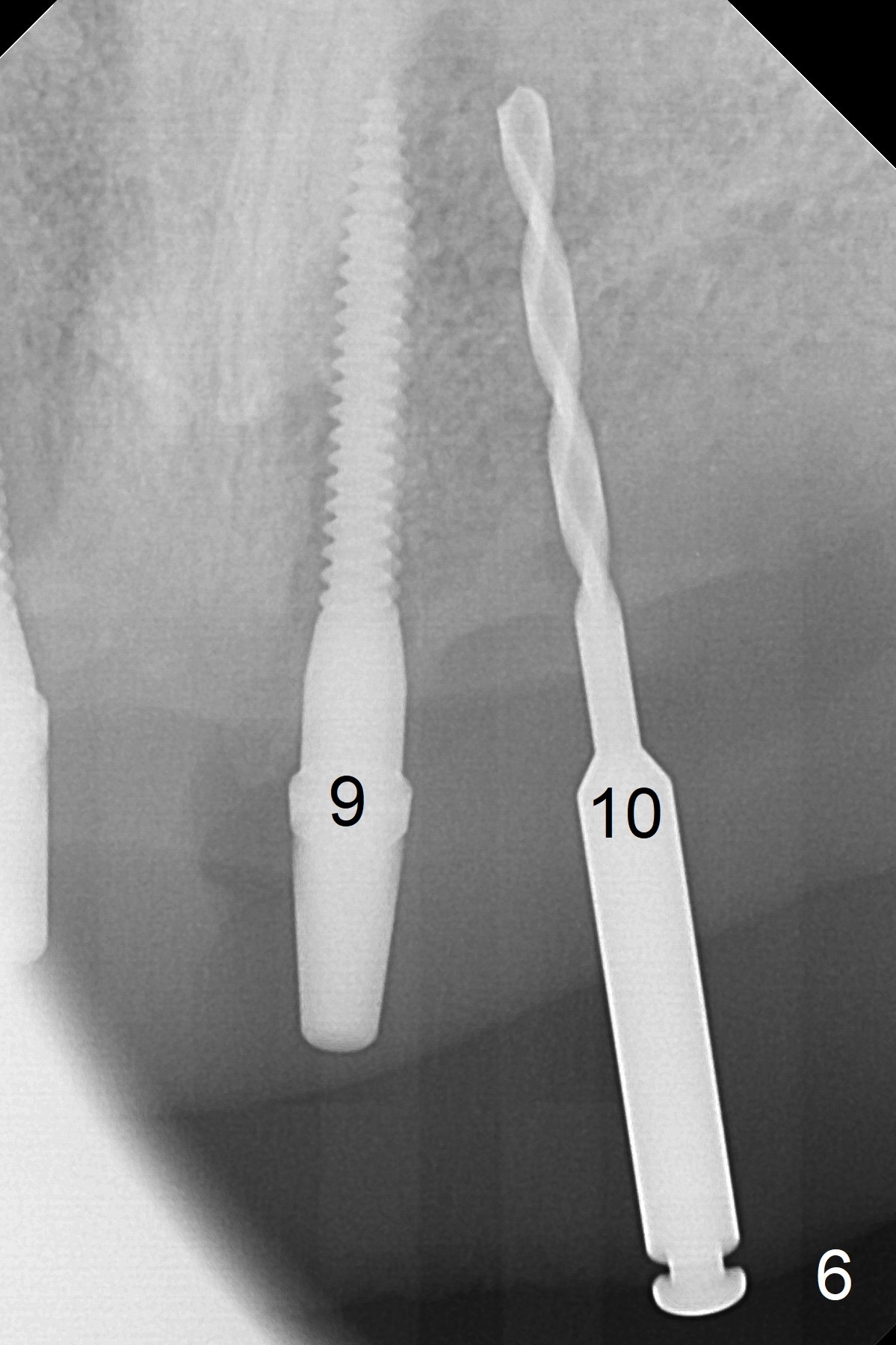
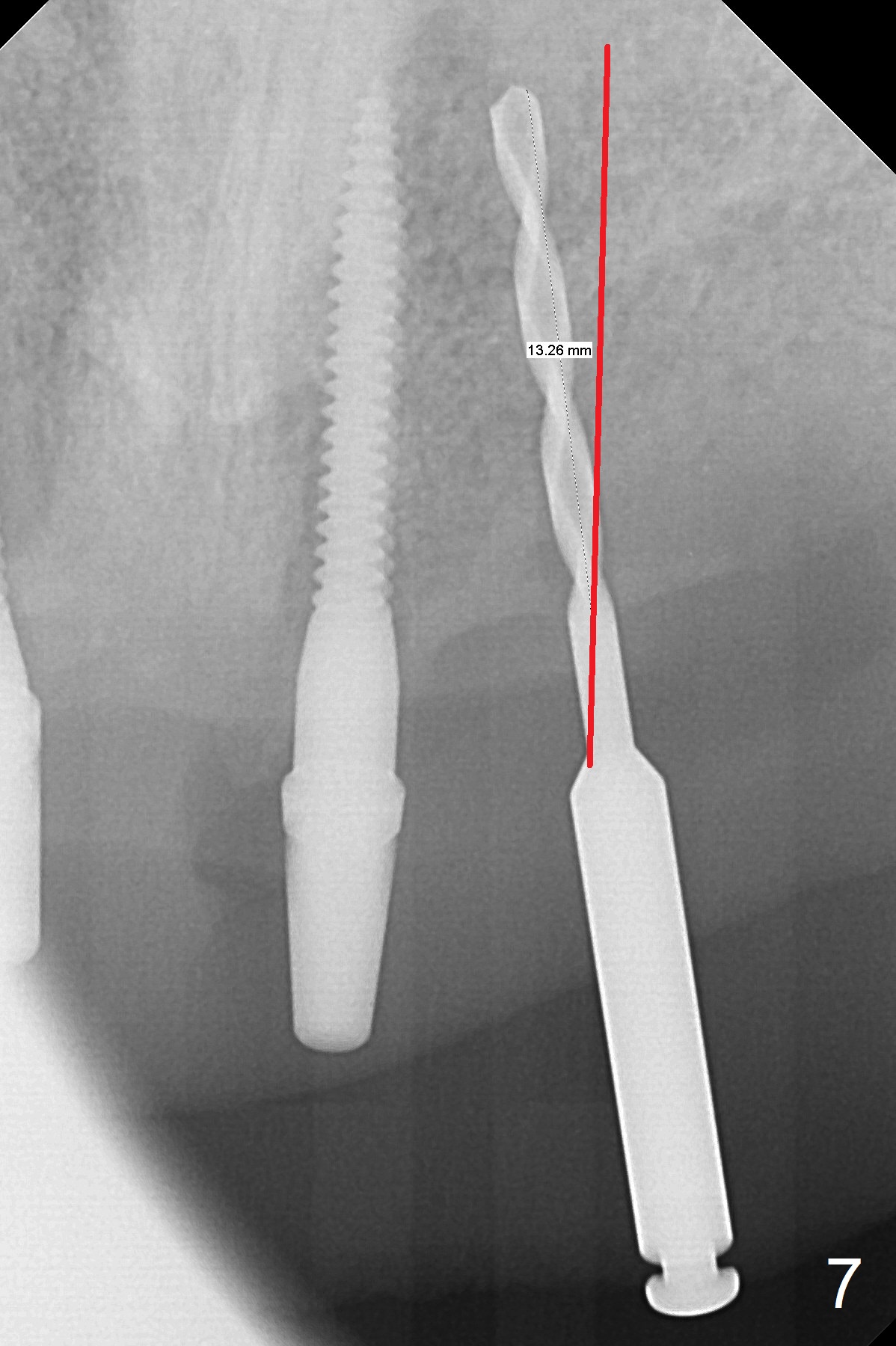
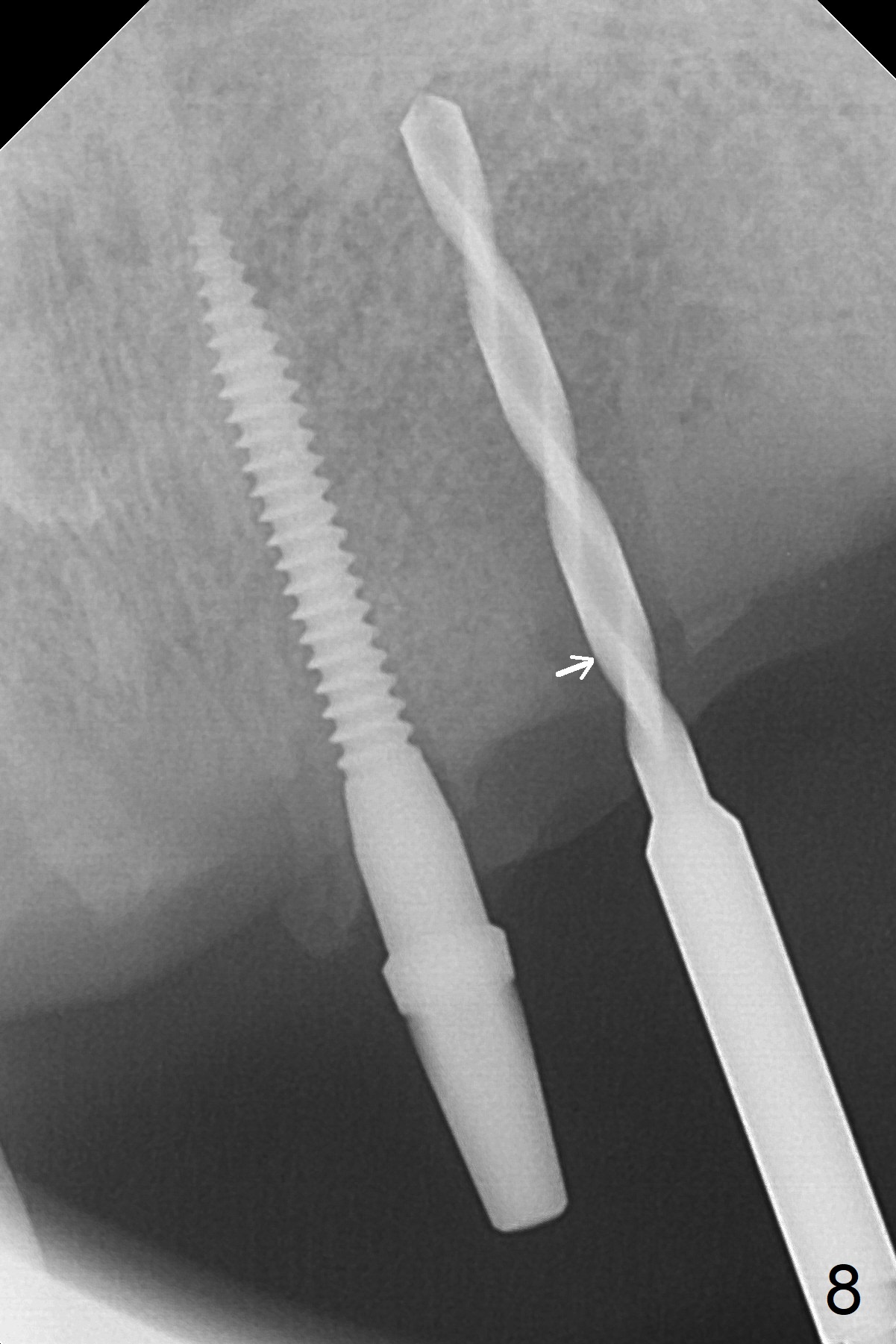
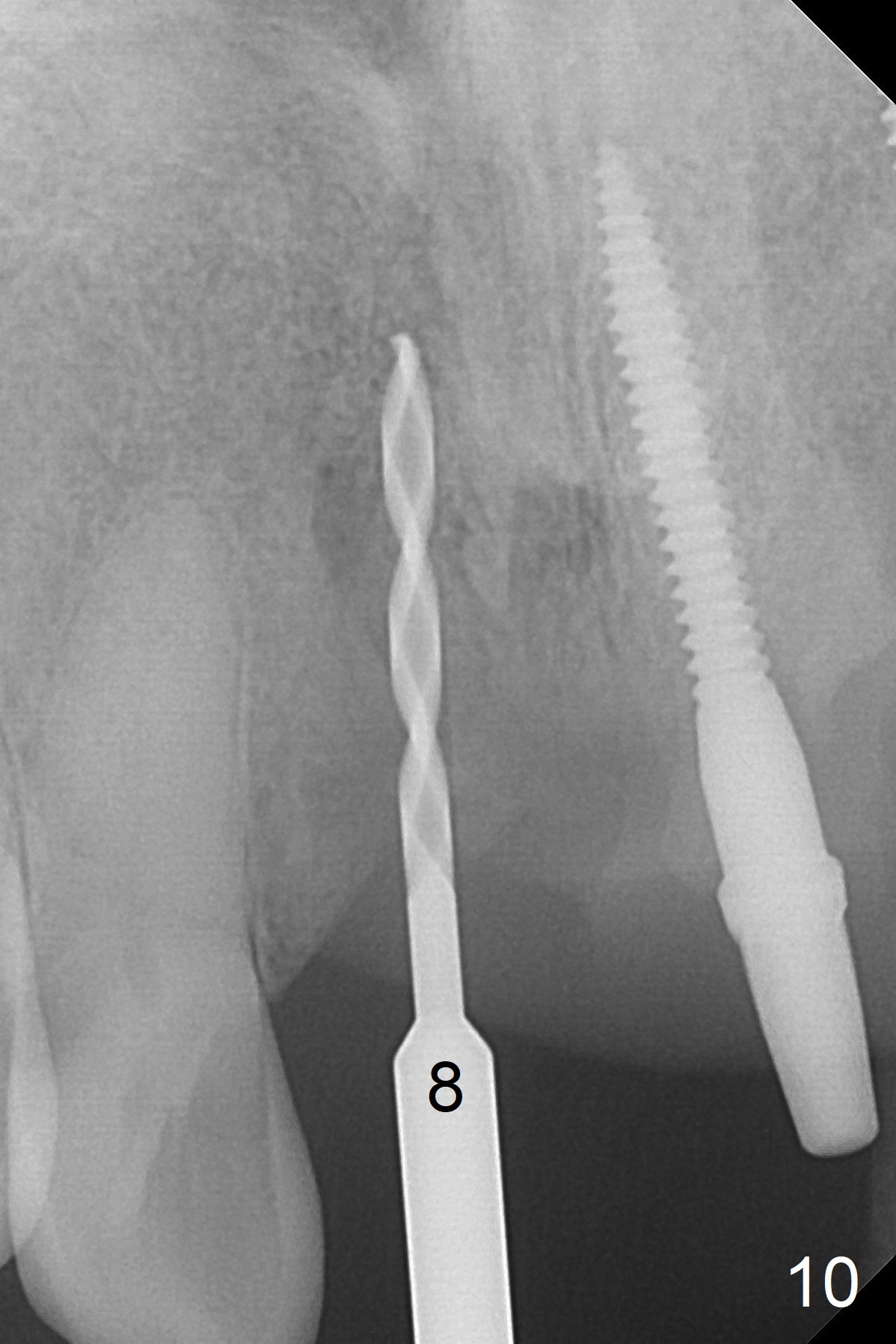
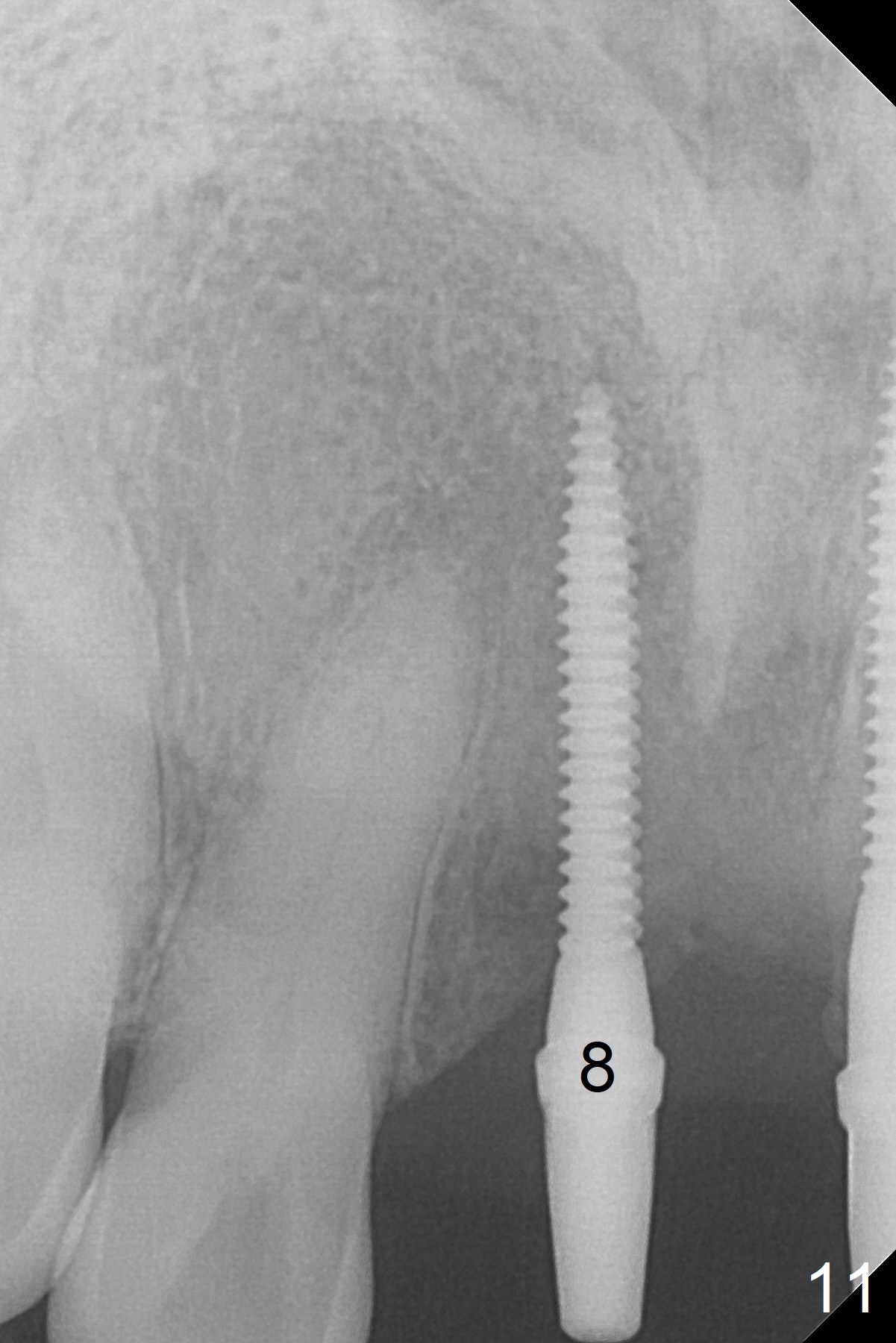
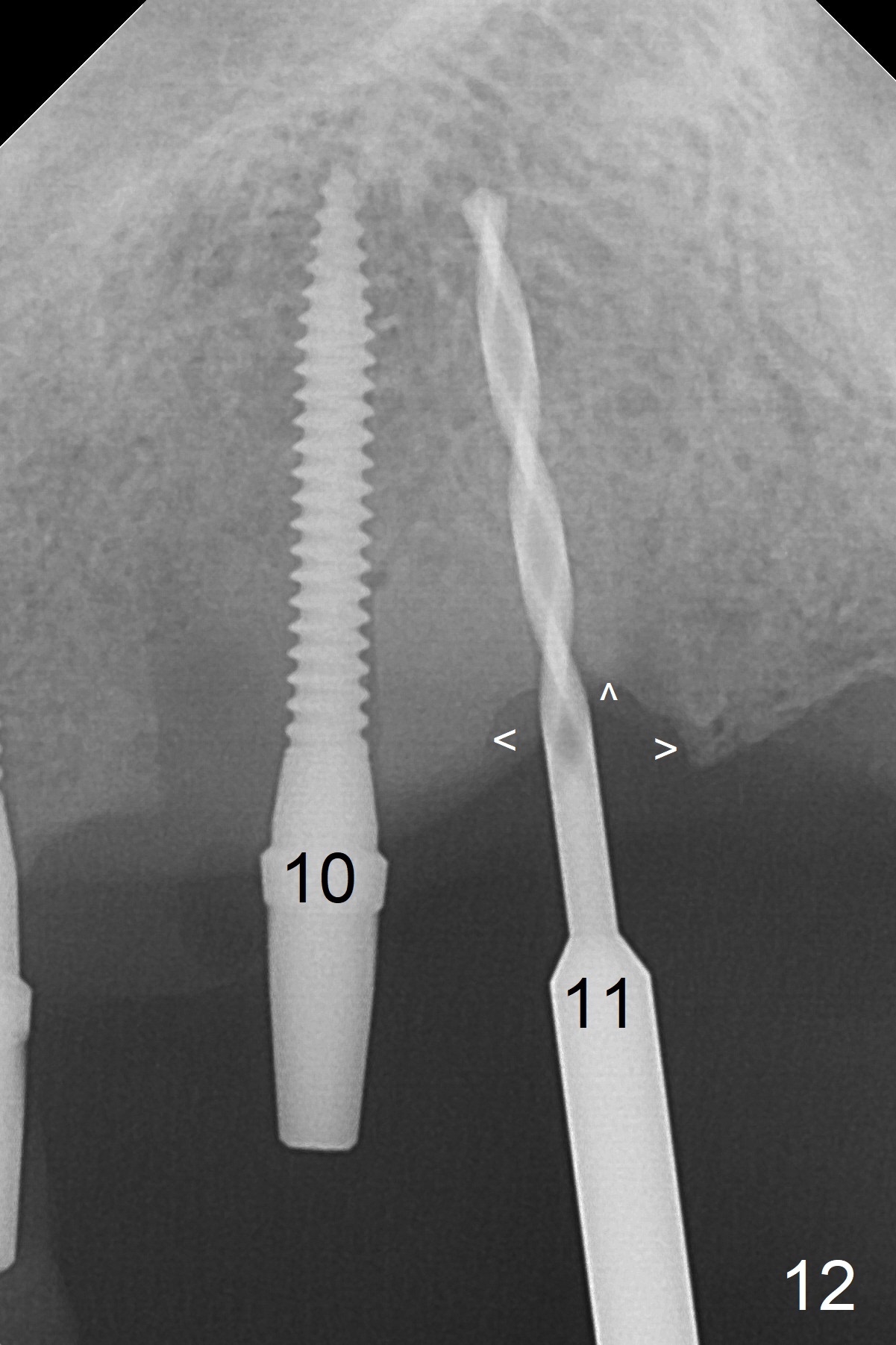
For implant placement of the atrophic ridge (Fig.1), osteotomy starts at #8 and 9 (Fig.2). Change in trajectory at #8 seems acceptable (Fig.3 (arrowheads: upper midline suture)). But it relapses when a 2x14(2) mm implant is placed (Fig.4 (2x14(4) mm at #9)). It appears that a drastic change in trajectory is necessary (Fig.5). The trajectory at #10 with 1.2 mm initial drill is also unsatisfactory (Fig.6) and needs a drastic change in trajectory (Fig.7). In fact the position of the osteotomy needs to be changed (distalized) in order to change the trajectory (Fig.8 arrow). Distalization is more obvious when a 2x14(2) mm implant is placed (Fig.9 arrow). With the same method (change in osteotomy position), the osteotomy with 1.2 mm drill (Fig.10) and the final position of the 2x14(2) mm implant (Fig.11) at #8 are reasonably normal. It is apparent that it is never too late to change trajectory of the initial osteotomy and final position of 2 mm implant.
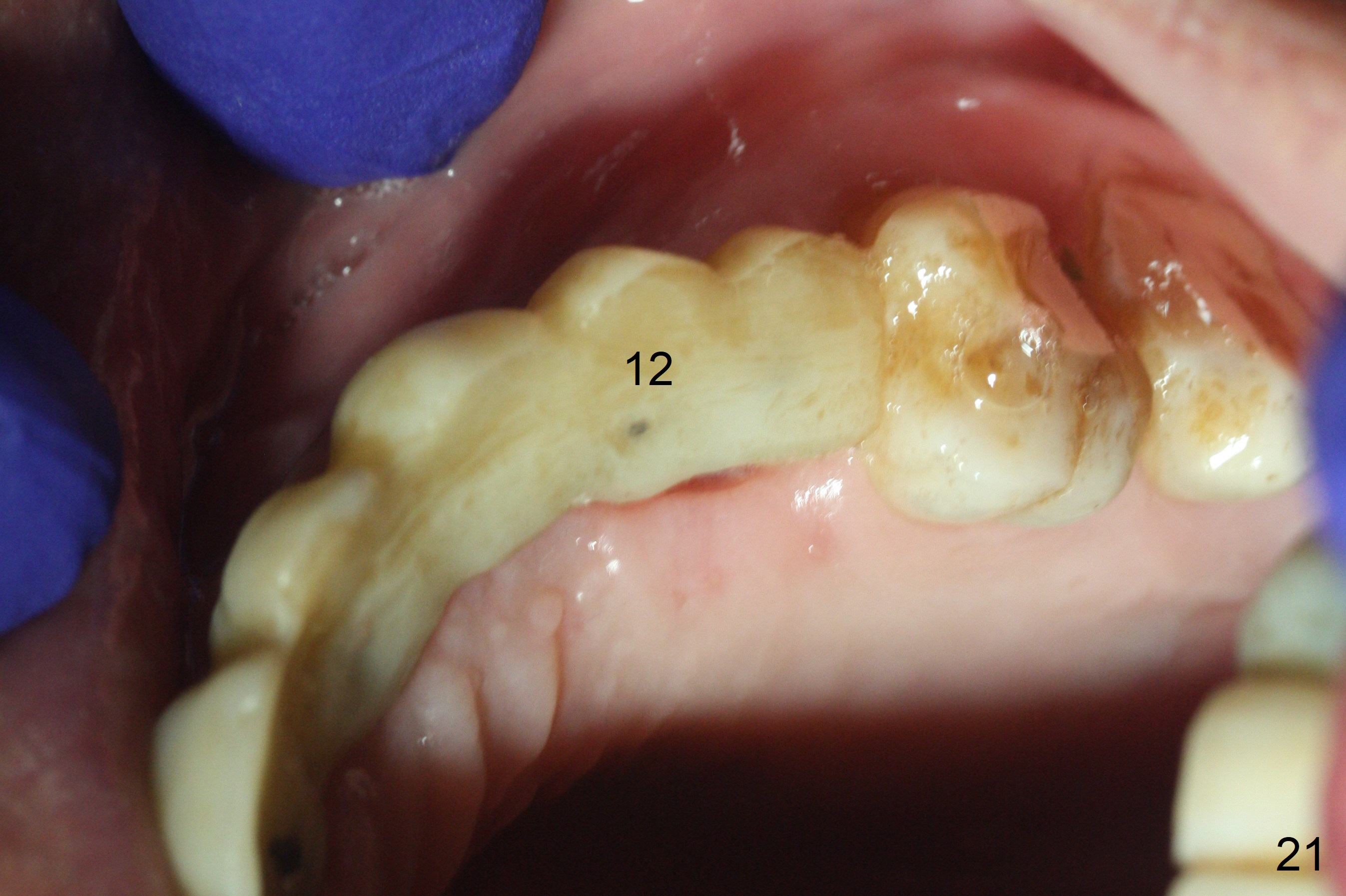
At the sites of #11 and 12, the knife-edged ridge is trimmed prior to initiation of osteotomy (Fig.12,13). With the flattened ridge, it is easy to start osteotomy and control the mesiodistal position. When the position and the trajectory are not correct, they can be changed (Fig.14-16) with 2.5x14(4), 2.5x12(2) and 3x10(2) mm implants placed at #11,12, and 13, respectively.
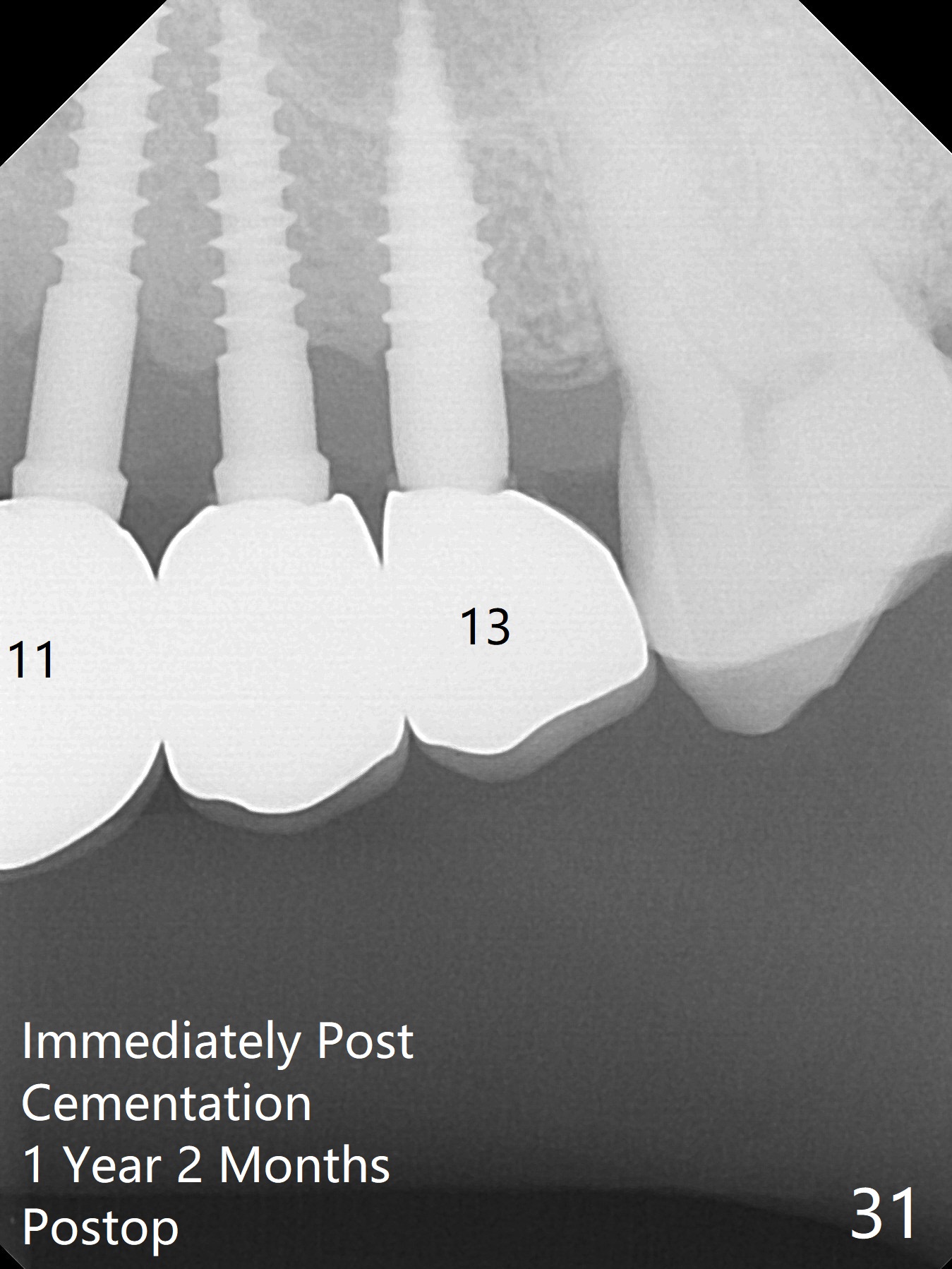
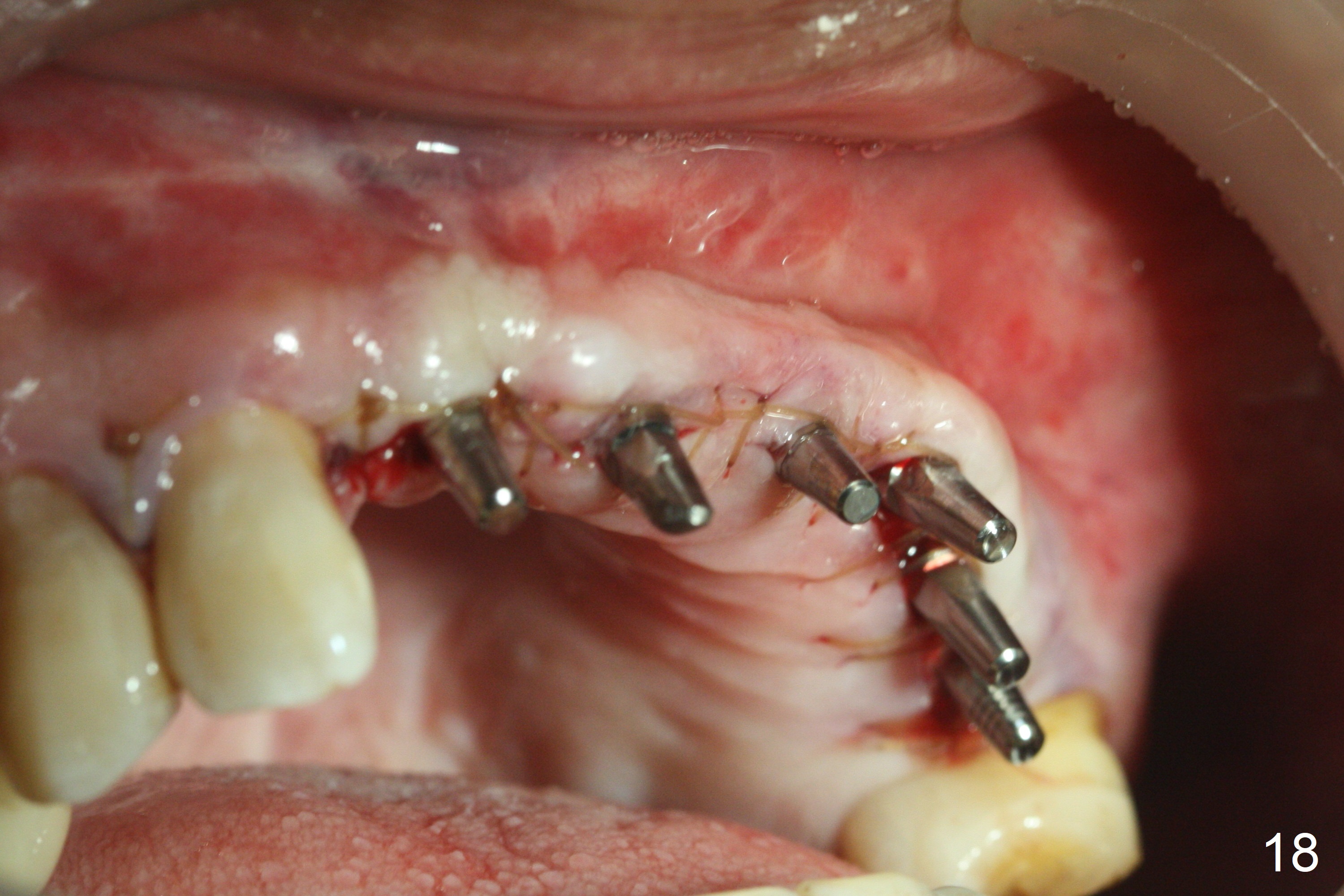
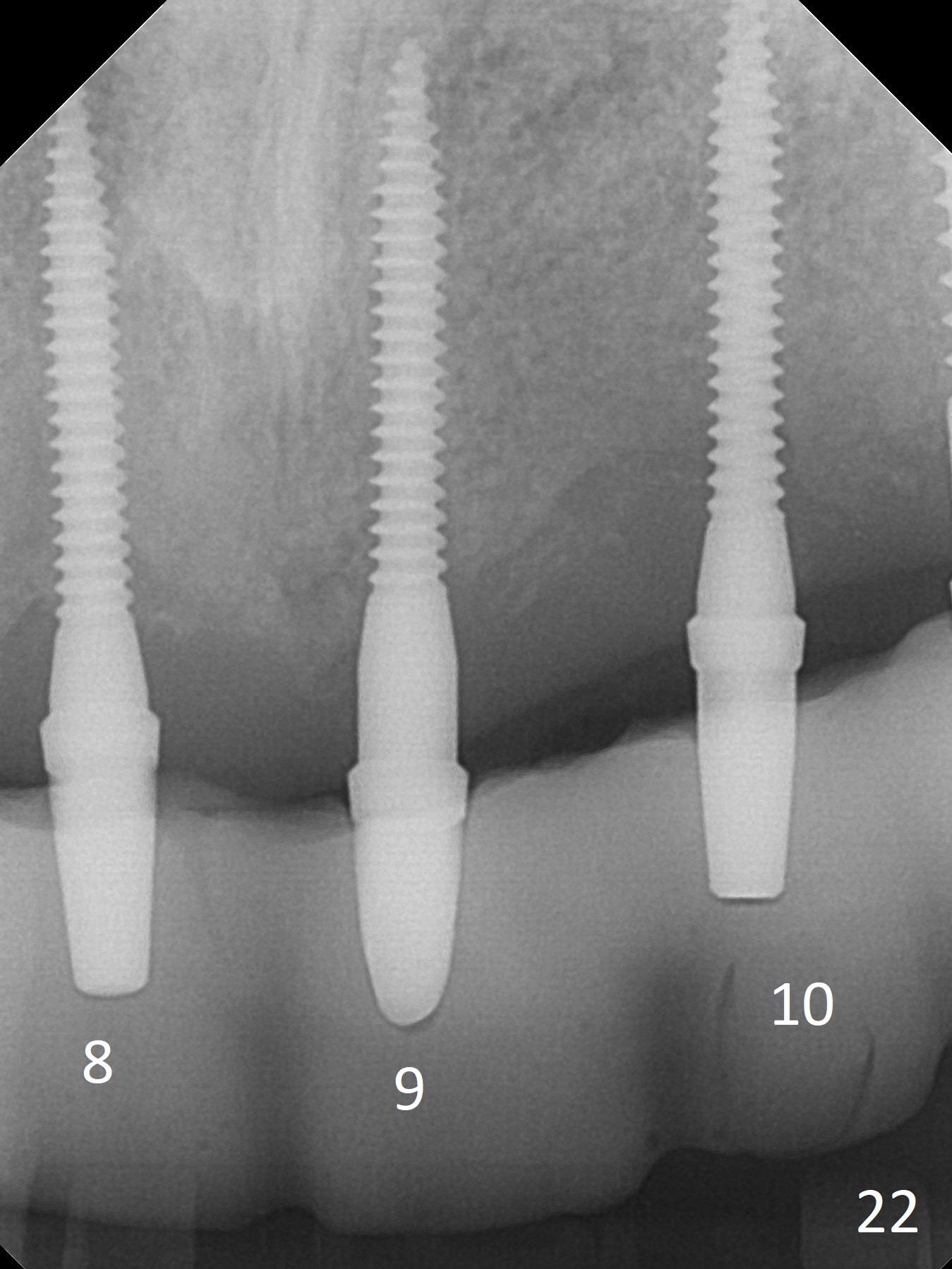
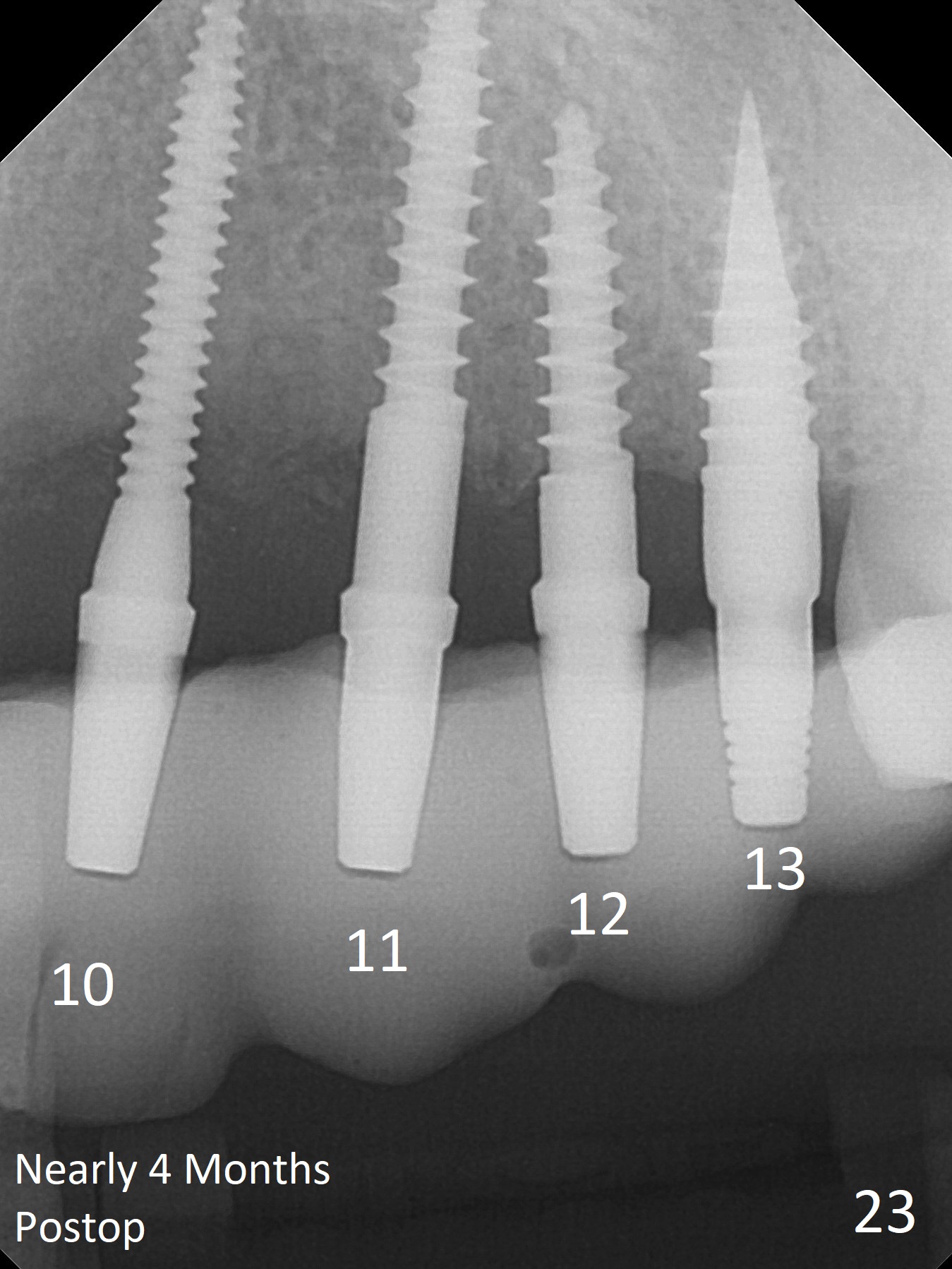
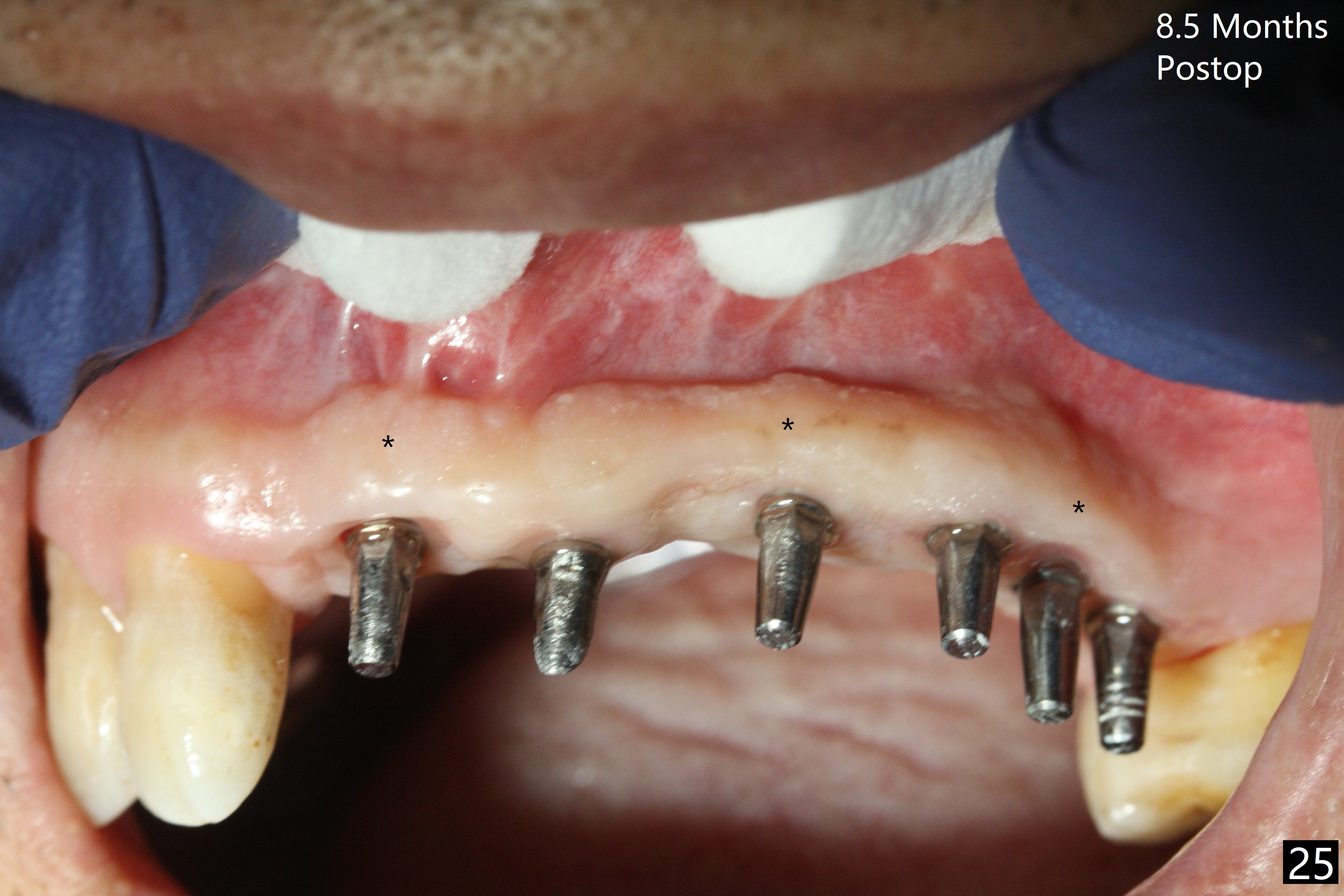
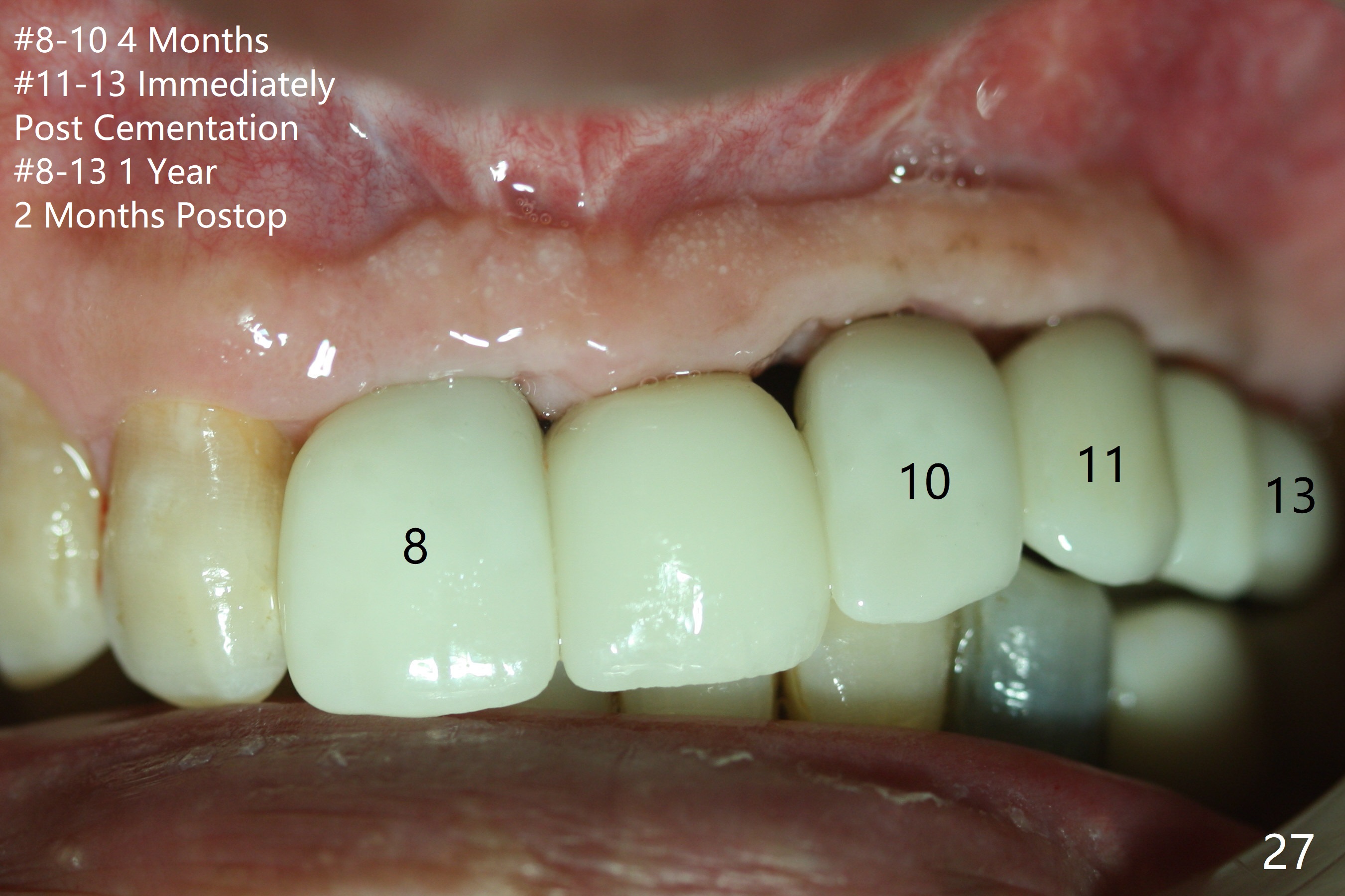
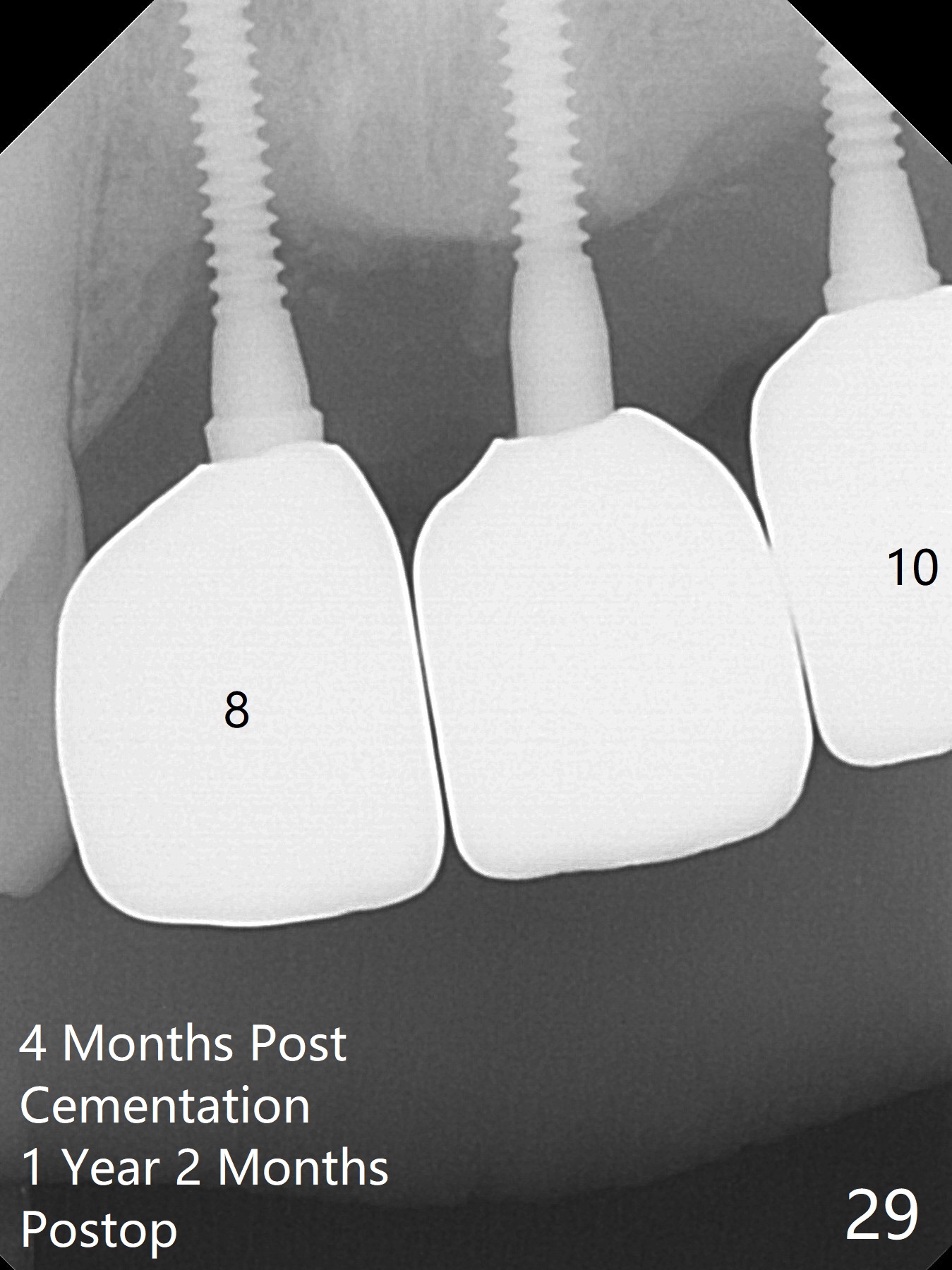
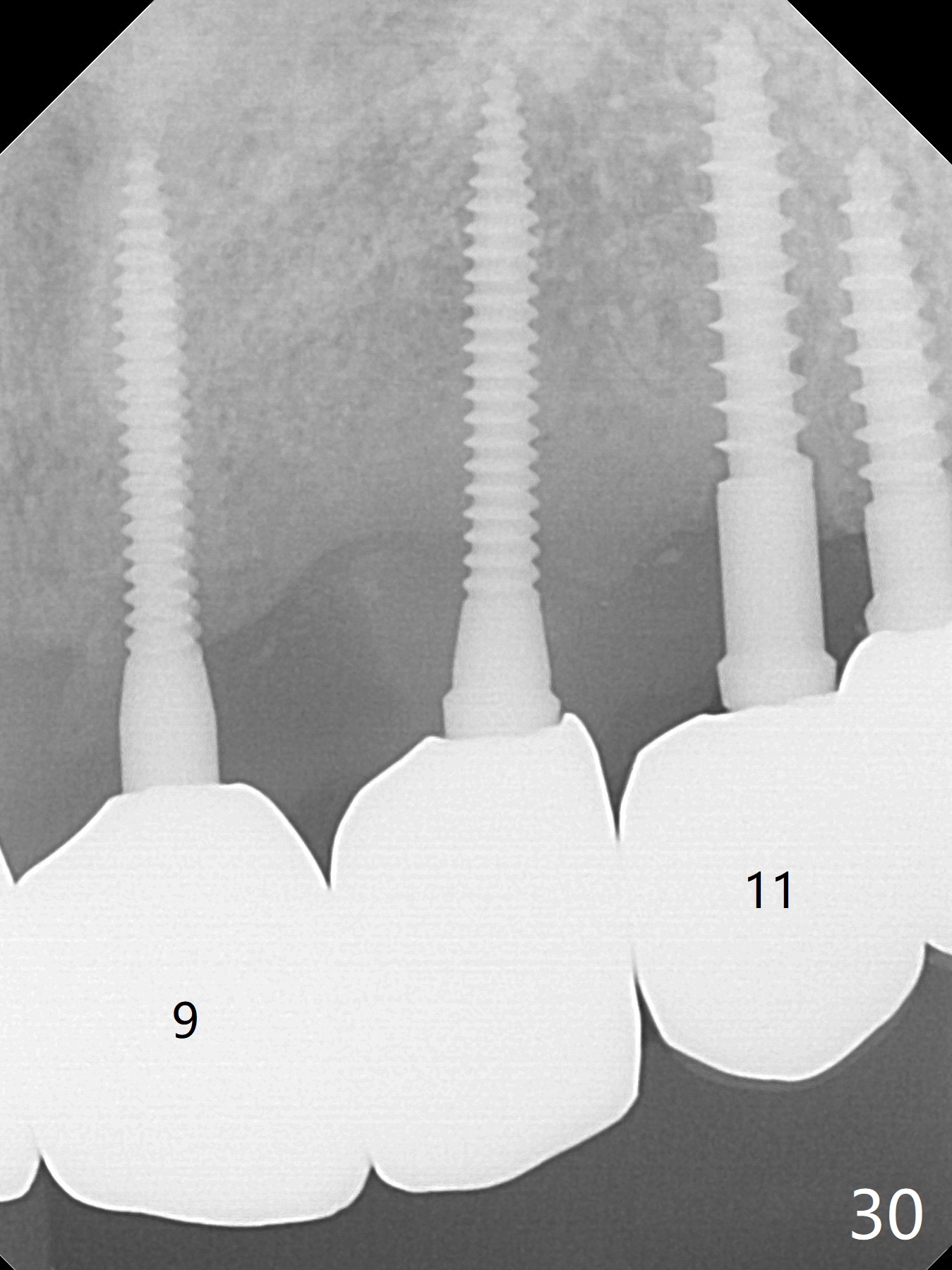
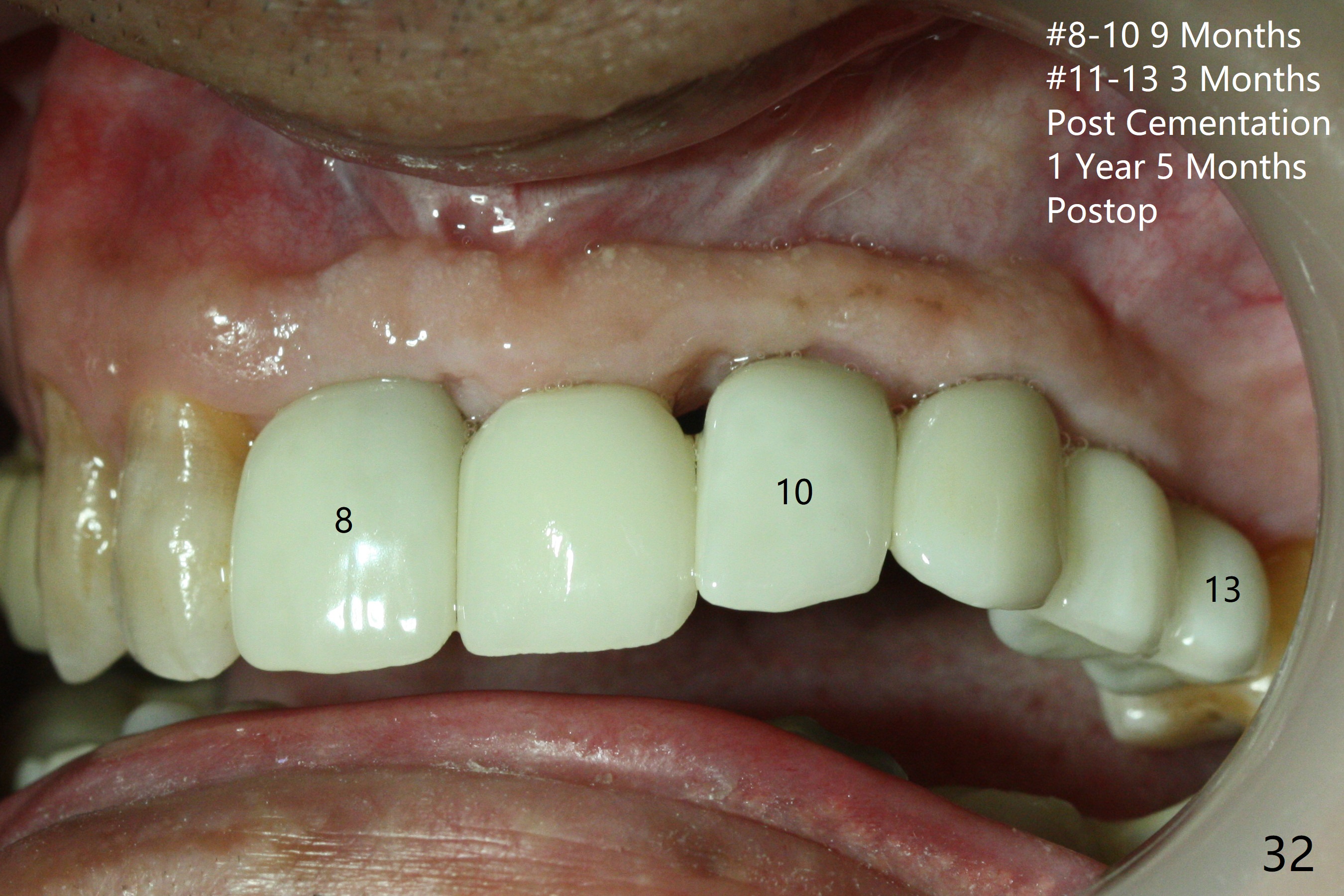
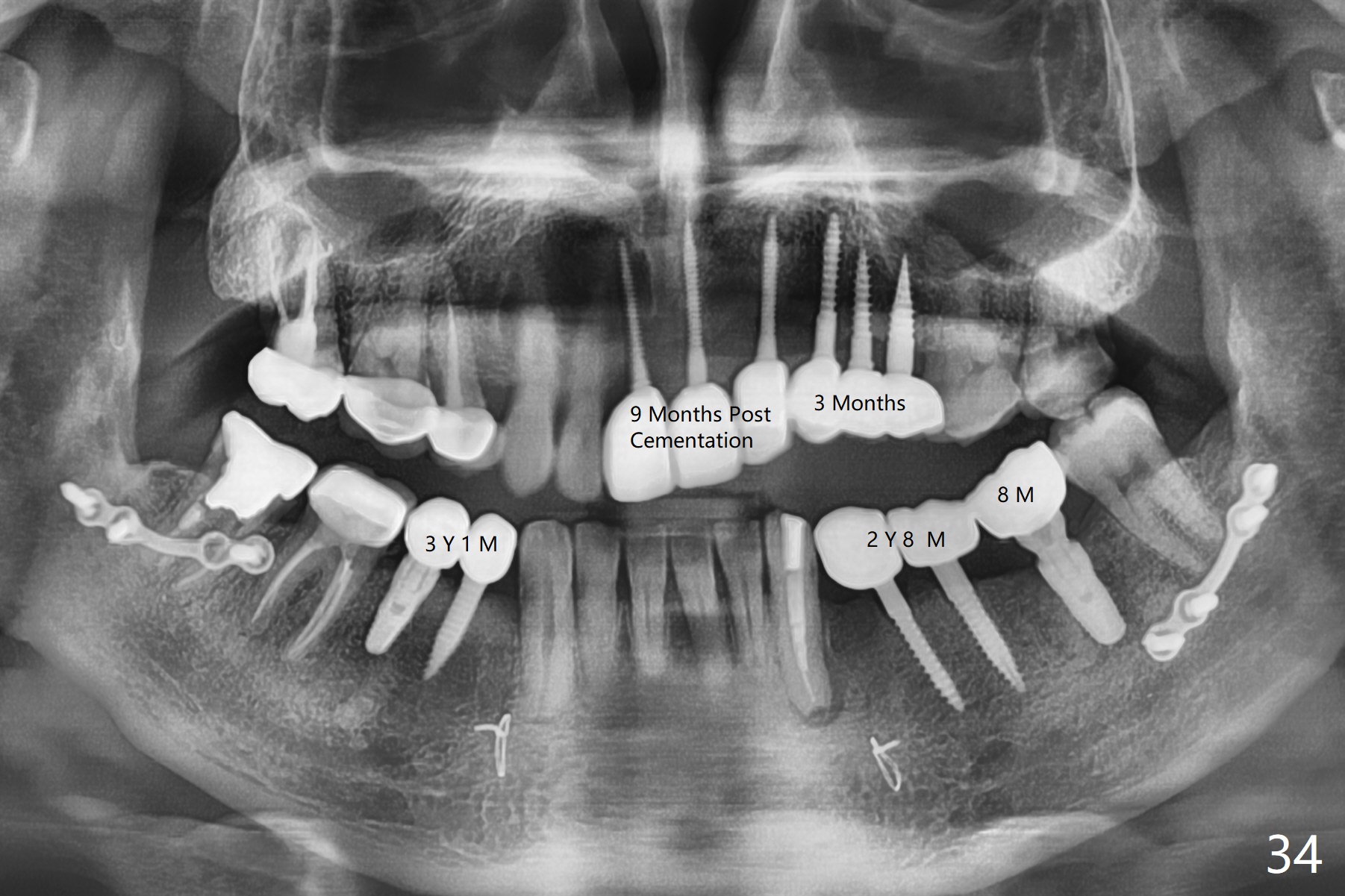
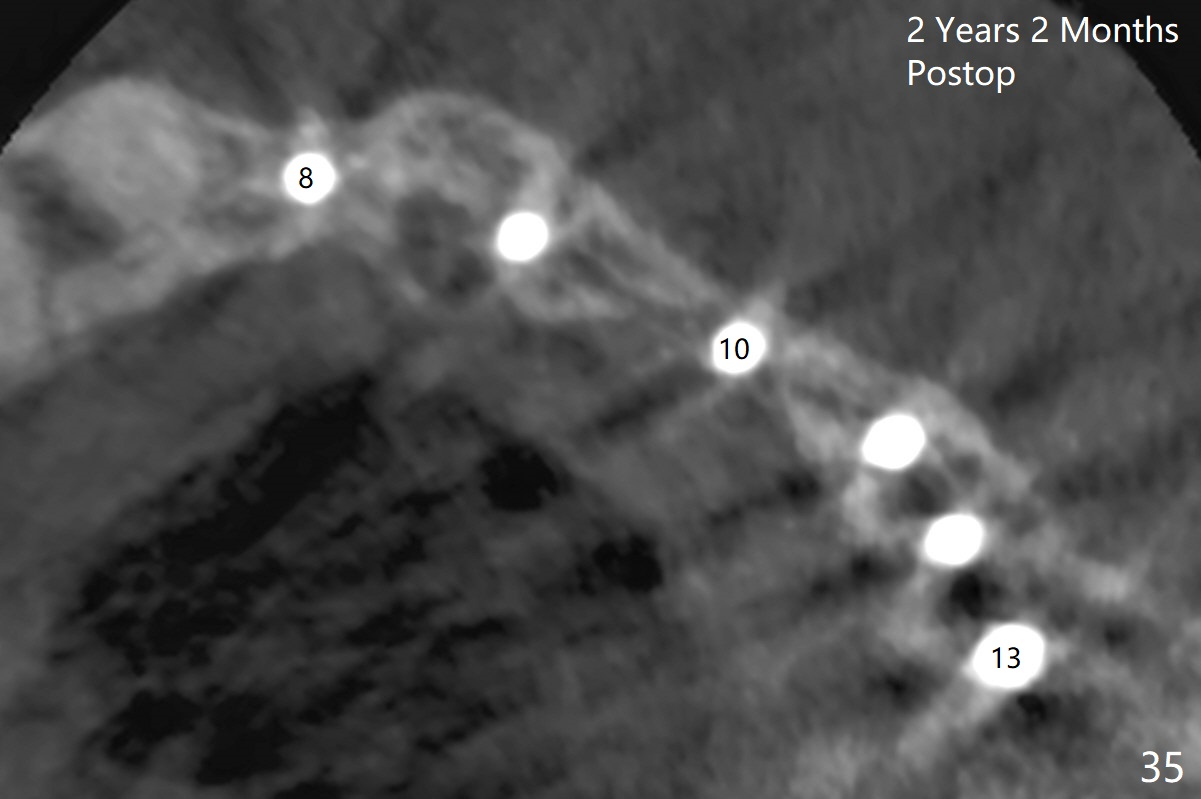
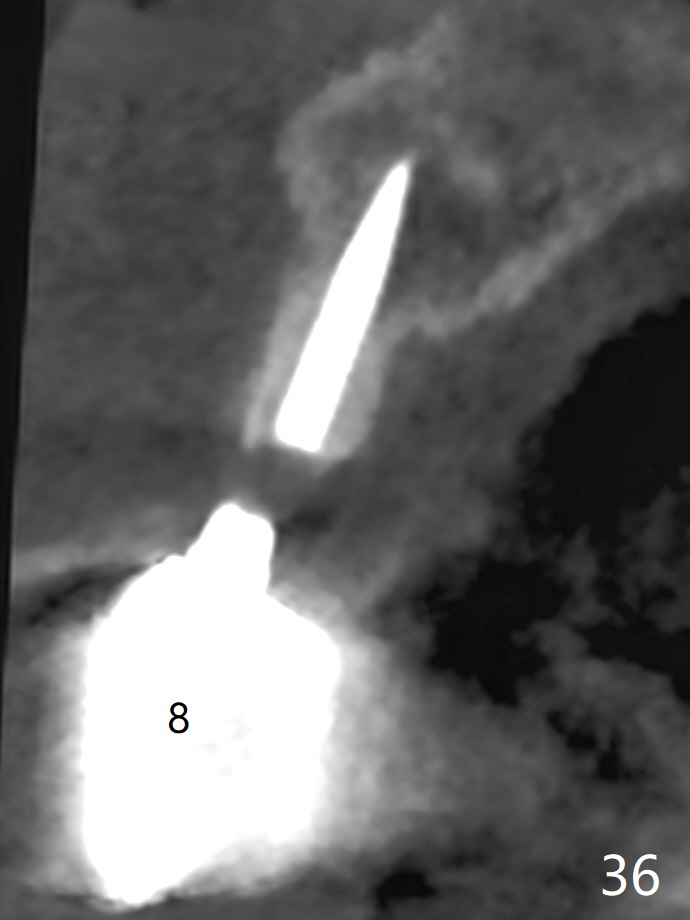
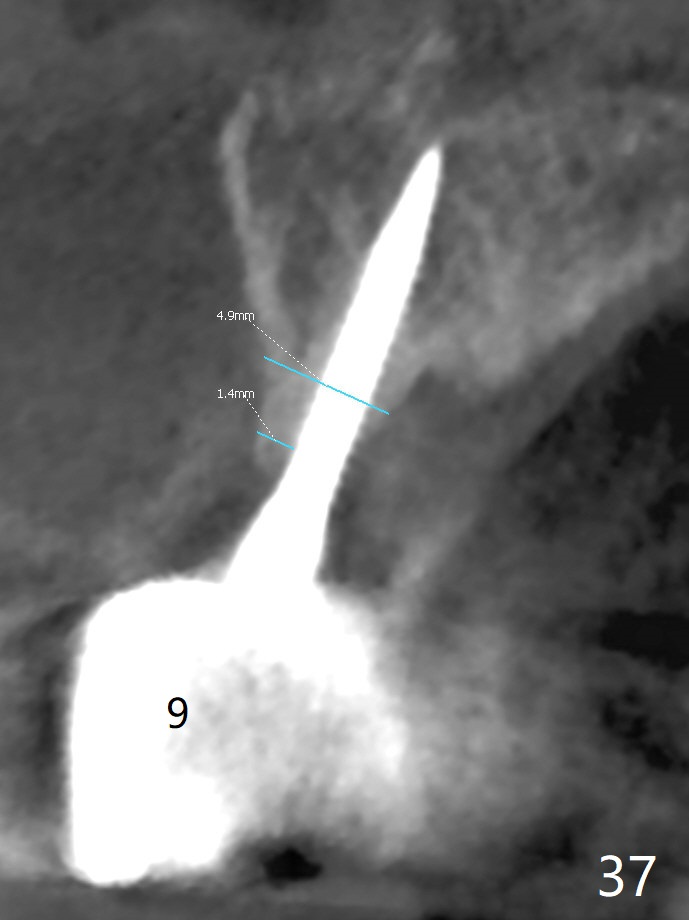
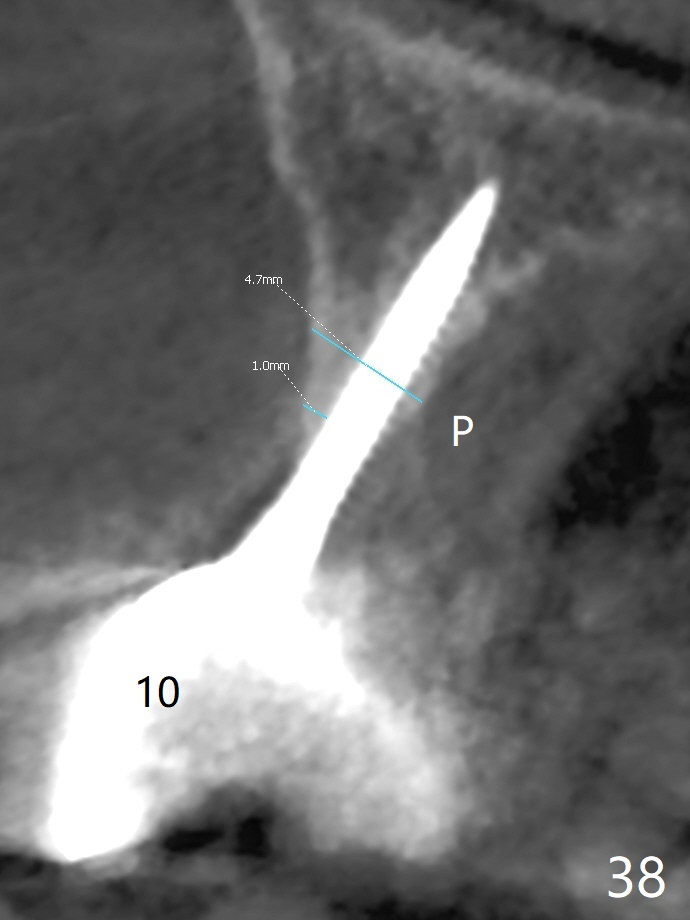
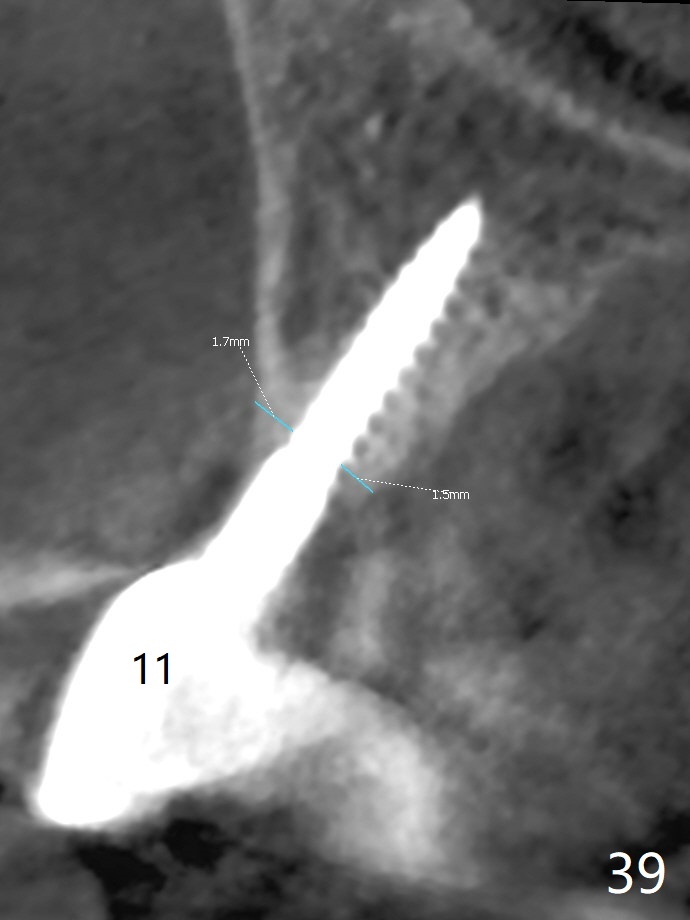
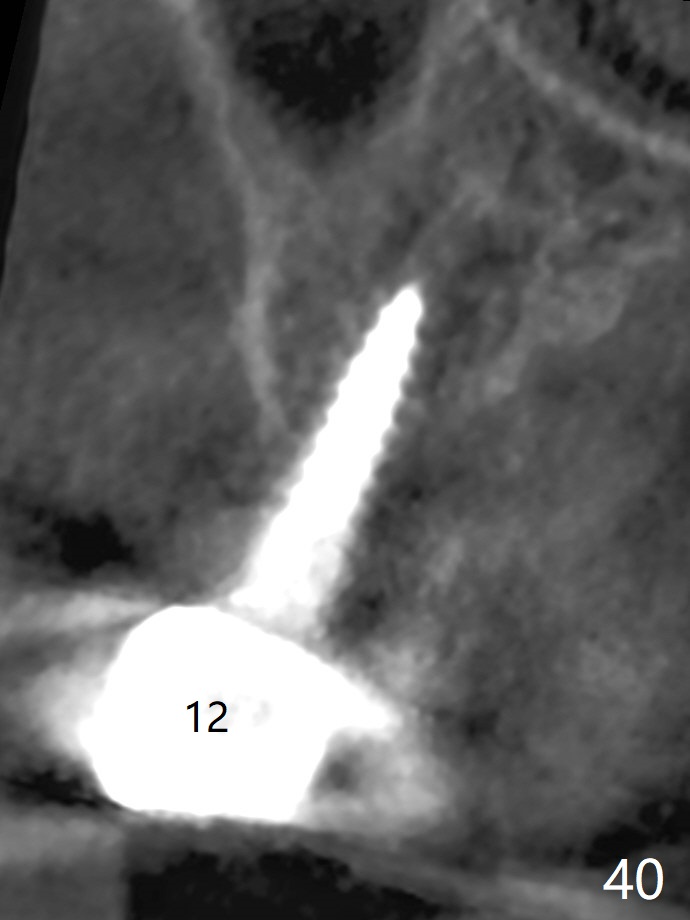
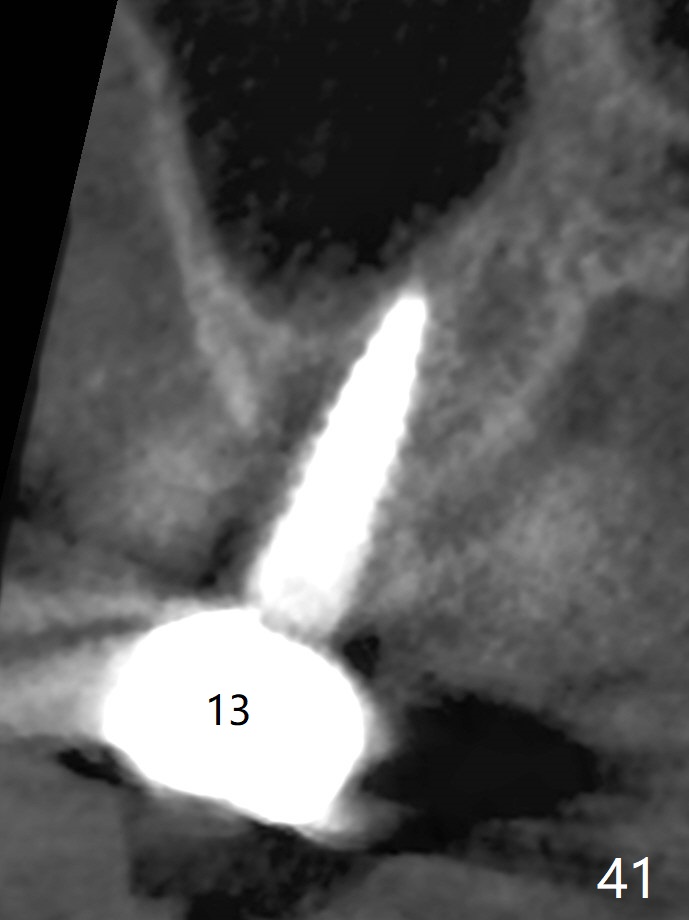
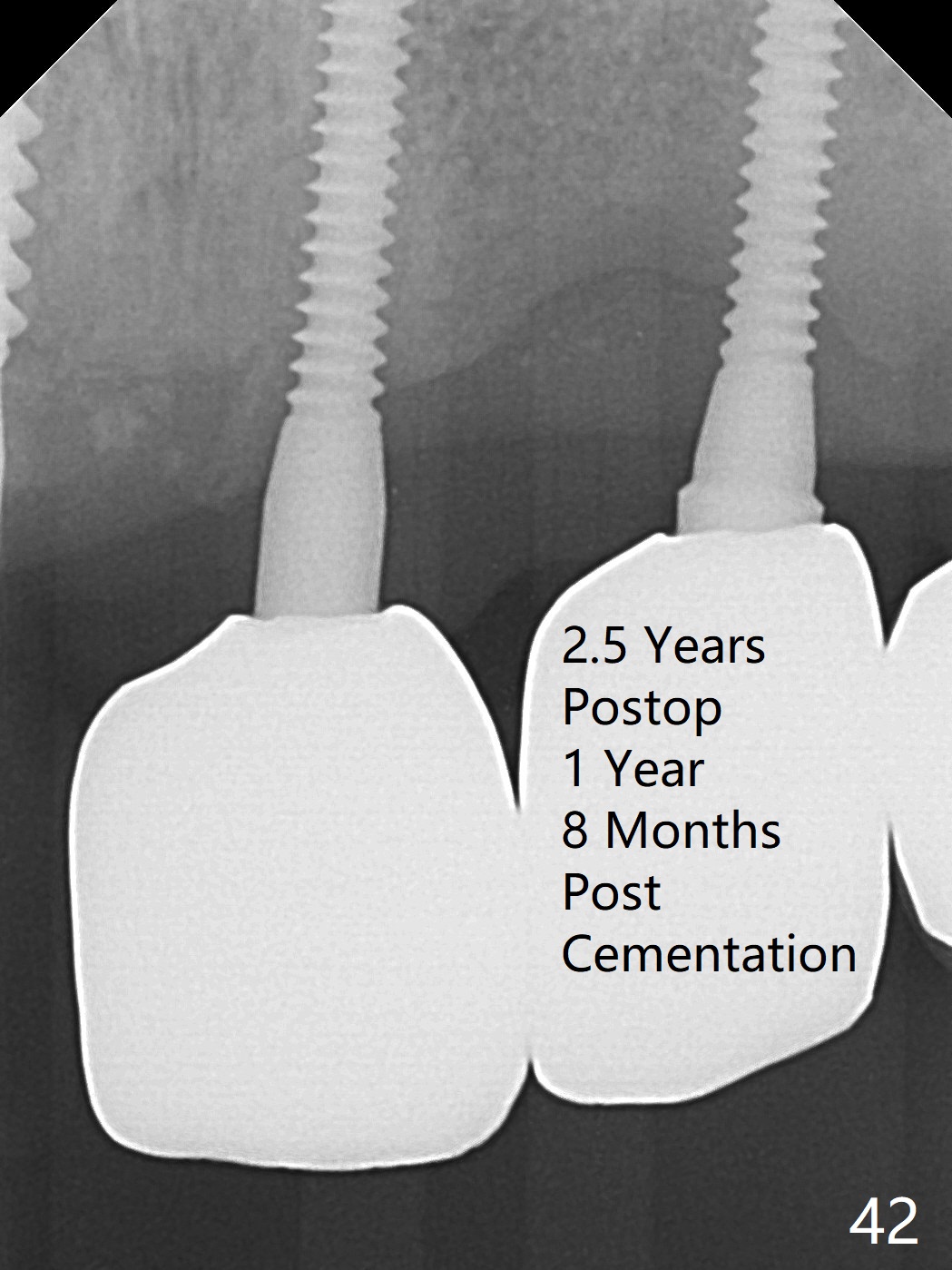
Following allograft placement around the implants (particularly palatally and in void due to change in osteotomy position) and PRF membrane buccopalatally, the ridge looks wider (Fig.17,18) than preop (Fig.1). The soft tissue heals 2 weeks postop (Fig.19-21). There is no bone loss nearly 4 months postop (Fig.22,23). Impression is taken after laser gingivectomy 7.5 months postop (Fig.24). Impression is retaken with gingivectomy because the patient does not like pink porcelain (Fig.25,26). The gingiva remains healthy with use of water pik at #8-10 (4 months post cementation) and at #11-13 (immediately post cementation (1 year 2 months postop), Fig.27,28), while bone loss is minimal (Fig.29-31). The patient is pleased with convenience of the fixed restoration. Three months later, he returns for follow-up; the soft (Fig.32,33) and hard (Fig.4) tissues remain healthy. The implant at #8 fractures 1 year 4 months post cementation (2 years 2 months postop, Fig.35-41). All of the implants except #10 are placed in the middle of the alveolus.
Return to
Lower Arch Reconstruction
LR
LL
19
IBS
1-Piece
Chinese,
Atrophic Ridge
Xin Wei, DDS, PhD, MS 1st edition 07/21/2017, last revision 02/04/2020