|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
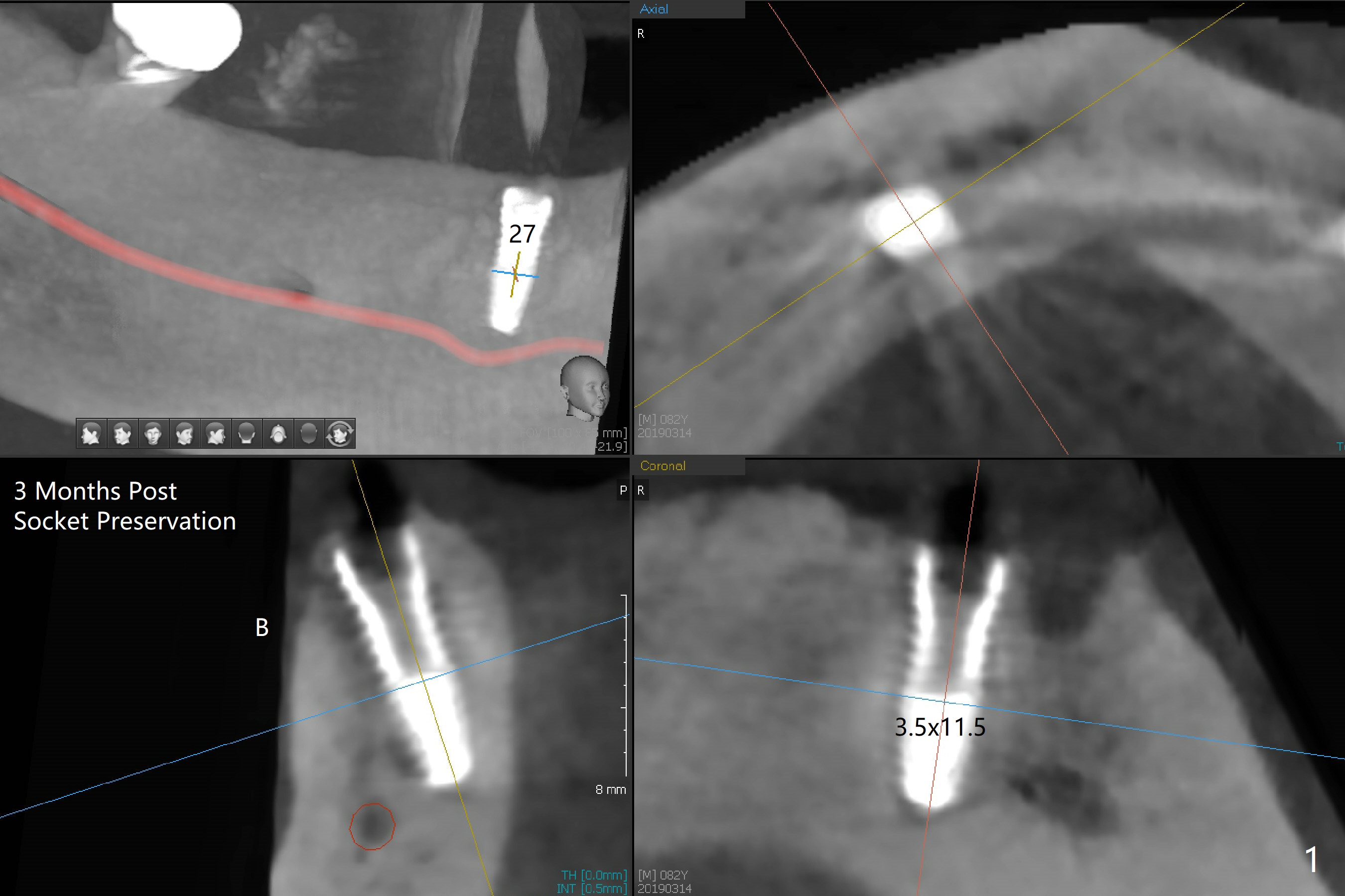
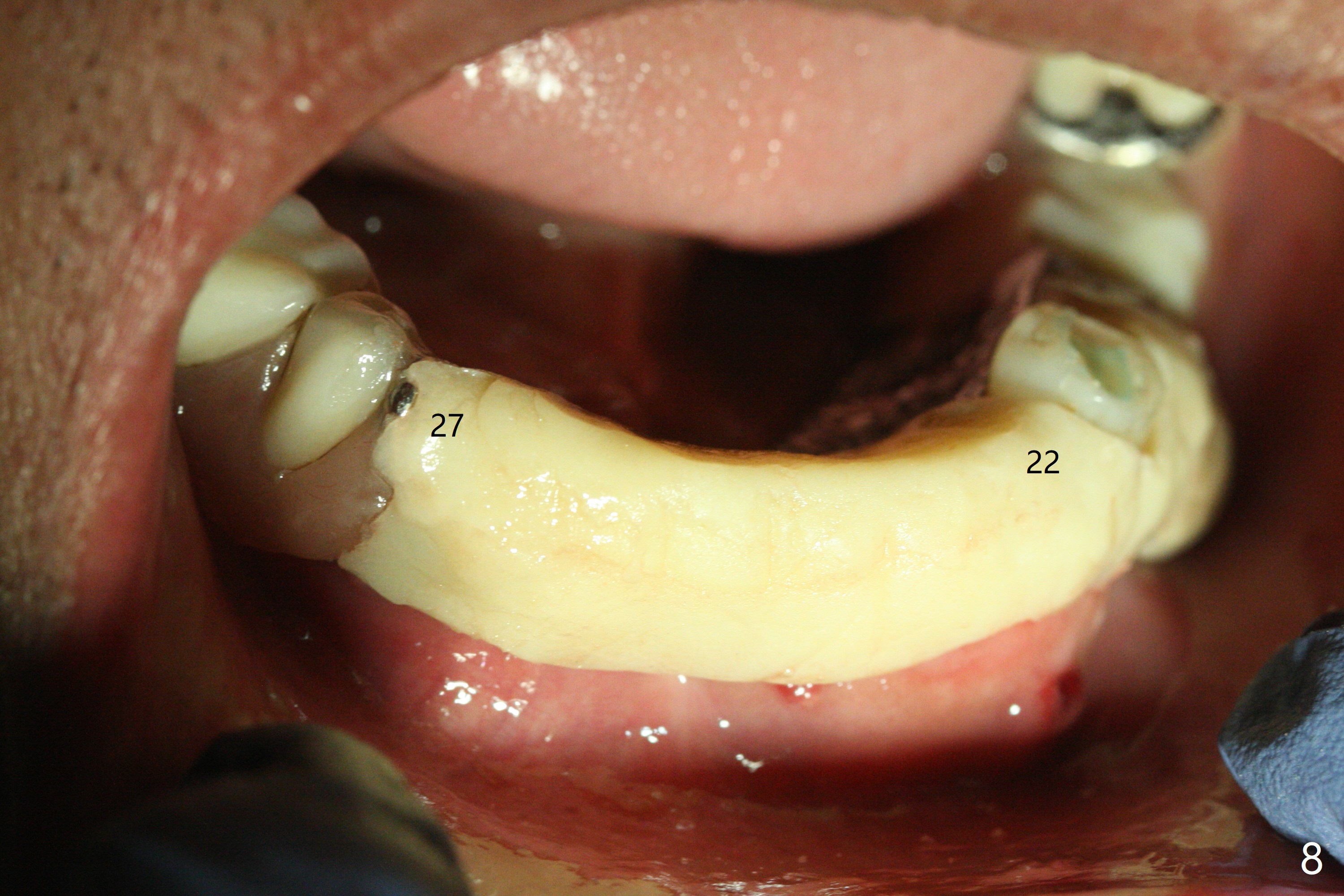
Removable Provisional
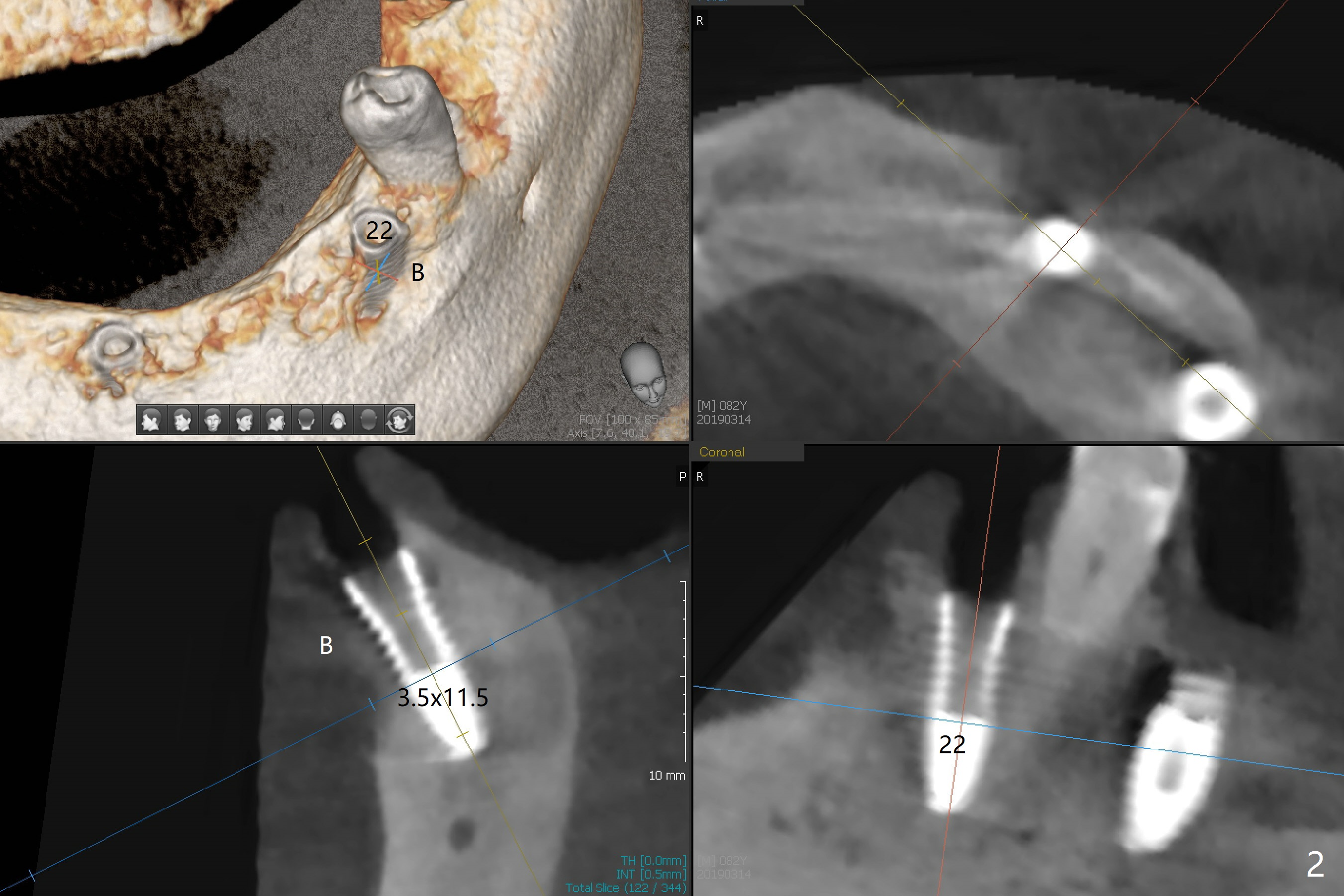
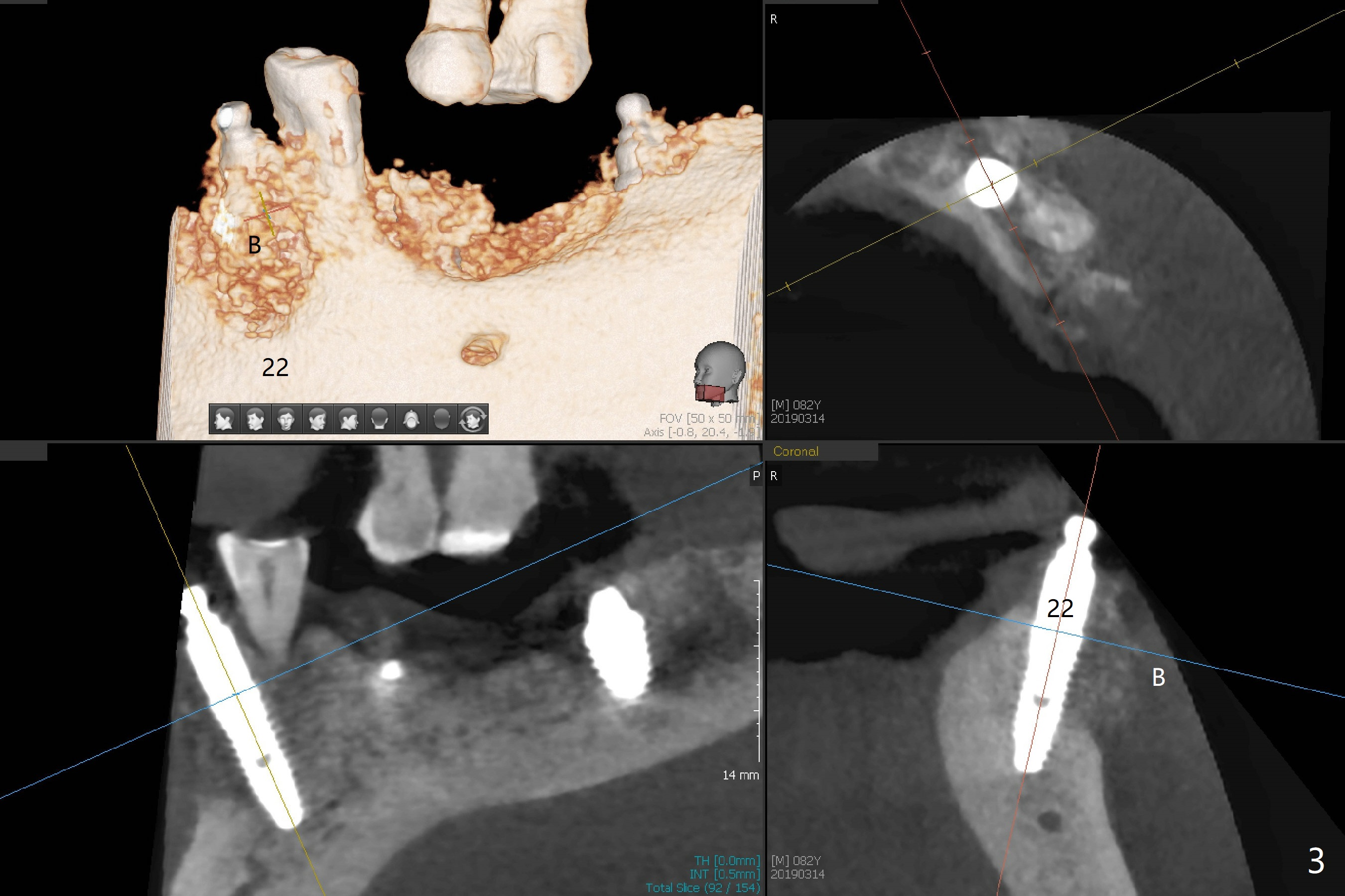
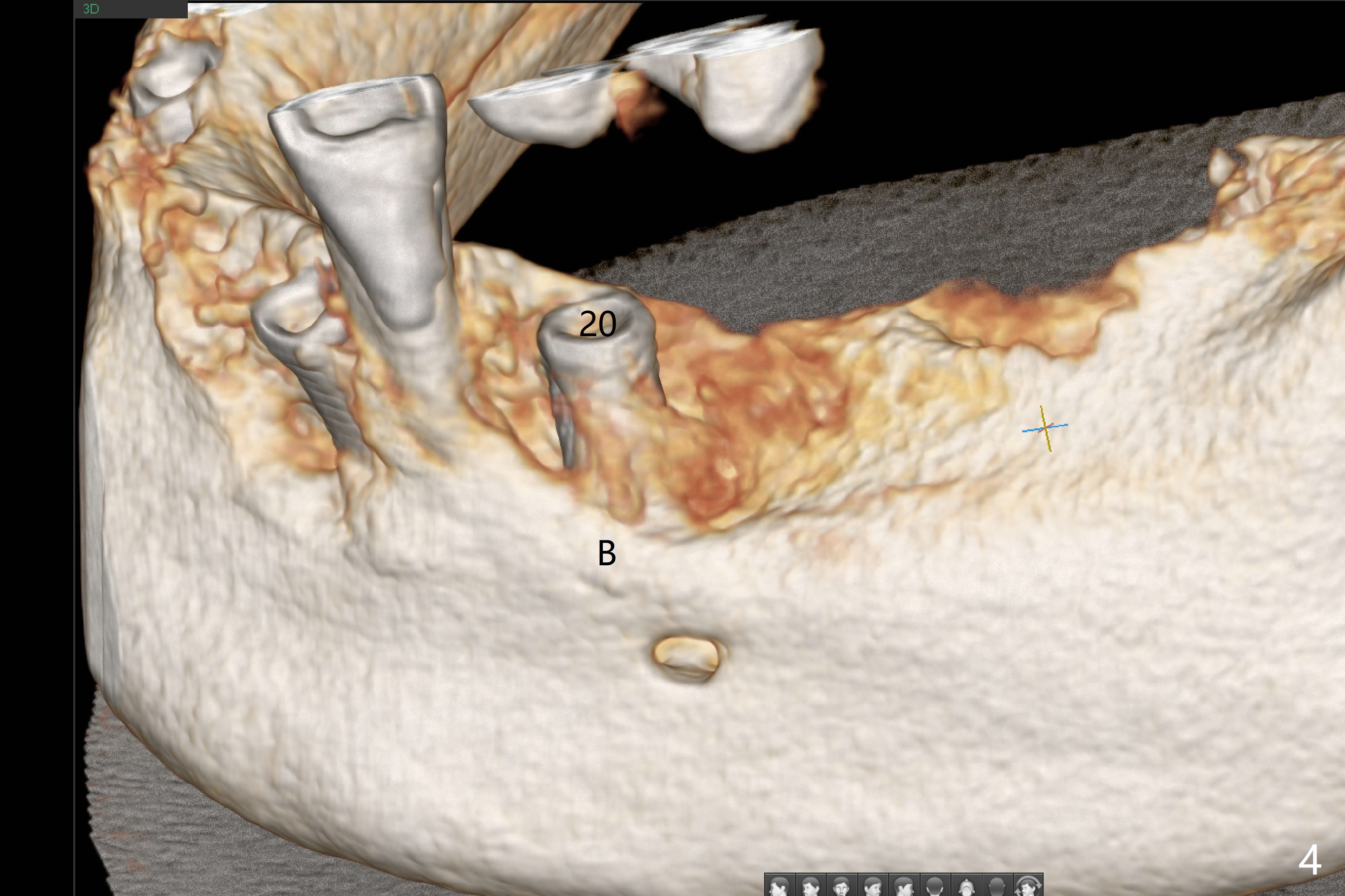
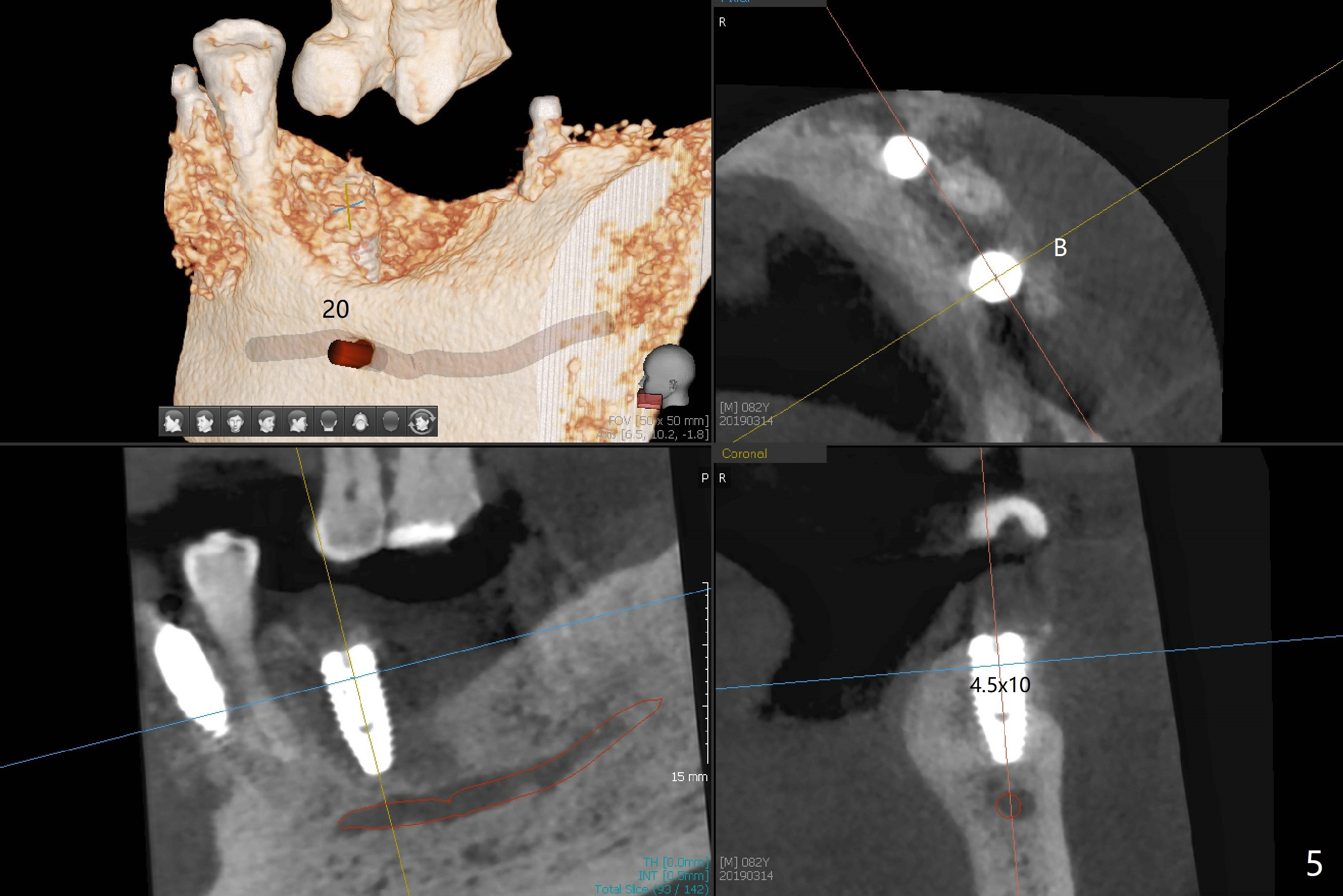
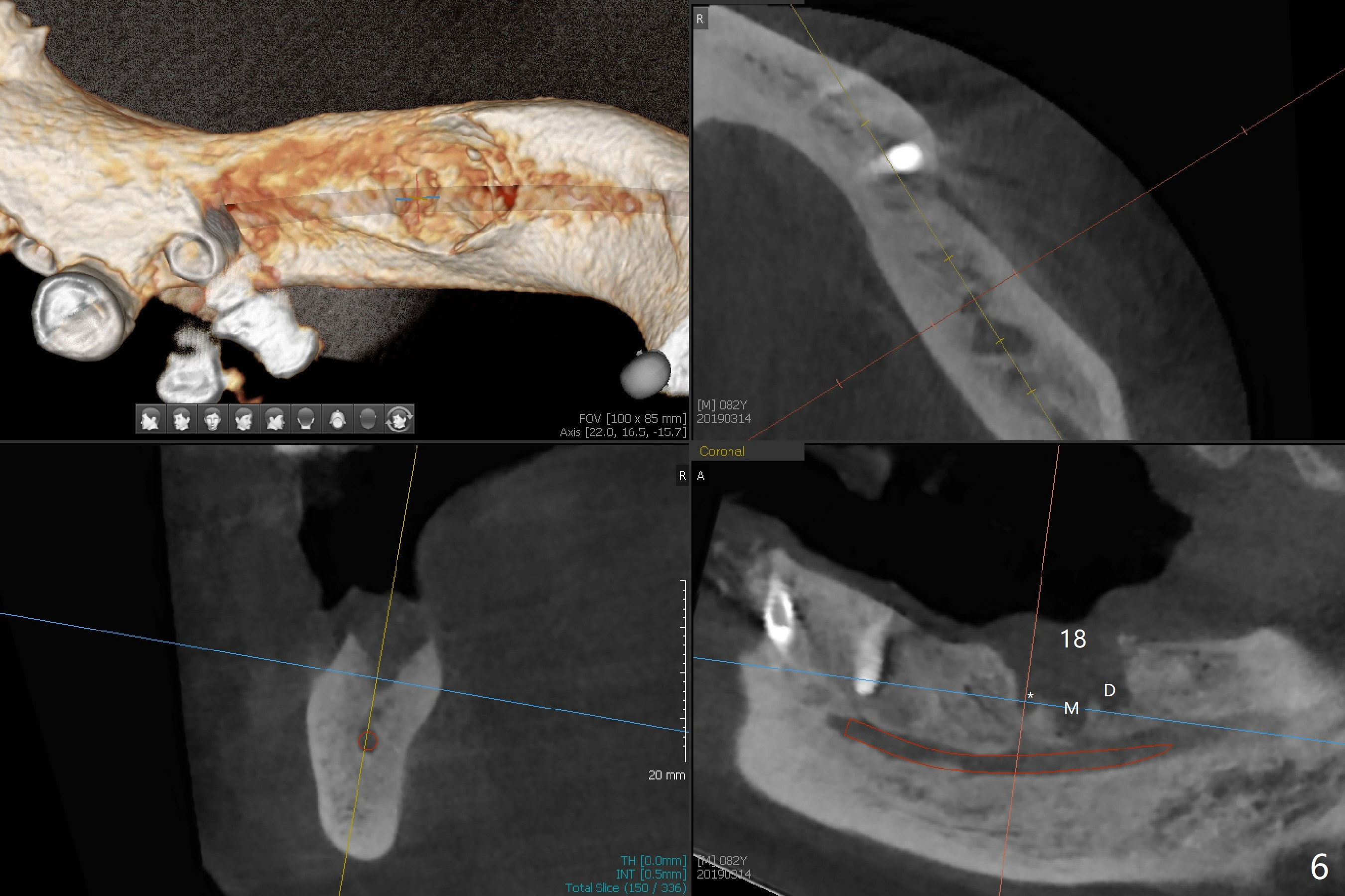
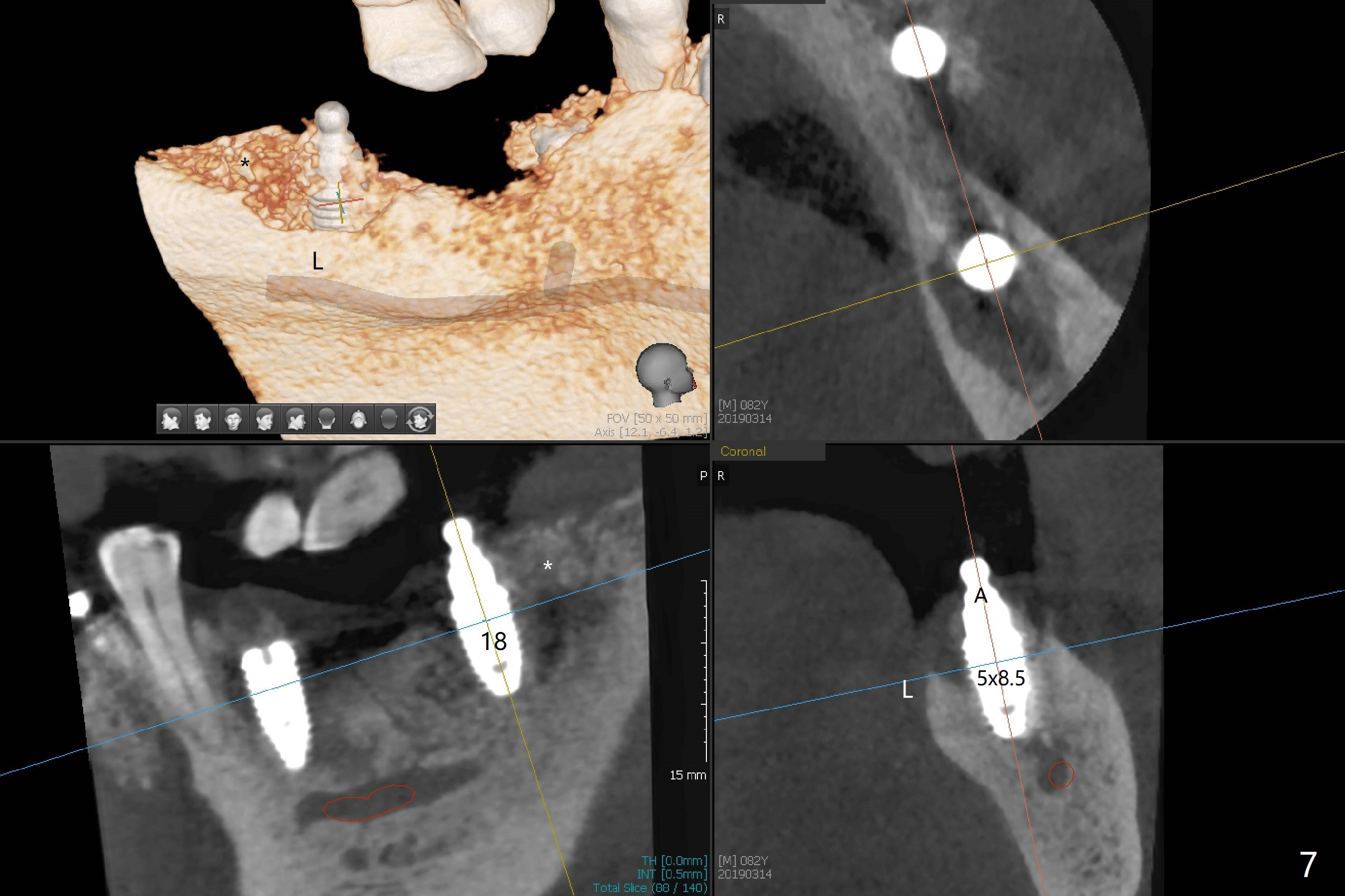
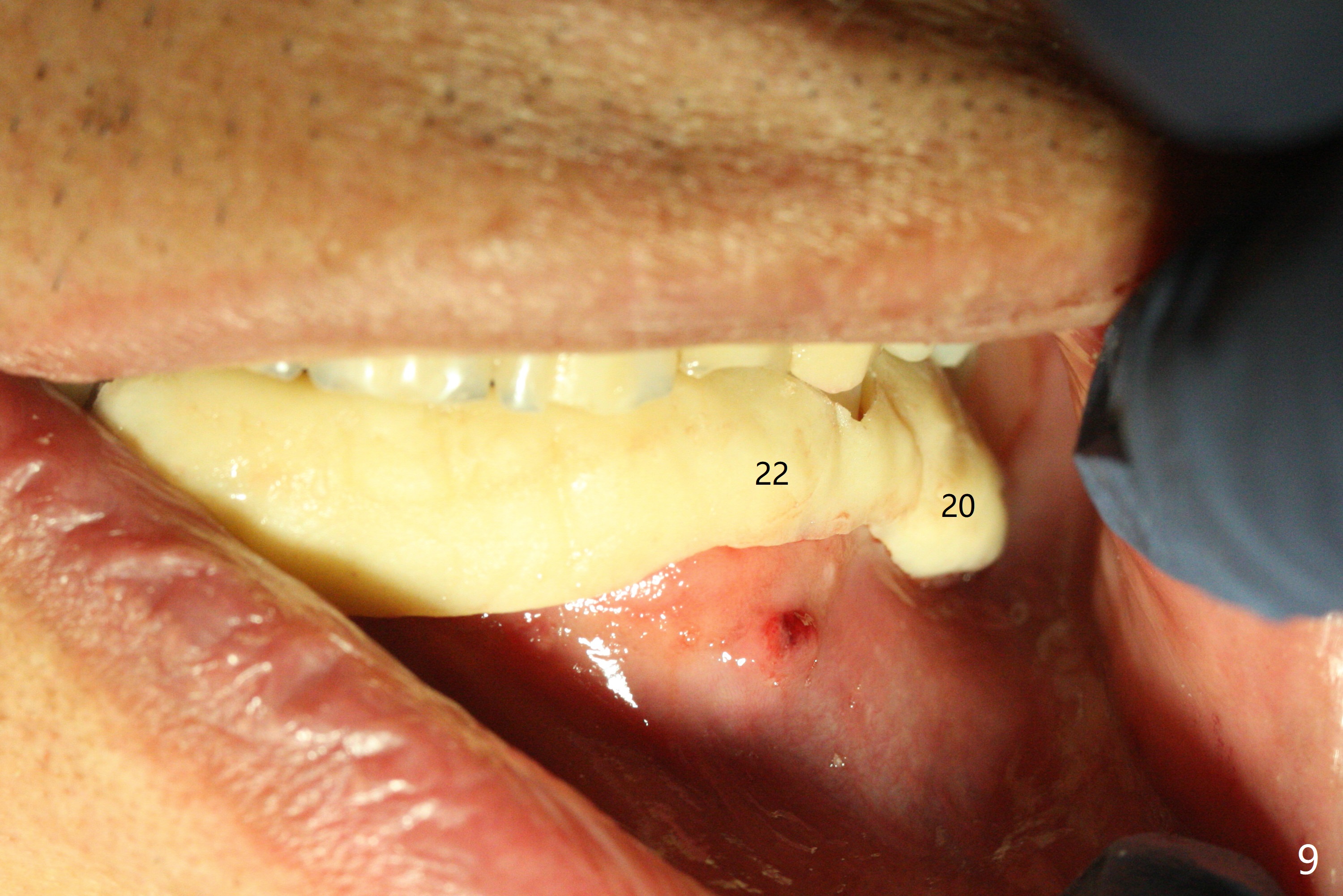
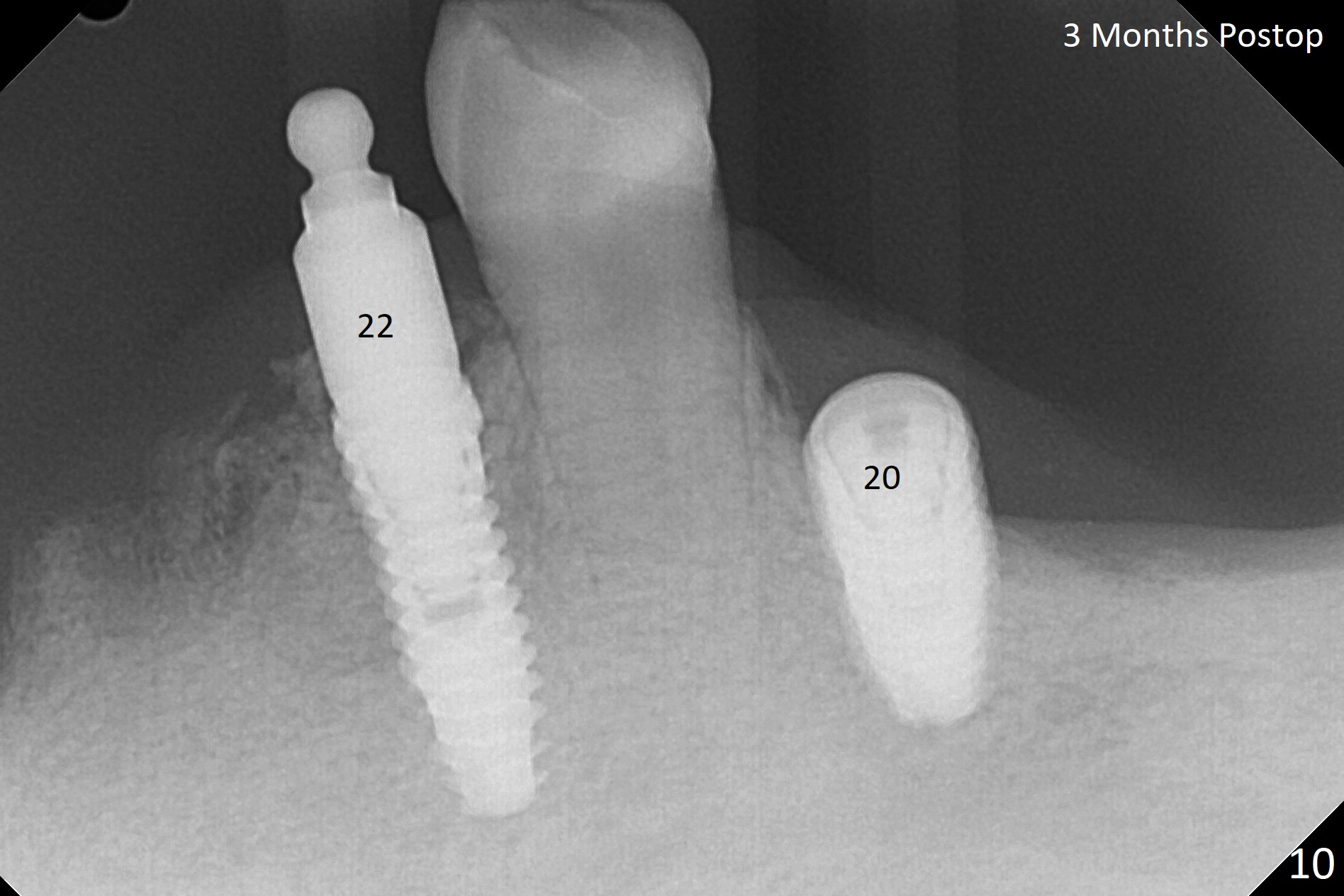
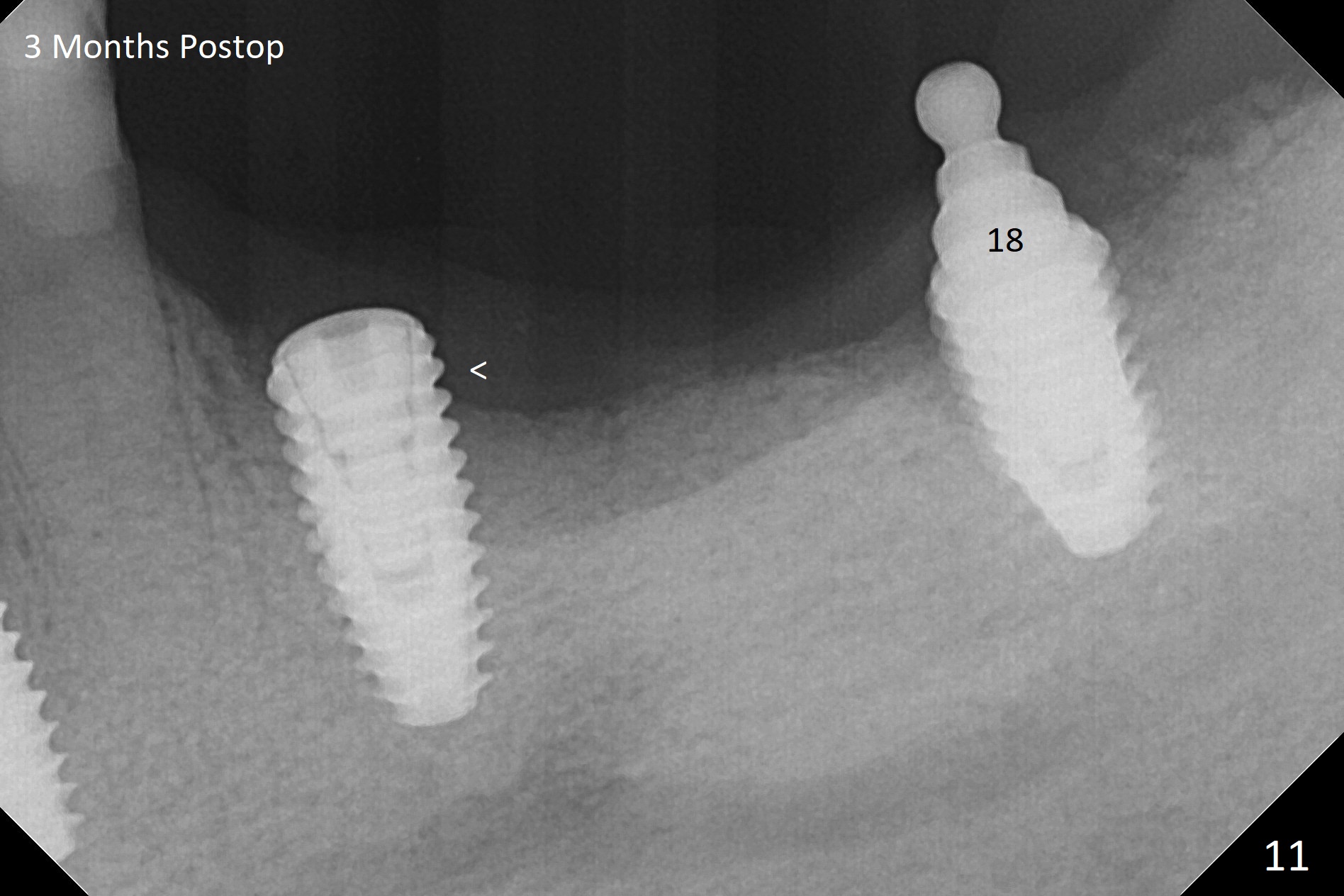
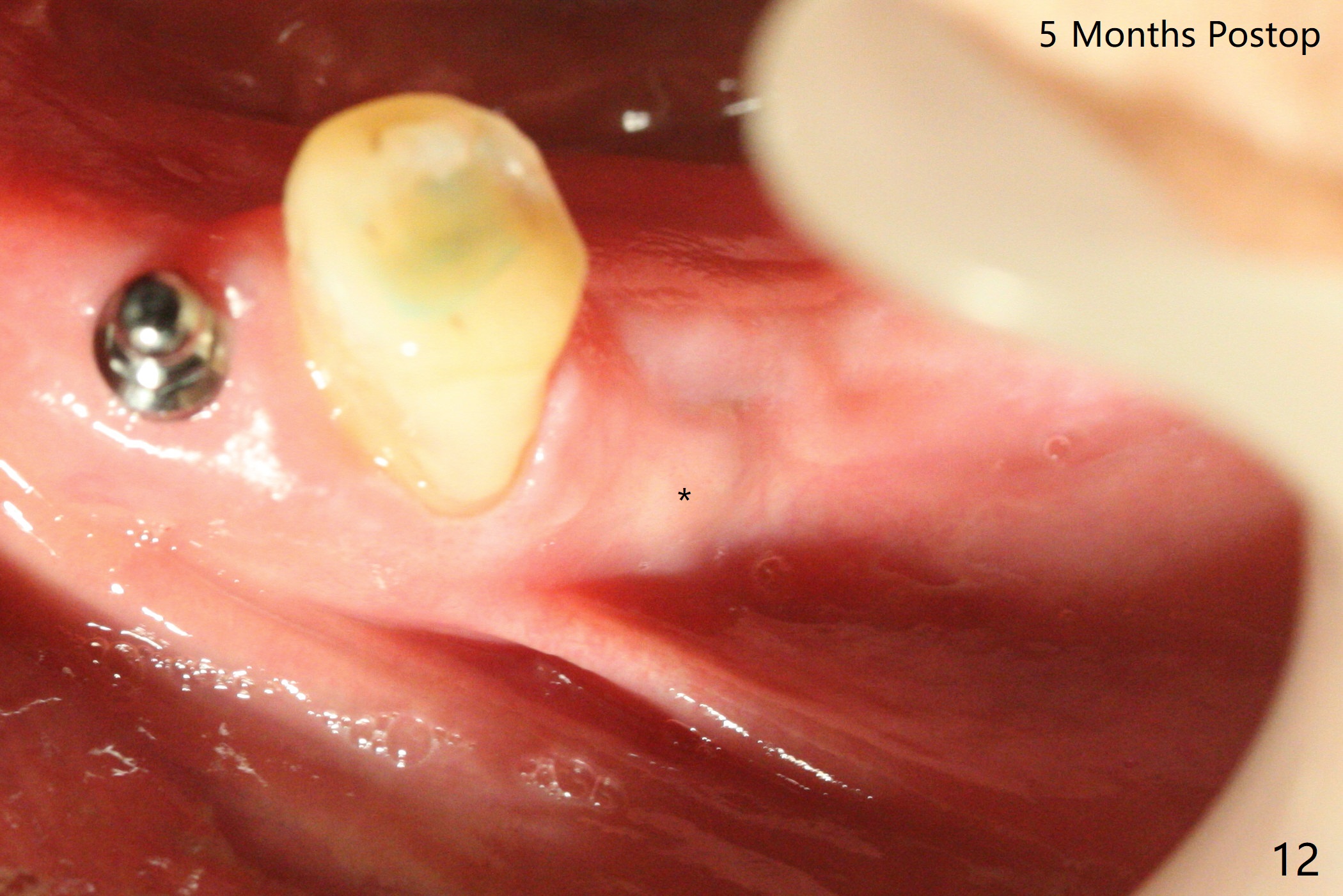
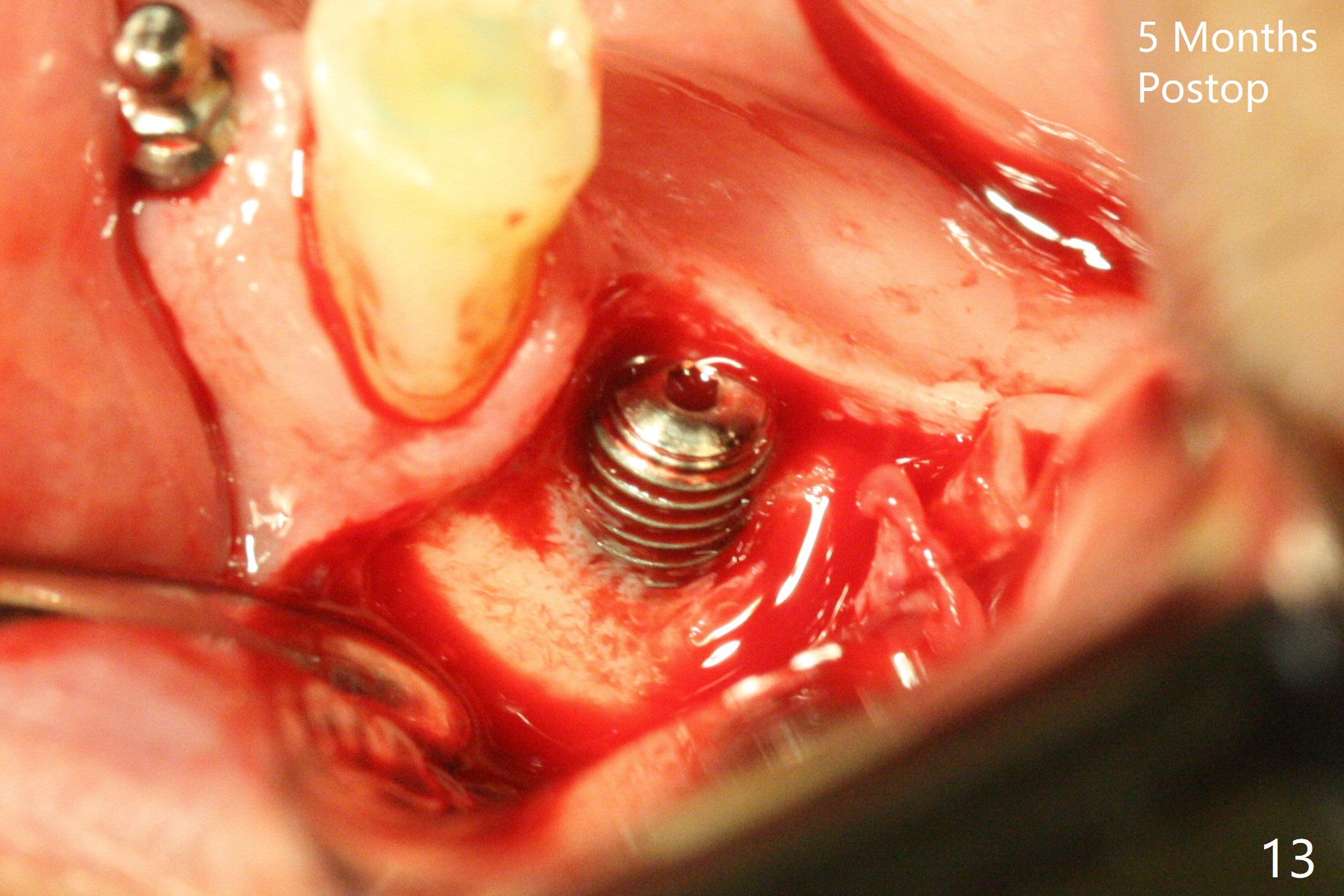
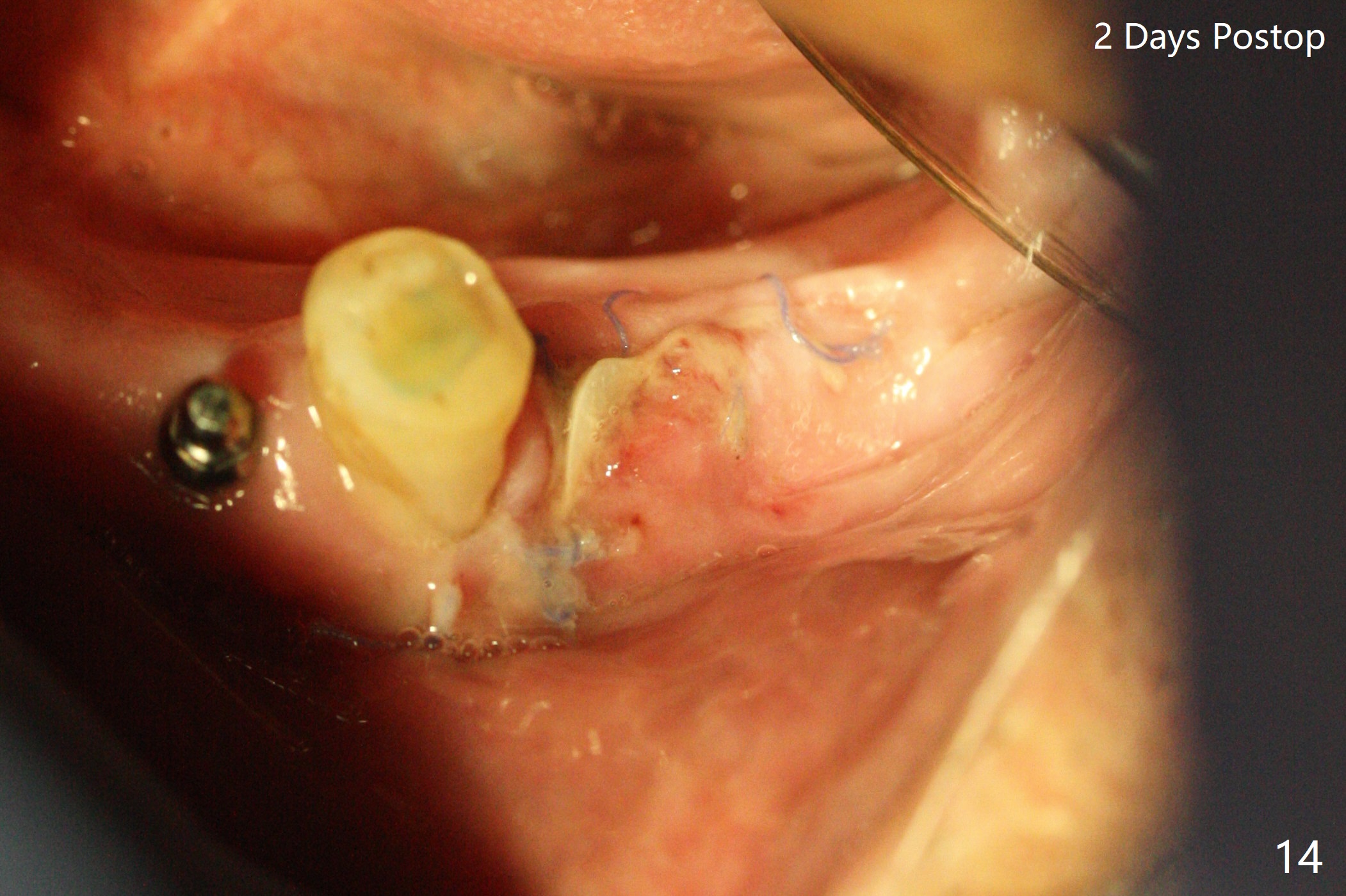
Three months post socket preservation (with buccal plate loss previously), a 3.5x11.5 mm implant is placed at #27 subcrestal (Fig.1). When implants are placed at #22 and 20 (Fig.2,4), threads are exposed buccal (B). Mixture of autogenous bone and allograft is placed to cover the exposed threads (Fig.3,5) following deep placement at #20. For safety, the implant at #20 is buried. Pain control at #18 is poor when initial osteotomy is being established (Fig.6 *), as related to severe infection. Repeated block anesthesia allows to finish implant placement with primary stability; a 3.5x2 mm ball abutment is placed (Fig.7). With placement of 2 other ball abutments at #27 and 22 (Fig.3), the lower existing RPD is converted to a removable provisional (Fig.8). With addition of acrylic, the socket of #20 is covered (Fig.9). There is no apparent bone #20 distal 3 months postop (Fig.10,11 <). Re-graft is needed? The implant at #21 appears immediately subgingival 5 months postop (Fig.12 *). The distobuccal threads are exposed (Fig.13). After decortication, allograft is placed, followed by 6-month membrane. In fact, a shorter and smaller implant should be placed instead. The patient has to wear the RPD for mastication. It would be more painful without it. Later the tissue surface of the RPD is trimmed.
Return to
Lower Arch Immediate Implant,
Prevent Molar Periimplantitis (Protocols,
Table),
Trajectory
Xin Wei, DDS, PhD, MS 1st edition
03/14/2019, last revision
08/25/2019