
,%20sticky%20bone.jpg)

,%20no%20profile%20drill.jpg)
,%20no%20gap.jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Immediate Redo Implant
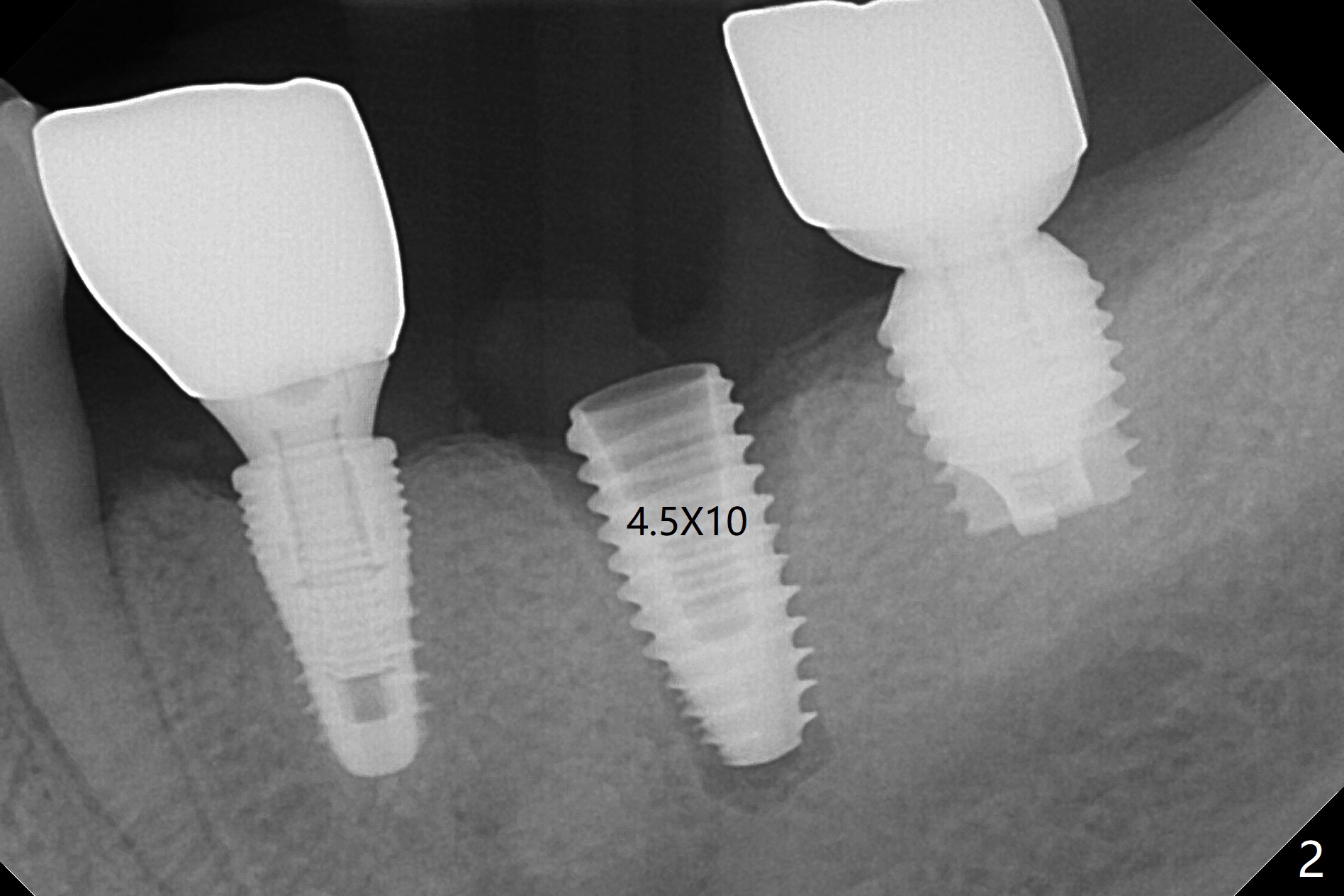
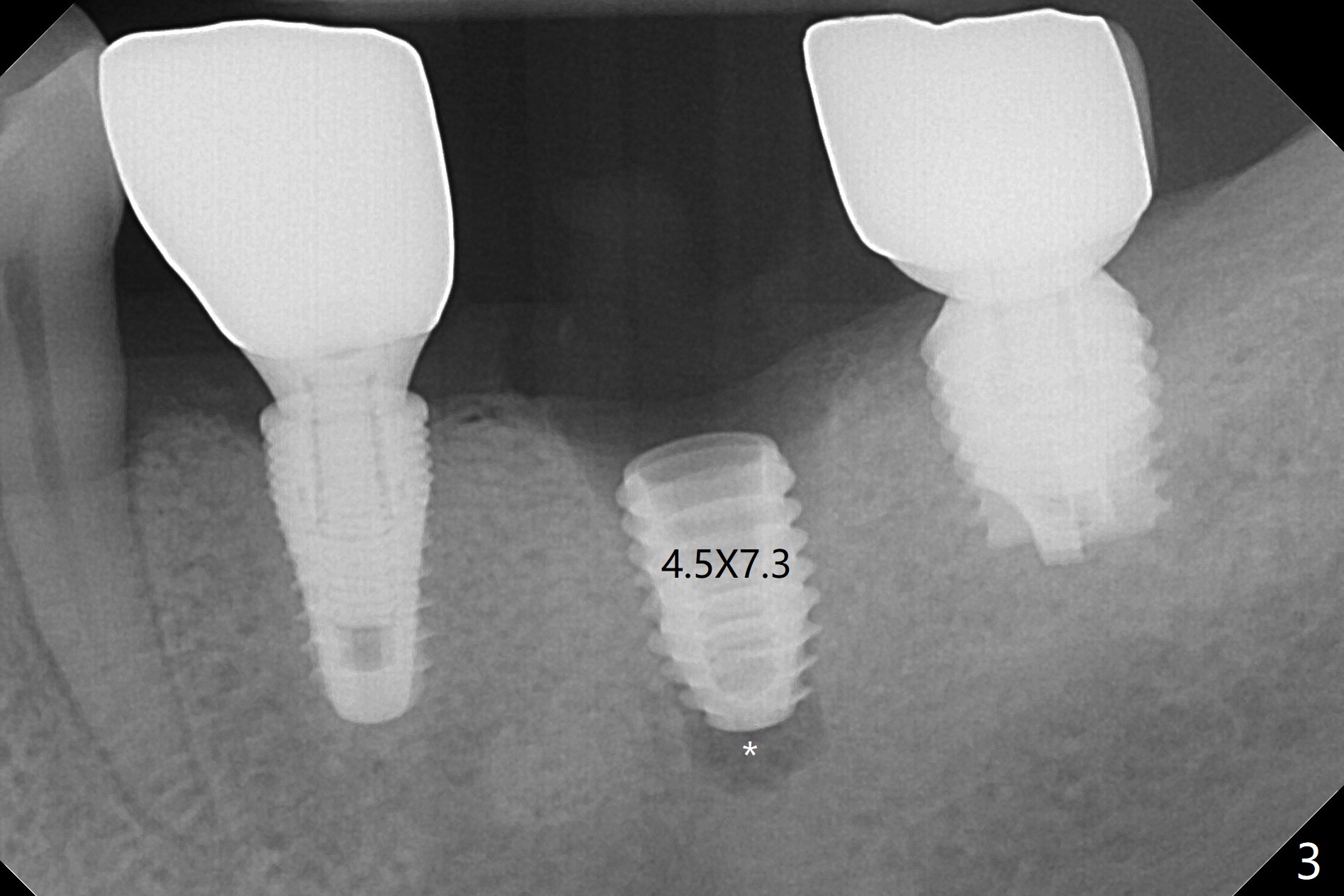
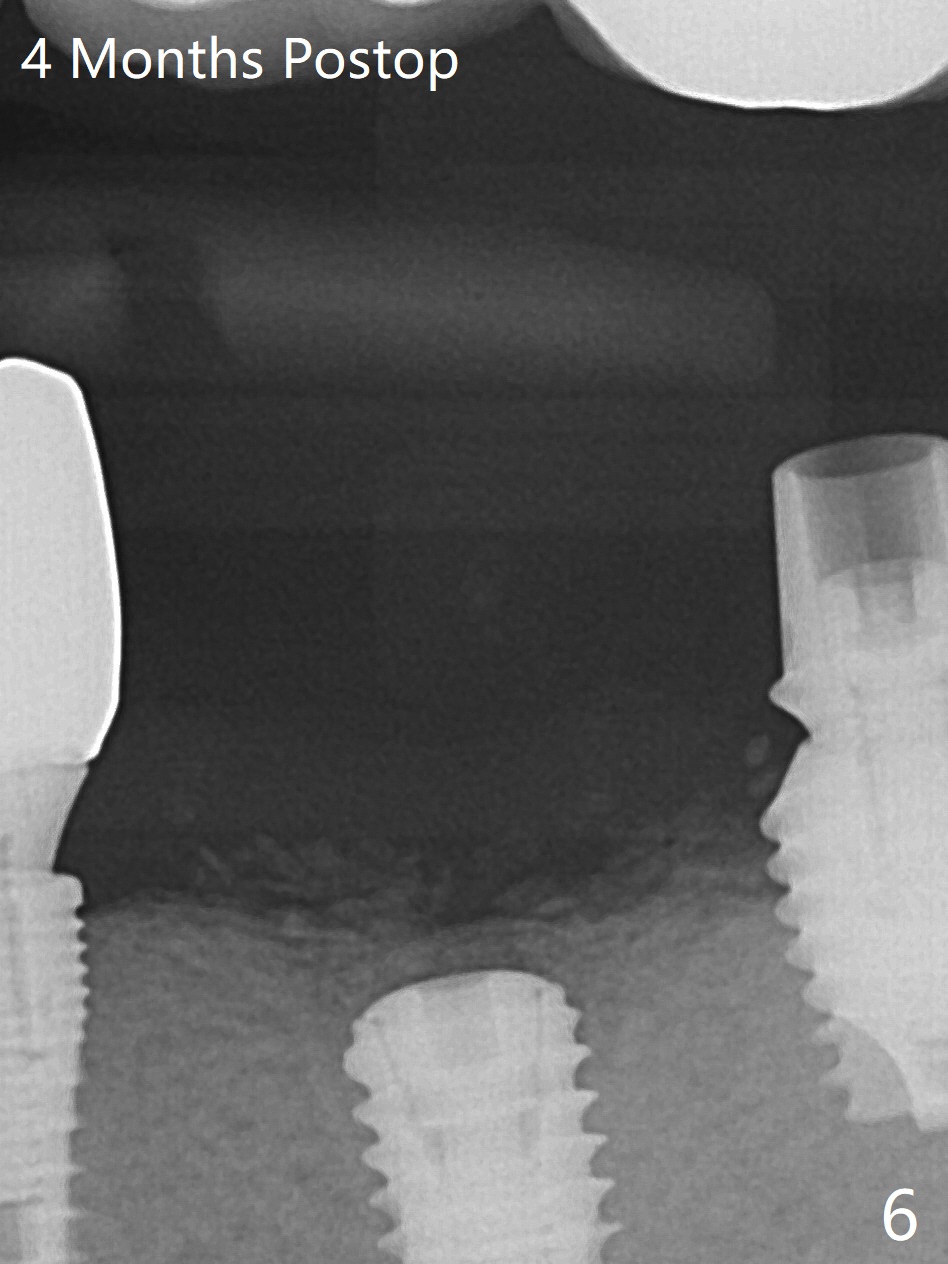
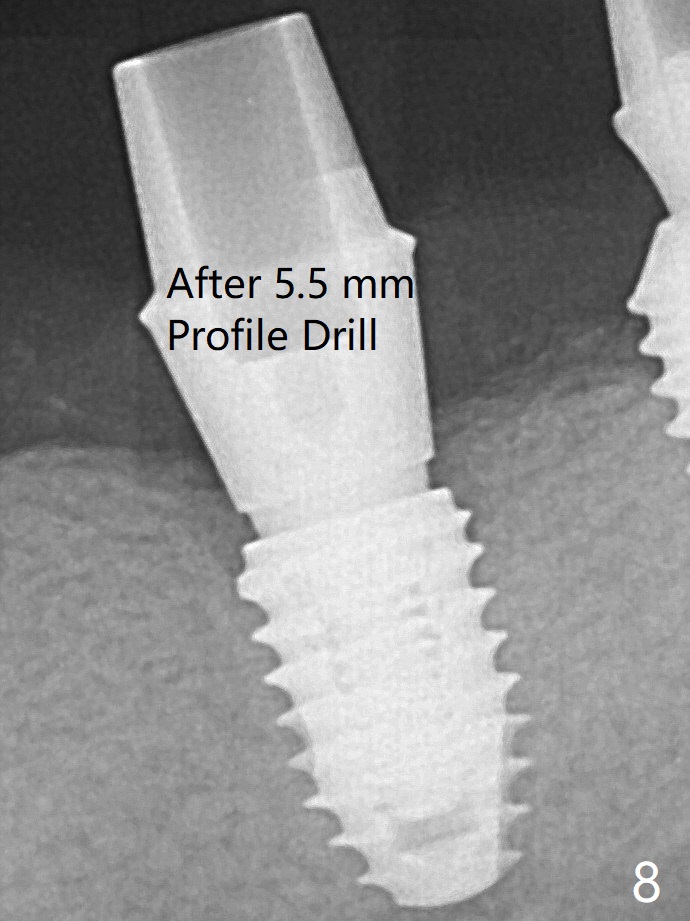
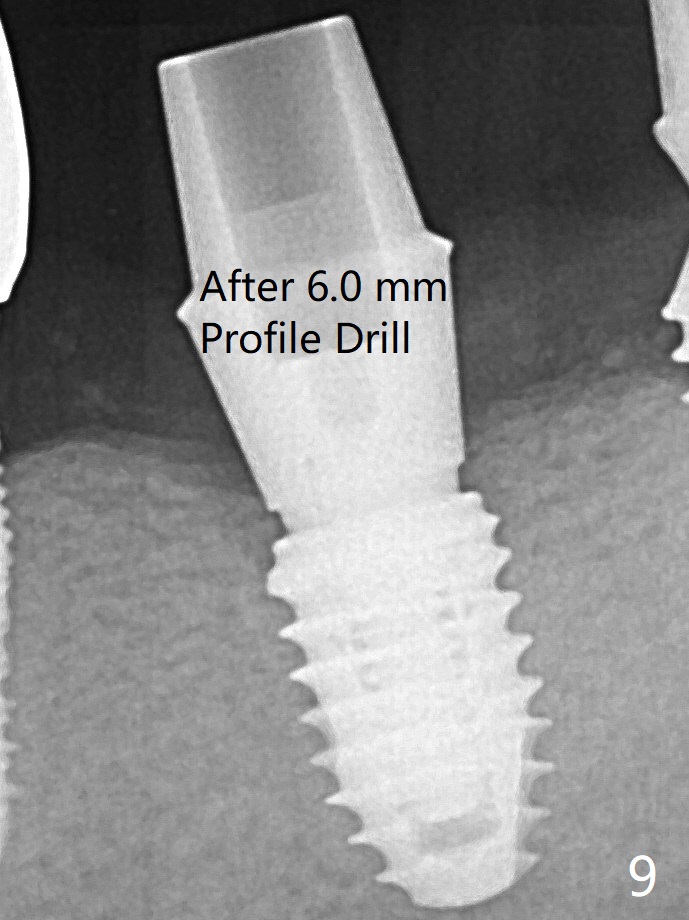
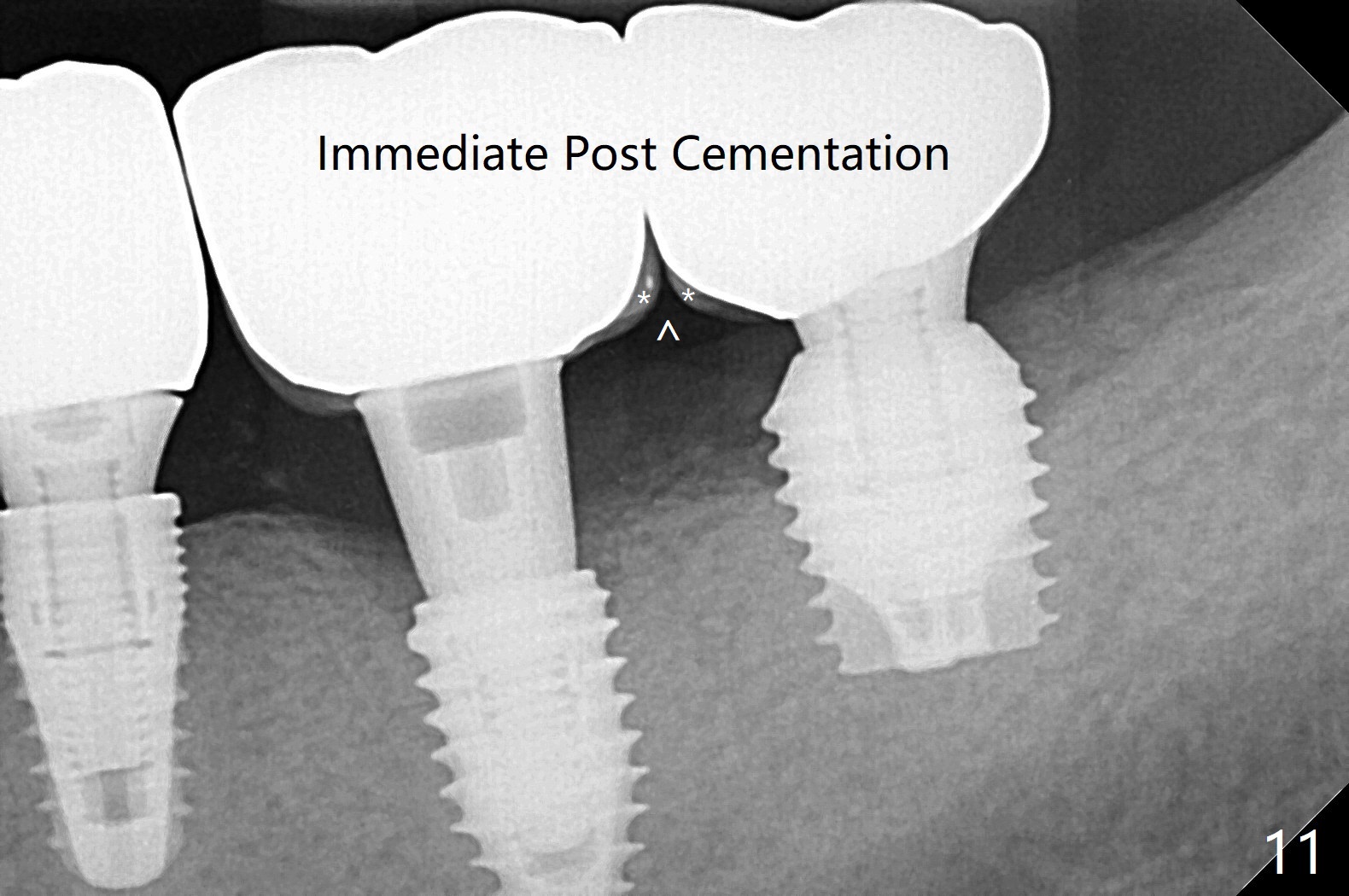
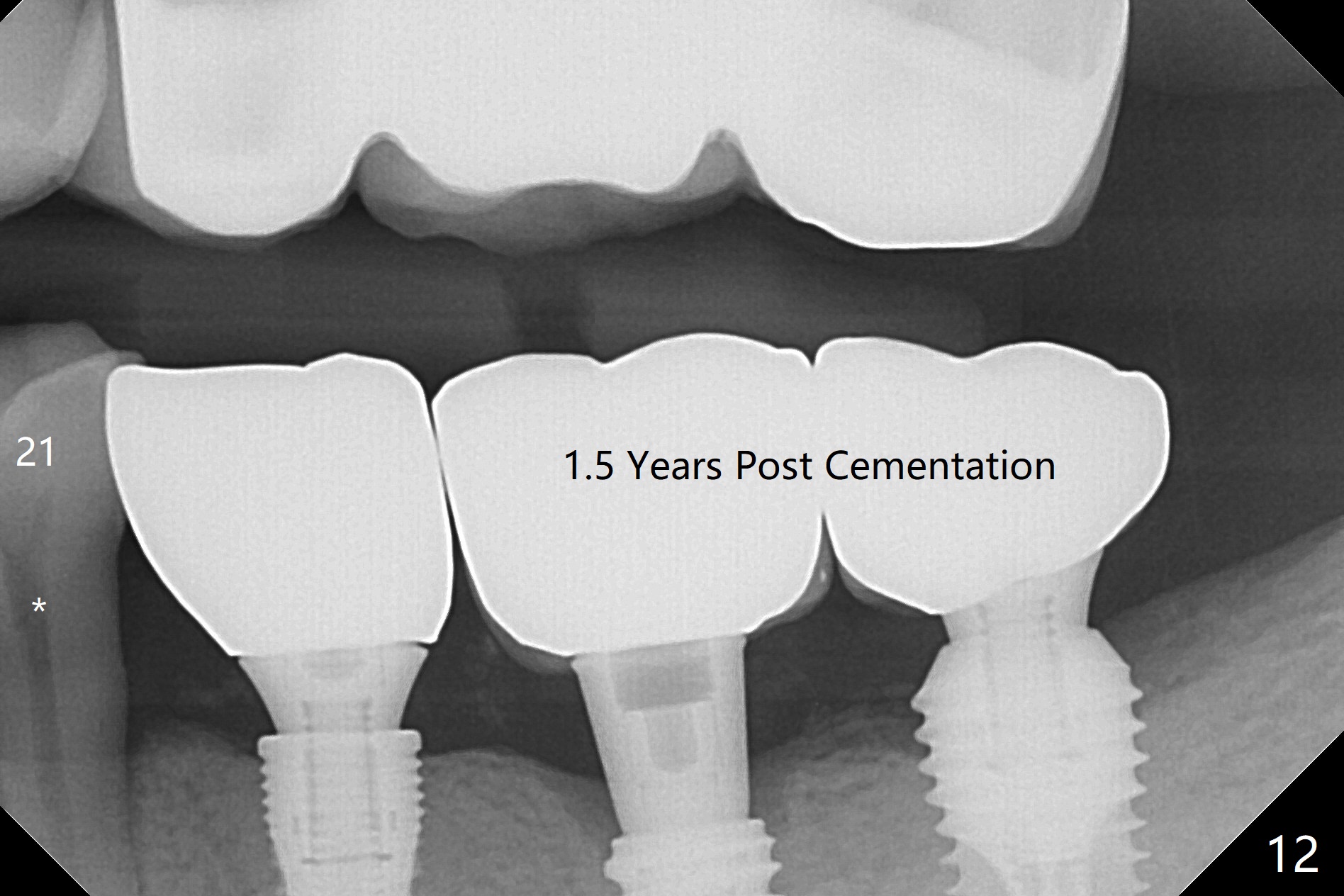
Since there is ~ 2 mm bone apical to the 5x8 mm loose implant at #19 (Fig.1), primary stability is achieved for a 4.5x10 mm dummy IS implant (having better surface treatment than the previous implant) when osteotomy is finished with a 4 mm drill (Fig.2). It is the same associated with a 4.5x7.3 mm definitive one with apical space (Fig.3 *). After depth adjustment to make sure that the implant is subcrestal circumferentially, sticky bone is placed on the top of the implant and around the implant at #18 (Fig.4 *), followed by PRF membranes and suturing with 5-0 PGA and 4-0 Chromic gut suture. Periodontal dressing is applied around the cemented abutment at #18 for additional retention. There is no paresthesia postop. In fact immediate implant redo is fairly safe. The wound heals 1 month postop (Fig.5). There is reorganized bone coronal to the healing screw 4 months postop (Fig.6), which is confirmed in uncovering. One month post uncover, the 6x4 mm healing abutment is found to be loose, suggesting incomplete seating after uncover. A 5.2x4.5(4) mm cemented abutment seems to be incompletely seated (Fig.7). It remains the same after 5.5 and 6.0 mm profile drills (Fig.8,9). A 4.5x4.5(4) mm abutment appears to be completely seated (Fig.10). When the crowns of #18 and 19 are cemented, the gingival embrasure between them is narrow (Fig.11 ^) because of bulky porcelain build-up (*). The tooth #21 with buccal Class V defect (Fig.12 *) seems to have occlusal trauma 1 year 6 months post cementation of #18 and 19. The problems are subsequently taken care of.
Return to Lower Molar Immediate Implant, Trajectory II 29/30 2
Xin Wei, DDS, PhD, MS 1st edition 08/12/2019, last revision 08/15/2021