
,%20incomplete%20seating.jpg)
,%20click,%20more%20graft,%20complete%20seating.jpg)

|
|
|
||
|
|
|
|
|
|
|
|
||
Tight Fit of Implant/Abutment I
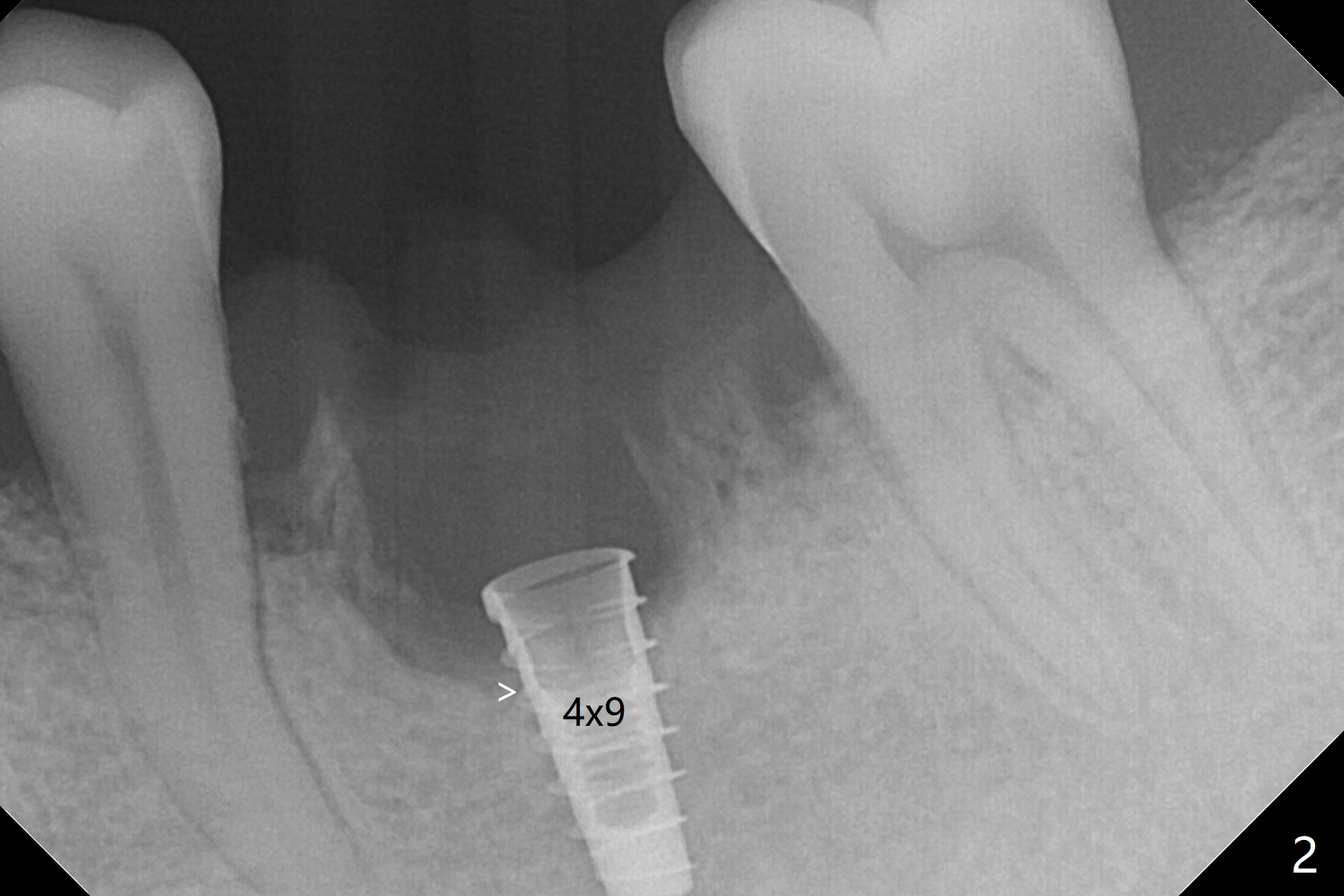
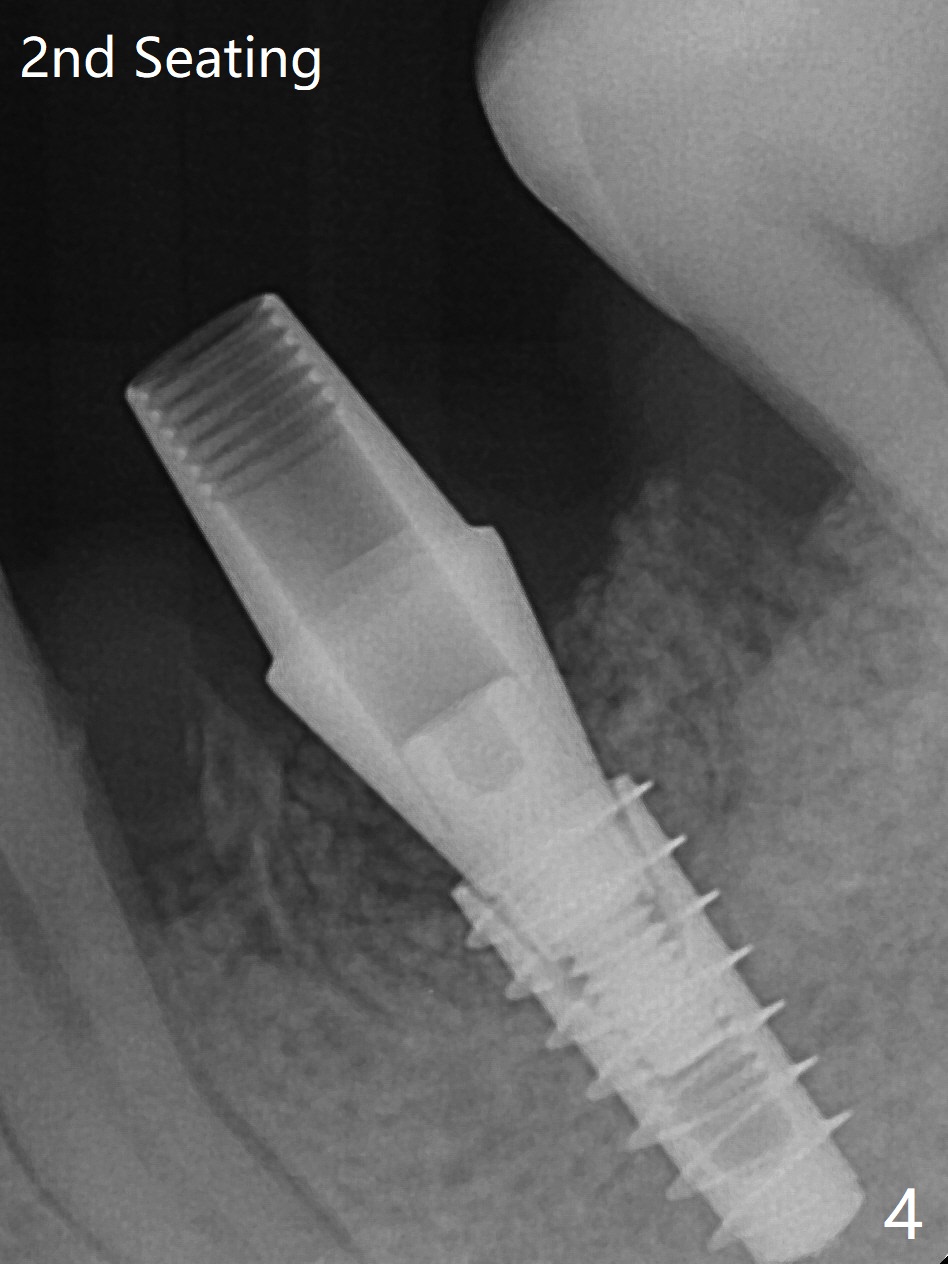
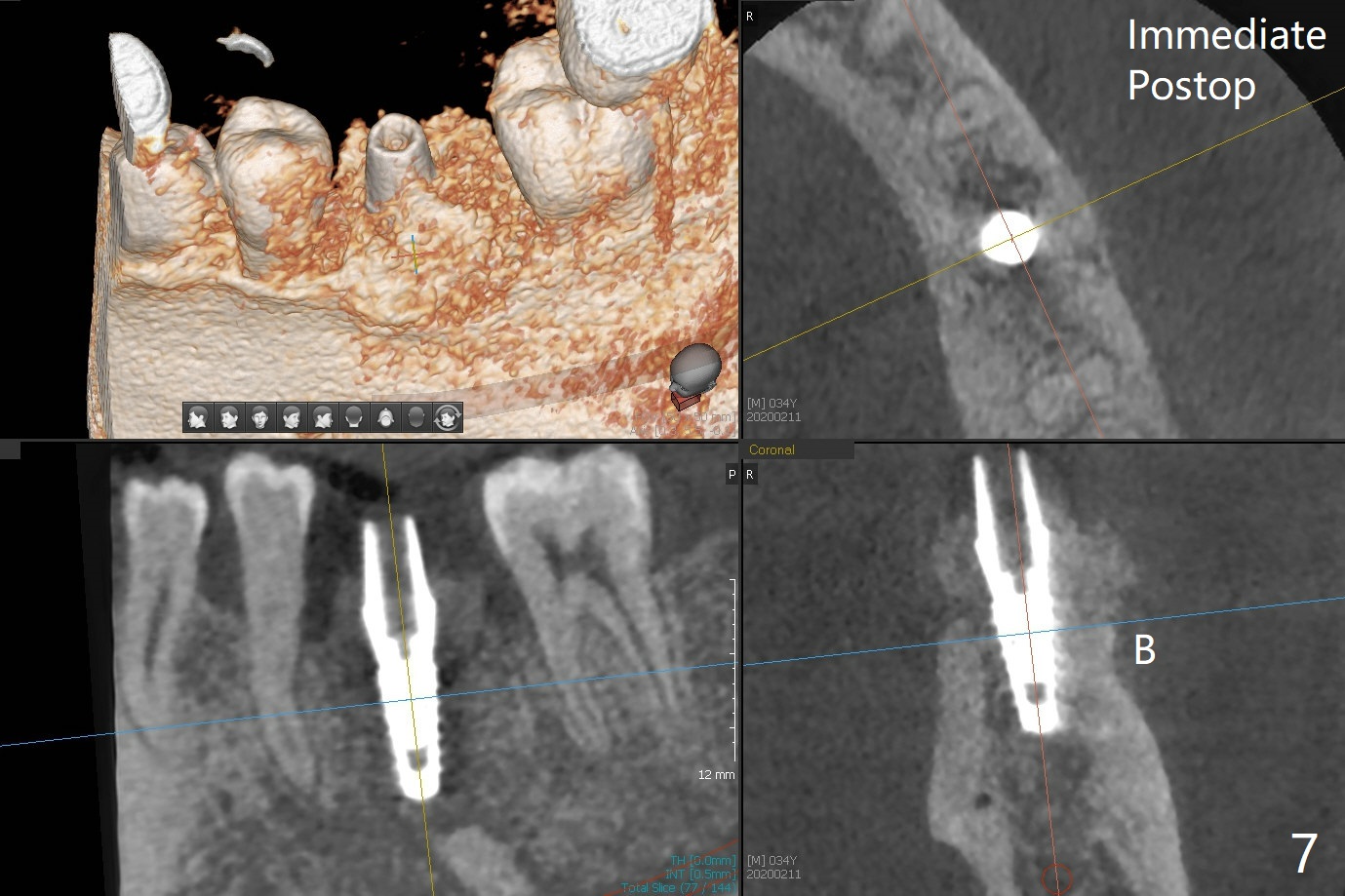
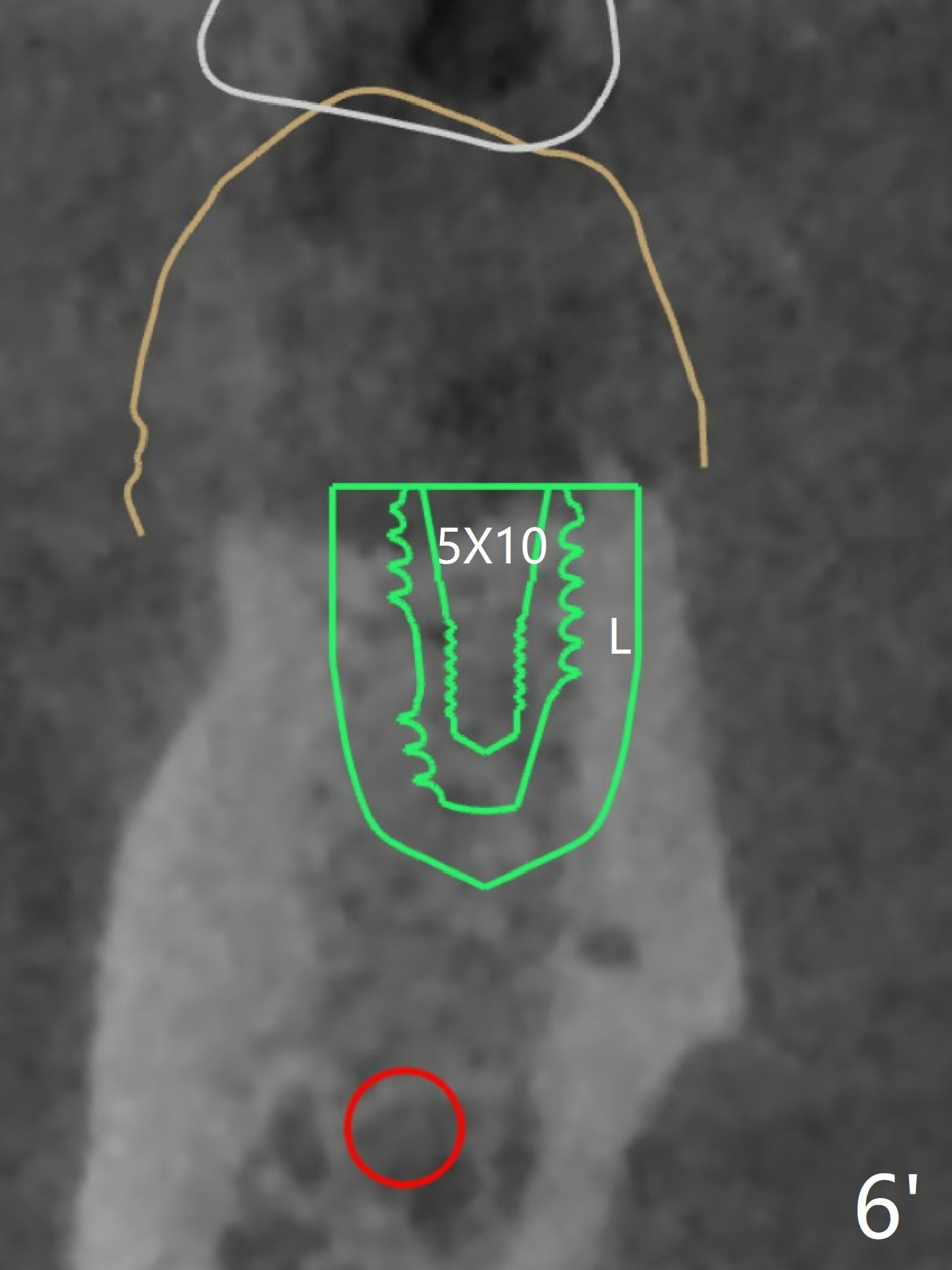
In spite of smoking reduction (1ppwk), the infection at #19, including buccal fistula (Fig.1 <) seems to be so severe that it affects pain threshold. Local anesthetics have to be added, including Bupivacaine IANB. When 4x10 mm drill is being applied, the patient feels pain. The plan is to use 4x11.5 mm drill as a final one. A 4x9 mm dummy implant is placed with 2.8 mm implant exposed (Fig.2 >), but it is subcrestal mesiodistally. Primary stability of a definitive 4.5x9 mm implant is satisfactory (Fig.3), but after initial bone graft, a 5x5.7(4) mm abutment is unable to be seated completely (<). Following 4.6 and 5.6 mm bone profile drills, the abutment remains incompletely seated (Fig.4). After fine turning, the abutment is fully seated; final round of bone graft (sticky bone) is placed mesiodistally (Fig.5 *) and buccolingually (Fig.6,7). It appears that there is tight fit between IBS implant and abutment. It is hoped that the excess bone graft with PRF is able to cover the coronal portion of the implant. If not, socket preservation should be done in this situation. In fact the implant is not placed lingual enough as compared to the design (Fig.6'). A 4.5 mm cortical drill should be used in a crown down fashion.
Return to Prevent Molar Periimplantitis (Protocols, Table) No Deviation
Xin Wei, DDS, PhD, MS 1st edition 02/11/2020, last revision 05/30/2020