




|
|
|
|
|
|
|
|
|
|
|
|
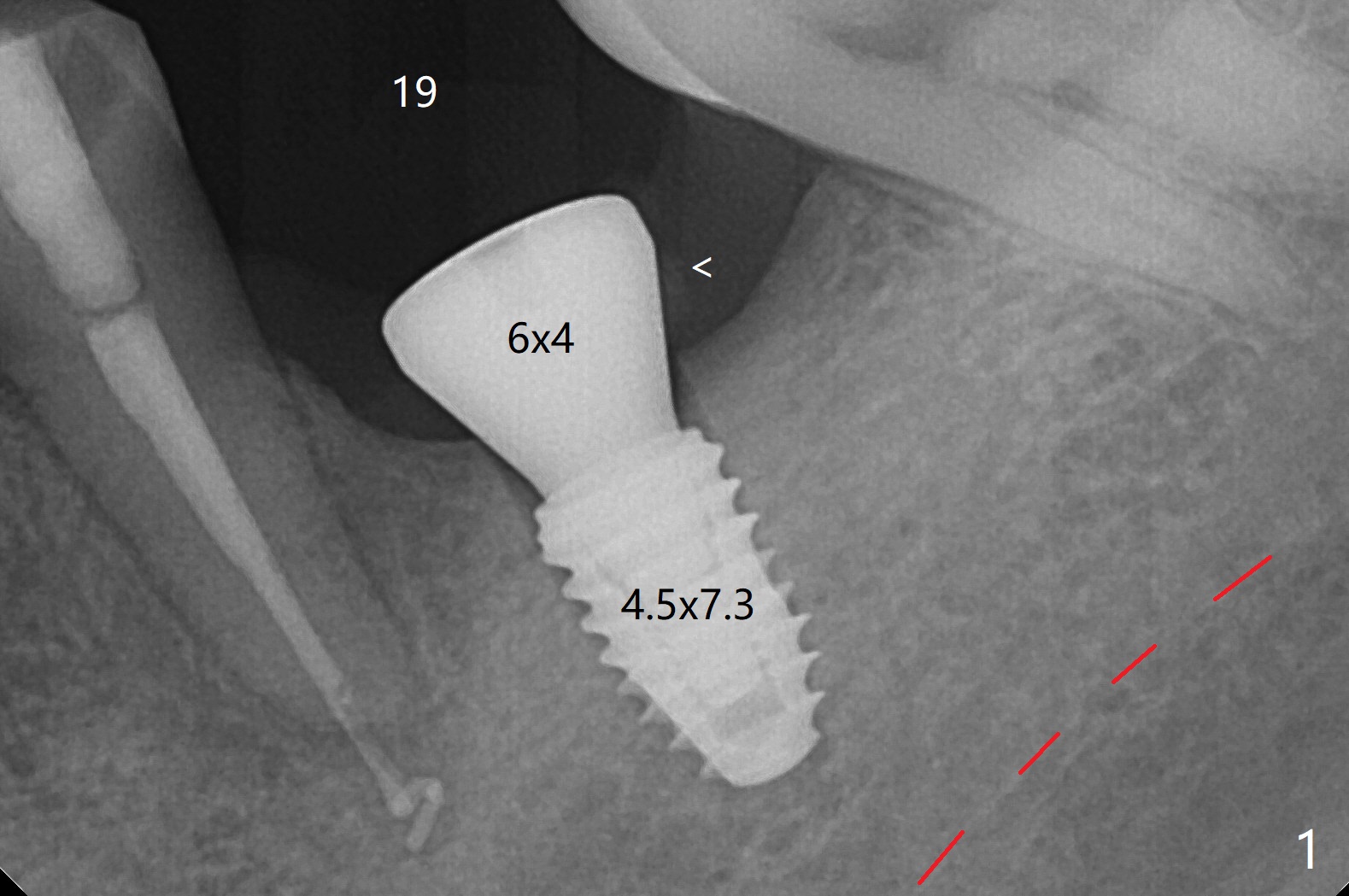
Overprep
Due to Dense Bone
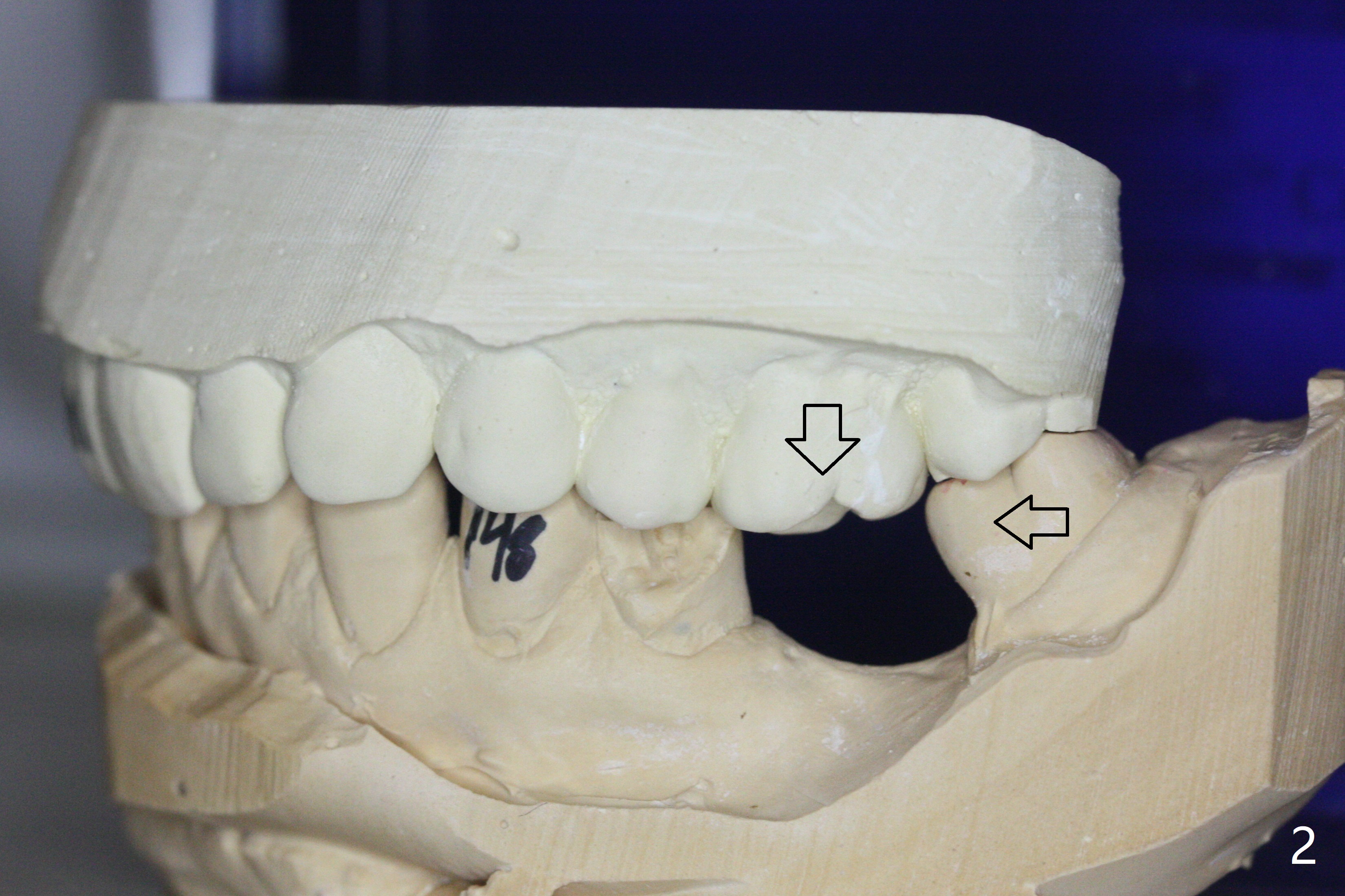
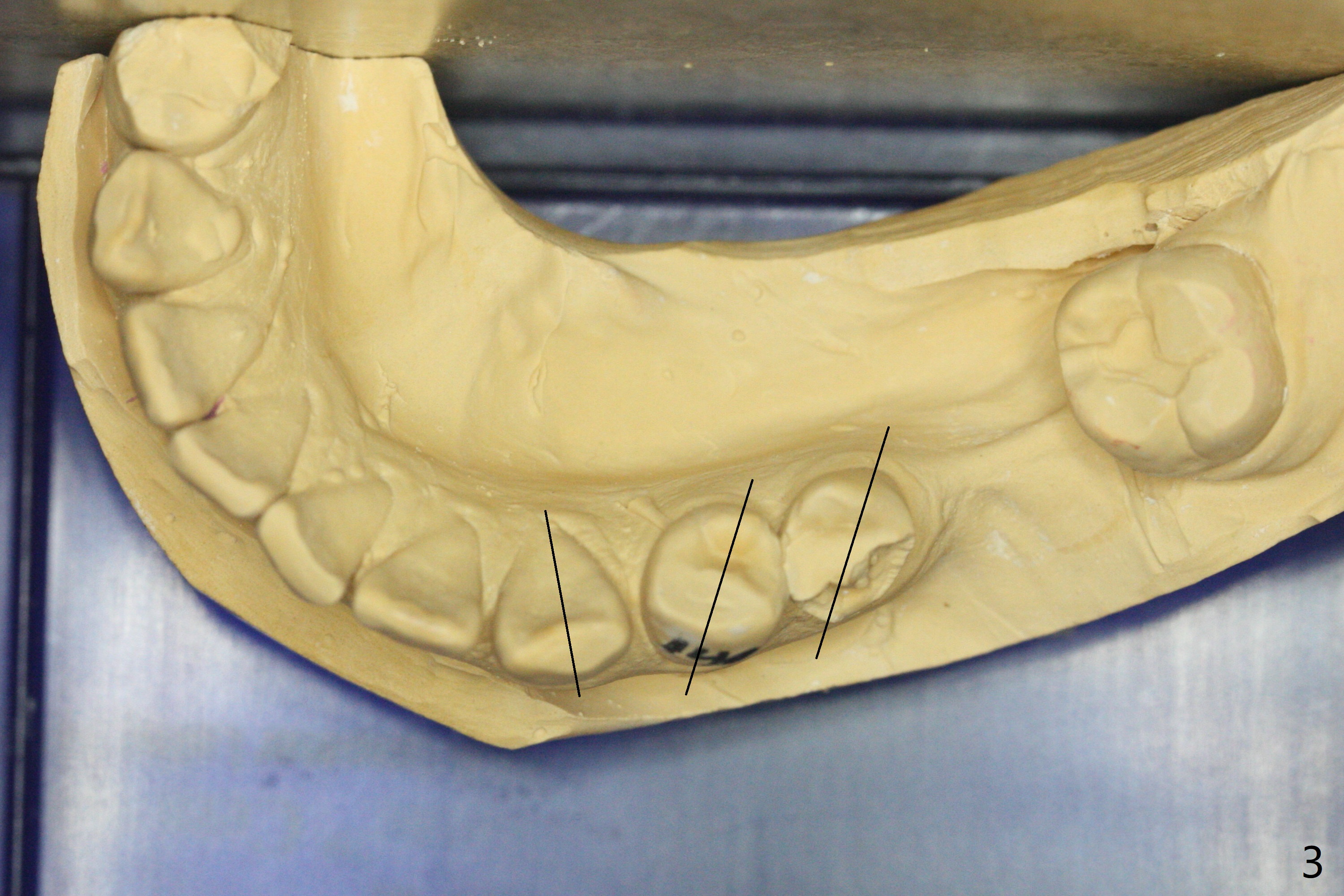
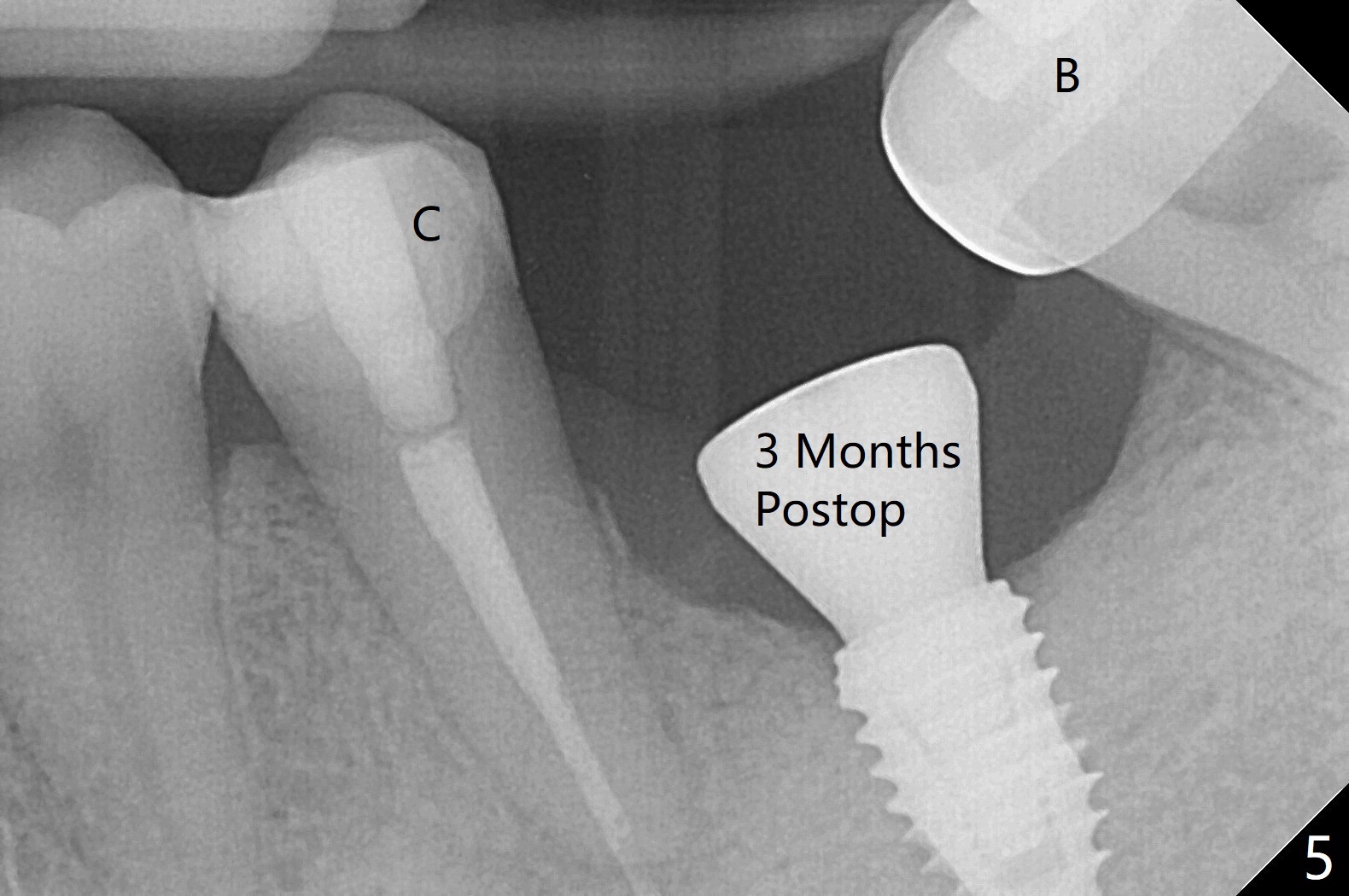
According to drill sequence at #19, the osteotomy is over prepared with the 4.5x8.5 mm last drill. The bone density does not feel so high that warrants use of 5.0 mm cortical tap. The insertion torque is ~ 25 Ncm (Fig.1). When a 6x4 mm healing abutment is placed, the implant does not turn. The distobuccal gingiva is slightly torn; following packing autogenous bone (<), periodontal dressing is applied. In fact the patient suddenly agrees to have limited orthodontic treatment 2 months post #19 implant placement in spite of supraeruption of the opposing tooth (Fig.2 down arrow) and the mesial tilt of the tooth #18 (horizontal arrow). Therefore, the orthodontic intervention will not be so limited. Pay attention to the height of the contour in the lower left quadrant at the time of bracketing (Fig.3 black lines). The implant was not planned to be placed distal enough. Thanks to the multiple diastemata in the lower arch (Fig.3), the planned placement issue is not so striking. The tooth #20 fractured and will need composite build-up before bracketing (Fig.4 * (3 months post #19 implant placement)). A provisional is not fabricated at #19, considering short healing time (Fig.5). But there is no gap between the implant and surrounding bone, as compared to Fig.1. It appears that overprep helps healing. The upper tooth touches the lower bracket when posterior composites dislodge (Fig.6). There is no posterior occlusal contact (Fig.7). There is anterior separation (Fig.8) when composite is placed in the palatal surface of the upper anterior teeth (Fig.9). Return to Lower Molar Immediate Implant, Trajectory Xin Wei, DDS, PhD, MS 1st edition 02/06/2019, last revision 07/13/2019